FIGURE 19.1 An example of the potential complications from transfacial incision. An extended lateral rhinotomy approach was used, and the medial canthal region broke down after radiotherapy. Such complications are rare with endoscopic-assisted craniofacial resections.
The majority of the tumors of the cranial base managed with endoscopic-assisted resections are malignant tumors or high-grade meningiomas, and as with other malignancy, the presentation may be related to local, regional, or distant disease. Defining the histology of the tumor and its stage is the key goal of investigations. Finally, treatment is generally multimodal with a combination of surgery and radiotherapy as the mainstay for most lesions. The proximity of critical structures, specifically the orbit, brain, and cranial nerves, dictate the morbidity from curative interventions.
HISTORY
The most important element in accurate diagnosis of sinonasal malignancy is clinical suspicion. The insidious onset of unilateral symptoms, the lack of previous inflammatory sinus disease or rhinitis, and the relative age of the patient (>50 years for tumors compared to <50 years for inflammatory disease) should be key features that prompt exclusion of neoplasia as a cause for a patient’s symptoms. Although the presentation can be with regional symptoms (mass in the neck, orbital changes, diplopia, epiphora or cranial nerve dysfunction) and/or distant metastasis, this is relatively uncommon for most tumors, and the more common presenting symptoms (nasal obstruction, bleeding, discharge, and hyposmia) are local. These symptoms share common presenting complaints of patients with inflammatory sinonasal disease, which again highlights the importance of initial clinical suspicion. Unilateral eustachian tube dysfunction can also occur. Gross macroscopic changes to the mucosa of the hard palate or the skin are uncommon in developed countries. True involvement of the cavernous sinus by malignancy is generally a contraindication to surgery and curative treatment. Involvement of the proximal trigeminal nerves or the other upper cranial nerves should be evaluated. Numbness of the palate and midface dysesthesia are the signs of involvement in the pterygopalatine fossa and V2 involvement in the orbital floor or the roof of the maxillary sinus. Along with asking about orbital symptoms (visual acuity changes, diplopia, and displacement of globe), the inclusion of epiphora is important as this is an anterior limit often missed and needs to be addressed via a transfacial approach.
General health, nutrition, smoking status, bleeding risks, and prior nasal/sinus and cranial procedures should also be noted.
PHYSICAL EXAMINATION
The evaluation of a patient with skull base neoplasia should include the limits of the tumor. Superiorly, the involvement of the dura and brain parenchyma is a radiologic assessment in most patients. Inferiorly, the palate should be evaluated to see whether a total maxillectomy is necessary. Anteriorly, the lacrimal sac and premaxillary tissue should be evaluated bimanually via the gingival buccal sulcus. Laterally, above the orbital floor, signs of restricted ocular movements, conjunctival congestion, and orbital displacement are signs of involvement of a space-occupying tumor. The presence of trismus is an important sign that the masticator space/pterygoid muscles are involved.
Endoscopic examination reveals a mass within the nasal cavity (Fig. 19.2). Preoperative endoscopic examination can be useful to inspect for uninvolved areas of the paranasal sinuses. Many lesions appear extensive on imaging, but they are predominantly exophytic lesions with only a small area of invasion. If the lesion is unilateral, then assessment of the contralateral septum and sphenoethmoidal recess can greatly assist surgical planning. Look for evidence of prior surgery on the septum, sinus, or turbinates. The local reconstructive options available should be noted on examination. Examination of the neck for cervical lymph node metastases is important as these are not always accurately assessed on imaging and may provide an easy route for tissue diagnosis.
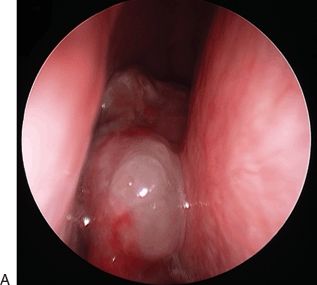
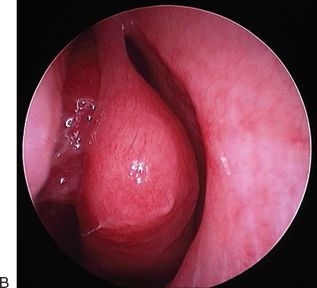
FIGURE 19.2 The classic endoscopic appearances of a SCC (A) and an olfactory neuroblastoma (B).
