FIGURE 23.1 The BrainLAB® bone anchored reference array for intraoperative navigation is fixed to the scalp with a self-tapping screw. The bicoronal flap is elevated.
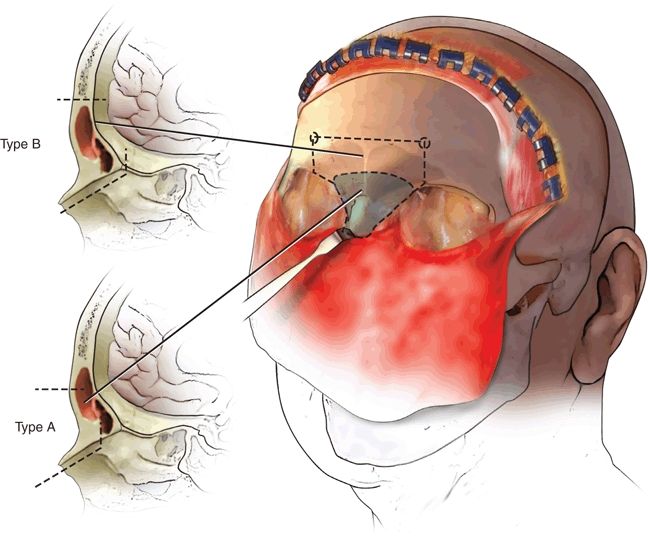
FIGURE 23.2 The outline of the nasofrontal segment depends upon the anatomy of the frontal sinus, the size of the tumor, and the location with regard to the intracranial extension. Type A osteotomy leaves the posterior wall of the frontal sinus intact to be removed as a second step, whereas type B osteotomy includes the posterior wall in a one-step procedure. (Adapted from an illustration courtesy of Professor Dan M. Fliss.)
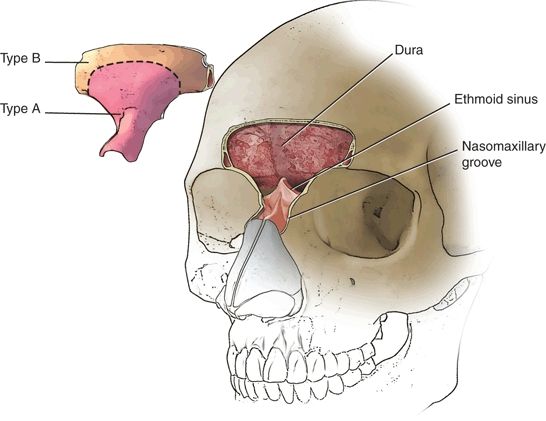
FIGURE 23.3 Osteotomies are performed across the frontal bone, down to and along the roofs of the orbit, medial wall of the orbit into the nasomaxillary groove just anterior to the lacrimal crest. The lacrimal duct is removed from its canal. (Adapted from an illustration courtesy of Professor Dan M. Fliss.)
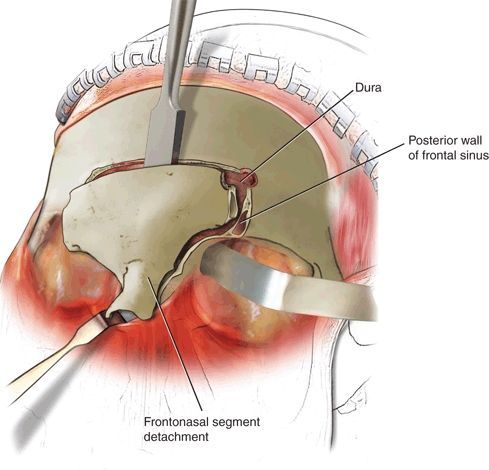
FIGURE 23.4 Following separation just anterior to the crista galli using a chisel, the frontonasal segment is detached providing direct vision to the nasal and sphenoethmoidal extracranial part of the tumor. Further removal of the posterior wall of the frontal sinus allows exposure of the planum sphenoidale and intracranial neurosurgical dissection. (Adapted from an illustration courtesy of Professor Dan M. Fliss.)
Resection of a tumor mass creates a large dead-space defect with communication between the sterile intracranial space and the sinonasal cavity. Satisfaction regarding functional and cosmetic outcome always depends as much on the reconstruction as it does on the tumor resection. Dural defects resulting from intradural tumor involvement must be closed to restore a water- and airtight barrier between the intracranial contents and any communication with the sinonasal cavity or nasopharynx to avoid a CSF leak, pneumocephalus, or meningitis. Free fascia is the standard, harvested from fascia lata, pericranium, or the superficial temporalis fascia. The first layer is adapted and sutured to the edges of the resected dura. Further overlapping sheaths are meticulously applied and sealed with fibrin glue intracranially under the bone level between the lateral resection borders of the planum sphenoidale, orbital roofs, and frontal cranial vault. An additional collagen sponge coated with fibrinogen and thrombin coagulation factors (TachoSil, Nycomed, Denmark) is glued over the superficial fascia layer toward the sinonasal cavity, which reaches from the exposed frontal lobes up to the clivus (Fig. 23.5A–D).
