CHAPTER 181 Anatomy and Developmental Embryology of the Neck
Posterior Triangle of Neck
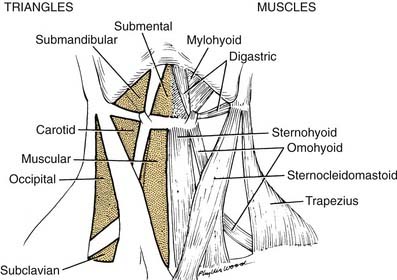
The posterior triangle is bordered by the sternocleidomastoid muscle, the anterior border of the trapezius muscle, and the middle third of the clavicle (Fig. 181-1). Specific layers of deep fascia form the floor (medial wall) and roof (lateral wall) of the triangular box. An understanding of the fascial relationships in the neck is important not only because of the boundary relationships but also because fasciae form planes that provide routes of surgical access or pathways for hemorrhage and infection. For this reason, a brief discussion of the fascial planes is necessary before proceeding with the anatomy of the posterior triangle.
Fascia of Neck
One of the earliest lessons in anatomy is that there are two types of fascia in the body: the superficial and the deep. In the region of the abdominal wall, superficial fascia consists of two layers—a fatty layer (Camper’s fascia) and a deeper, membranous layer (Scarpa’s fascia). The deep fascial layer of the abdominal wall is not subdivided but simply envelops the abdominal muscles. In the neck the superficial fascia is very thin and is not divided into layers, whereas the deep fascia is divided into three layers.1 The names of these layers vary with different authors, resulting in a somewhat chaotic terminology. Regardless of the terminology used, the divisions are arbitrary at best. A simple approach can provide a workable solution for either the anatomist or the surgeon.
Deep Fascia
The deep fascia is divided into three layers, demonstrated best when the neck is viewed in cross section (Fig. 181-2). These are the external, middle, and internal layers of the deep cervical fascia. The external layer of deep fascia underlies the platysma muscle and completely invests or encircles all of the superficial neck structures. For these reasons, the external layer is also known as the superficial layer, or investing layer, of deep fascia. In the region of the sternocleidomastoid and trapezius muscles, it splits and envelopes the individual muscles. A middle layer of the deep cervical fascia encloses the visceral structures of the neck (the trachea and esophagus). Hence the synonym for the middle layer is the visceral fascia.
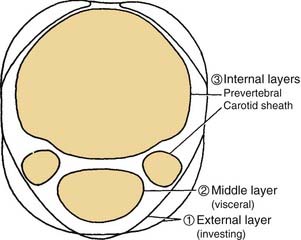
Figure 181-2. Divisions of the deep cervical fascia seen in transverse section at the level of cranial nerve VII.
The third, or internal, layer of the deep cervical fascia surrounds the deep muscles of the neck and cervical vertebrae (Fig. 181-3). This layer also is known by its descriptive term prevertebral fascia (although “paravertebral fascia” would have been more appropriate). The muscles enclosed by the prevertebral fascia include the deep muscles of the neck (the cervical part of the erector spinae); the levator scapulae; the scalenus anterior, middle, and posterior muscles; and the longus colli and longus capitis muscles, which lie on the anterior aspect of the cervical vertebrae. The last-named pair of muscles serve as flexors of the vertebrae; the longus capitis also assists in flexion of the skull. The scalenus group underlies the prevertebral fascia in the region of transverse processes of the cervical vertebrae. The anterior tubercles of the transverse processes provide origin for the scalenus anterior muscle, whereas the posterior tubercles provide the origin for the scalenus medius and posterior muscles. Continuing posteriorly, in order, are the levator scapulae and deep cervical muscles already noted.
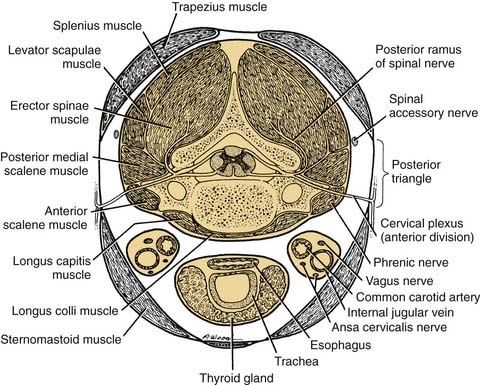
Figure 181-3. Structures contained by the deep cervical fascia seen in transverse section at the level of the cranial nerve.
The internal layer of deep fascia is described by some authors as enveloping the carotid and jugular vessels. Hence, the carotid sheaths are included as part of the definition of the internal layer of deep fascia. An effective means of visualizing the spatial relationships of these layers of fascia is to examine a cross section of the neck. This view not only is informative in defining the three layers of deep fascia but also serves to relate them to the posterior triangle of the neck (see Fig. 181-2). Placing a finger over the middle of the posterior triangle (i.e., between the trapezius and sternocleidomastoid muscles) will clarify that the roof (lateral wall) of the triangle is formed by the superficial layer of deep fascia. Palpation deeper into the triangle will bring the tip of the finger into contact with the prevertebral fascia that forms the floor of the posterior triangle and invests the prevertebral muscles. If the superficial layer of the deep fascia is incised, a finger inserted into the space, exploring anteriorly between the sternocleidomastoid and prevertebral muscles, will encounter the carotid sheath. This is a surgical approach to the retropharyngeal area or to the carotid vessels for vascular surgery.