INDICATIONS
Skull base pathologies requiring endoscopic-assisted surgery are neoplasms: primarily malignant tumors of the paranasal sinuses (Fig. 19.3A). Some intracranial lesions such as atypical/aggressive meningioma are also addressed (Fig. 19.3B). The general principle of surgical access is important here. If the surgical approach crosses the axis of critical neural or vascular structures, then an alternate route should be considered.
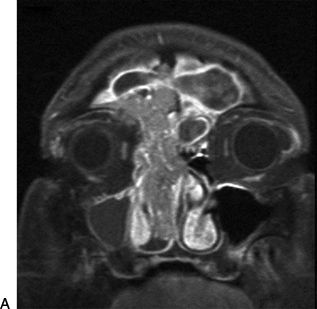
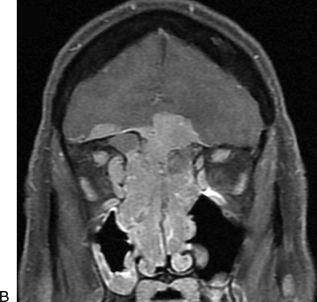
FIGURE 19.3 Typical aggressive SCC ex-inverting papilloma with extension into the lateral aspect of the frontal sinus (A) and an aggressive atypical meningioma with involvement of the roof of the orbit (B). Both required endoscopic-assisted resections.
Classic absolute indications to combined endoscopic and open cranial resection:
1.Involvement of the dura beyond the midorbital roof and intraorbital extension
2.Involvement of the anterior table or lateral recess of the frontal sinus
3.Significant involvement of the posterior table of the frontal sinus, where preservation of the sinus is not practical and cranialization should be performed
4.Tumor superior or lateral to the optic nerve canal
5.Tumor lateral to the carotid artery or involvement around bifurcations
6.Extension into facial or orbital soft tissues (usually transfacial approaches apply)
Relative indications:
1.Gross involvement of brain parenchyma
2.Lateral extension of tumor to the lateral wall of the maxillary sinus and infratemporal fossa
CONTRAINDICATIONS
Tumors that are situated entirely medial to the cavernous internal carotid artery (ICA) are most accessible using an endonasal approach and do not need an open approach. Where bacterial colonization is associated with the pathology, preoperative antibiotic therapy should be given. Severe local mucosal involvement from concomitant inflammatory conditions should warrant consideration of an alternate route.
PREOPERATIVE PLANNING
Radiologic Evaluation
Imaging should always be focused on what is trying to be achieved, namely tumor staging. Accurate information on local tissue involvement is critical for “T” staging. Most patients will undergo both computed tomography (CT) and magnetic resonance imaging (MRI) for several reasons. The T2 MRI will highlight edematous mucus and retained secretions compared to the tumor as defined on T1 post–contrast imaging (Fig. 19.4A). The involvement of the periorbita is determined by bone loss on CT and enhancement of adipose tissue on MRI. Thirdly, involvement of the dura (and brain parenchyma) is defined by bone loss on CT and dural enhancement on MRI (Fig. 19.4). Perineural involvement of cranial nerves is usually defined using fine-slice adipose tissue–saturated T1 post–contrast MRI. Finally, the relationship of the tumor to the intracranial course of the ICA and its branches is defined by either CT or MR angiography. Formal angiography of the ICA should be considered when there is tumor involvement or ectasia. The merits of preoperative balloon occlusion testing are very limited and should be applied when a sacrifice of the carotid artery and bypass is being considered and not just because of the risk of carotid bleeding. Where possible, include a scan series (CT or MRI) for future image-guided surgery (IGS) in the initial assessment.