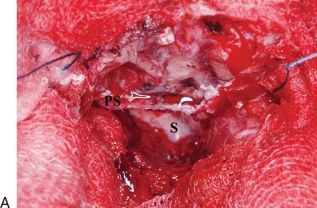
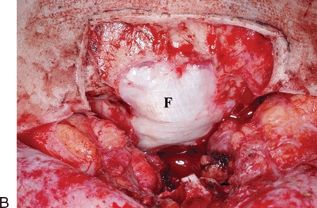
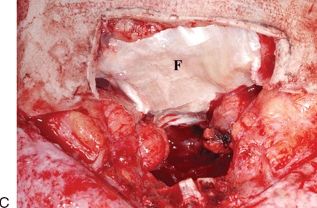
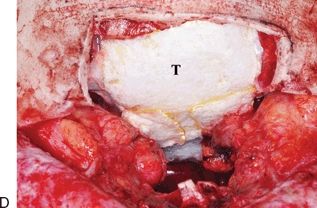
FIGURE 23.5 A–D. Dural repair. A. Defect resulting from intradural tumor resection, showing posterior wall of the sphenoid sinus (S) and planum sphenoidale (PS). B. First layer of fascia lata (F) is adapted and sutured to the edges of the resected dura. C. Further overlapping layers of fascia lata (F) are applied over the bony borders of the resection. D. An additional collagen sponge (T) coated with fibrinogen and thrombin coagulation factors (TachoSil®, Nycomed, Denmark) is glued over the superficial layer of fascia toward the sinonasal cavity, which reaches from the exposed frontal lobes up to the clivus. (Adapted from an illustration courtesy of Professor Dan M. Fliss.)
Significant osseous defects are likely to produce functional disturbances or aesthetic contour deformities such as enophthalmos or diplopia, if left unrepaired. The anatomical restoration of the missing medial wall and floor of the orbit to their original internal shape is therefore crucial to achieve a normal position of the globe. For this purpose, a high molecular resorbable l-lactide-co-glycolide preshaped triangle form orbital plate (Synthes Polymax) is heated in a hot water bath to a malleable state, then contoured to the desired shape before becoming rigid in air temperature again. This self-reinforced resorbable material shows high initial strength and mechanical stability similar to titanium and is consequently suitable for reconstructive procedures in non–load-bearing areas, even if later radiation is planned. A stable bridge of soft tissue should remain after complete degradation within 12 to 24 months.
Finally, I apply a vaseline-coated gauze along the skull base planes to provide additional support against brain pulsation, being removed transnasally after 8 to 10 days. The frontal sinus must be cranialized by removing the posterior table and removing all of the mucosa from the undersurface of the nasofrontal segment. The bone flap is then repositioned precisely to reproduce the original anatomical position and fixed with three-dimensional titanium microplates. Telecanthus should be prevented by bilateral fixation of the canthal ligaments. This is accomplished by passing a nonabsorbable suture through the medial canthal ligament and then guiding it under the nasofrontal segment to the contralateral anterior wall of the frontal sinus. Bilateral tightening of the suture results in medial, downward, and inward traction, thus achieving correct positioning of the canthal ligaments. The last step of the procedure consists in the application of suction drains and closure of the bicoronal incision in layers. In the absence of manifest signs of early postoperative CSF leakage, no lumbar drainage is instituted.
Examples
Case 1: Esthesioneuroblastoma.
This 83-year-old but physically younger and very active former airline pilot was flying a small aircraft, when he suffered a sudden frontal headache during rapid descent. The sinus barotrauma was first treated with topical decongestants and antibiotics, while endoscopic examination manifested a tumor mass in the left nostril that bled easily. Histopathologic findings of the biopsy revealed a high-grade esthesioneuroblastoma Hyams grade III. High-resolution CT and three-plane contrast-enhanced MRI confirmed a considerable tumor extending into the nasal cavity and ethmoid sinus along with intracranial tumor spread and erosion of the medial wall of the orbit. Accordingly, the tumor was classified as Kadish stage C or T4b according to the AJCC-UICC classification, respectively (Fig. 23.6A and B). Further medical investigation revealed a slight stenosis of the subclavian artery with absence of symptoms, hypertension, and cardiac right bundle branch block. Since this circumstance did not appear to be a major risk factor for the development of perioperative cardiac complications, there seemed to be no contraindication for surgery. Complete resection of tumor was achieved with an extended subfrontal approach as described above without complication.

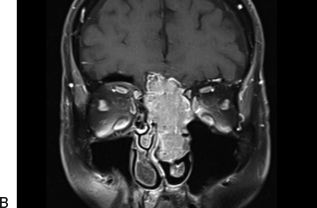
FIGURE 23.6 A and B. Esthesioneuroblastoma Hyams Grade III. A. Preoperative coronal high-resolution CT. B. Contrast-enhanced MR imaging indicating the extent of the tumor into the nasal cavity and ethmoid sinus along with intracranial intradural tumor spread and erosion of the medial wall of the orbit.
Immediately following removal of the nasal packing at postoperative day 8, high-resolution CT and three-plane contrast-enhanced MR imaging were performed and demonstrated complete absence of the tumor (Fig. 23.7A–C
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