Contents of Posterior Triangle
Cutaneous Branches of Cervical Plexus
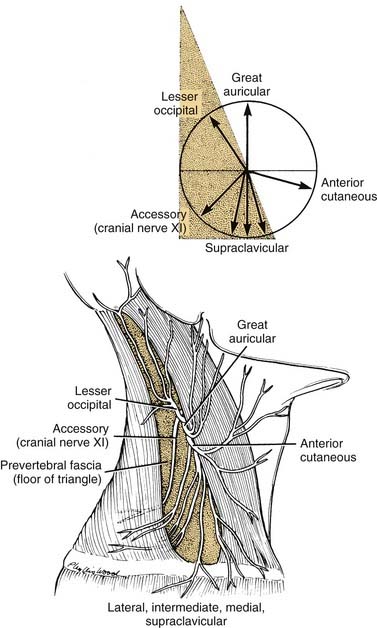
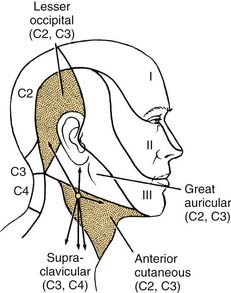
The sensory branches of the cervical plexus contained within the posterior triangle are four cutaneous nerves, which supply the skin of the head and neck from the area of the posterior scalp to the supraclavicular region. These cutaneous nerves are the (1) lesser occipital, (2) great auricular, (3) anterior, and (4) supraclavicular (Fig. 181-4). The first three of these nerves contain cervical segments C2 and C3 and the supraclavicular nerves C3 and C4. The topographic relations of these nerves and their distribution to the skin are illustrated in Figure 181-5. The important landmark for the cervical nerves is the accessory nerve at the point where it enters the posterior triangle from under cover of the sternocleidomastoid muscle. If this point is viewed as the center of a clock face, the cervical nerves mimic the hands pointing in different directions (see Fig. 181-4, inset). For instance, on the right side, the lesser occipital nerve is approximately at the 11 o’clock position, the great auricular is at the 12 o’clock position, and the anterior cutaneous nerve of the neck can be found at the 3 o’clock position. The supraclavicular nerves consist of three or four bundles of filaments scattered between the 5 and 7 o’clock positions on the clock’s face. Continuing this analogy, the accessory nerve can be seen to traverse the posterior triangle along the line of the 8 o’clock position until it enters the deep surface of the trapezius muscle. Viewed in this manner, the accessory nerve serves as a focus for organizing the pathways of the cutaneous nerves, as well as for emphasizing cranial nerve XI as a motor nerve in the posterior triangle.
Accessory Nerve
The accessory nerve is the only motor nerve in the posterior triangle as just defined. However, if the prevertebral fascia is incised, it is possible to encounter the motor nerves of the deep cervical muscles, the phrenic nerve, or the brachial plexus. With regard to its innervation of the sternocleidomastoid and trapezius muscles, cranial nerve XI is in fact a spinal nerve. Cell bodies of motor neurons innervating these muscles lie near the ventral horn in the upper cervical spinal cord, in the region of segments C2 through C4. The axonal fibers exit the anterior lateral portion of the cord as a series of fine filaments before becoming bundled as a nerve fiber within the subarachnoid space of the vertebral canal. The nerve ascends in the subarachnoid space, enters the posterior fossa through the foramen magnum, and joins with the cranial root of the accessory nerve before exiting the skull through the jugular foramen on the deep surface of the internal jugular vein. As the nerve descends the neck adjacent to the carotid sheath, motor or sensory filaments may join the nerve directly from segments C2 through C4.2 After crossing the deep surface of the sternocleidomastoid muscle, the nerve enters the posterior triangle, as already described.
Anterior Triangle of Neck
The anterior triangle of the neck is complementary to the posterior triangle and is bounded by the sternocleidomastoid muscle, the body of the mandible, and the midline of the neck. This space can be further subdivided into smaller triangular units, such as the submandibular triangle, and carotid and muscular triangles, which are included in this discussion (see Fig. 181-1).
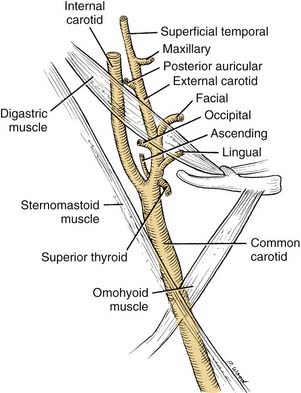
Carotid Triangle
The major focal point of the triangle is the bifurcation of the common carotid artery (Fig. 181-6). The internal carotid artery ascends the neck without branching. The external carotid artery provides several branches, many of which are important landmarks. The external carotid artery has anterior, posterior, and terminal branches.
Ansa Cervicalis
The ansa cervicalis is part of the cervical plexus. Its essential role is to supply the infrahyoid muscles: the sternohyoid, sternothyroid, and omohyoid muscles (Fig. 181-7). C1 fibers, which descend the neck, enter the hypoglossal nerve and travel as far as the occipital artery. At this point the hypoglossal nerve curves anteroinferiorly, but C1 fibers descend the neck to form the branch of cranial nerve XII, termed the superior root of the ansa. Fibers from C2 and C3 form an inferior root, which descends the carotid sheath on the surface of the internal jugular vein before turning anteroinferiorly to join the superior root. The ansa cervicalis is thus formed by the union of the two roots of the ansa. Three muscles are supplied directly by the ansa: the sternohyoid, sternothyroid, and omohyoid. At the origin of the superior root of the ansa, some C1 fibers do not follow the superior root but rather continue in the hypoglossal nerve transversely across the neck, before leaving cranial nerve XII to supply either the thyrohyoid muscle or the geniohyoid muscle (see Fig. 181-7
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