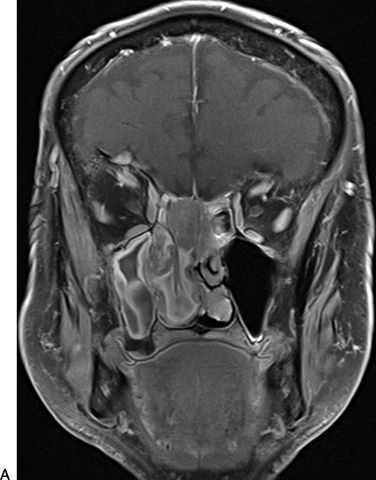
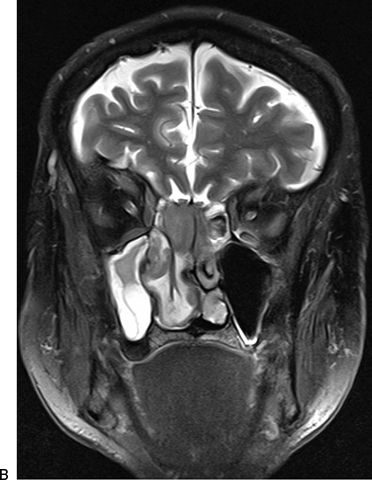
FIGURE 19.4 The T1 (A) and T2 post–contrast (B) MRI characteristics of an invasive right sphenoethmoid SCC. The differentiation of tumor, mucus, and mucosal edema can be seen.
Regional and distant metastases may be defined with a positron emission tomography/CT assessment. This technique is a combination of full-body CT and assessment of focal radioactive glucose uptake (18FDG) by cells. This is the most efficient form of staging and can provide standard uptake value information for subsequent follow-up. Imaging of the neck, chest, and abdomen as well as blood tests for calcium and alkaline phosphatase would also suffice. Specific investigations for bone, brain, or other metastasis are usually driven by clinical suspicion rather than being routine.
Histopathologic Diagnosis
Obtaining histopathologic confirmation of malignancy and its subtype is critical prior to therapy. This is usually done prior to treatment decision making, and the use of “frozen” or intraoperative specimens is ill advised and not recommended for a definitive diagnosis. This is important as some tumors such as lymphomas are radiosensitive and do not require surgery, whereas a diagnosis of melanoma would prompt an aggressive search for metastasis prior to local treatment.
The WHO classification is listed in Table 19.1 with the most common subtypes included. The epithelial versus nonepithelial distinction is easy and reflects the frequency of tumors. Epithelial tumors are the most common with squamous cell carcinoma (SCC), adenocarcinoma, and adenocystic carcinoma most commonly reported. The nonepithelial tumors are lymphoma (hematologic), olfactory neuroblastoma (neuroectodermal), chondrosarcoma (bone/cartilage), and mucosal melanoma (neuroectodermal).
Table 19.1 The WHO Classification System for Sinonasal Malignancies
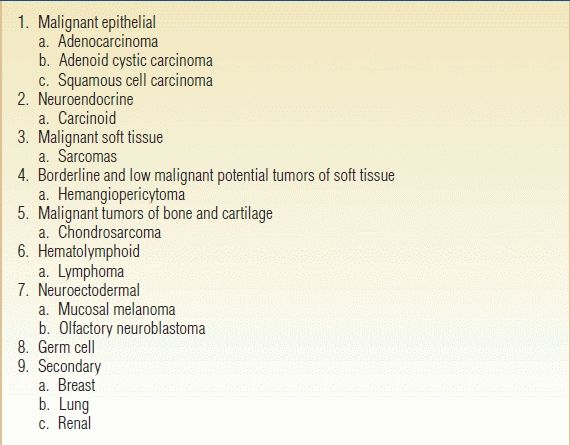
The Main Subtypes are Described Here with Common Pathologies.
Endoscopic biopsy can be performed in either a clinic or an operating room. The ability to manage a biopsy site that bleeds is critical. When lesions have already been imaged and the pathology is in the proximal nasal cavity anterior to the middle turbinate, we routinely biopsy these in the clinic as we have bipolar forceps and compression dressings available. This greatly assists in organizing further investigations and treatment decision making.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


