 on Hippel–Lindau disease (VHL) is a genetic condition that involves the growth of angiomas in highly vascular areas of body, including the retina. Although the angioma from VHL can grow in the brain, spinal cord, adrenal glands, kidney, and pancreas, an angioma in the eye is the only VHL hemangioma that can be directly observed.
on Hippel–Lindau disease (VHL) is a genetic condition that involves the growth of angiomas in highly vascular areas of body, including the retina. Although the angioma from VHL can grow in the brain, spinal cord, adrenal glands, kidney, and pancreas, an angioma in the eye is the only VHL hemangioma that can be directly observed.
Pathophysiology and Clinical Presentation
Lesions in VHL can be single or multiple, with considerable variation in appearance and progression through the various stages. Five clinical stages can be identified, as discussed below.
Preclassical
In this stage, small capillary clusters can be seen in the retina. Lesions appear as simple red spots or microaneurysms.
Classical
The classical retinal hemangioma is a knot of vessels with a large artery as a feeder vessel leading to the hemangioma and a large vein as a draining vessel. In the early stages, the hemangioma appears as a nodule with normal-sized vessels. As the lesion grows, the feeder vessels can become two or three times the size of a normal retinal artery or vein. Eventually the lesion becomes elevated. Depending on the location of the lesion, these could be asymptomatic or symptomatic.
Exudative
Fluid leaks across the walls of the lesion result in retinal edema, retinal exudates, and leaked proteins and plasma from the blood. The accumulation of fluid causes retinal swelling and edema. The symptoms may include blurred vision, loss of visual acuity, or vision distortion.
Retinal Detachment
The retinal exudates and edema lift the retina from the choroid. This has a tendency to spread and may cause partial or complete loss of vision.
End Stage
In this stage, the retinal detachment progresses. Glial or scar tissue is likely to form, which may lead to painful glaucoma, and vision maybe permanently lost.
CASE STUDY
We have treated three patients who had stage four VHL with extensive exudates and retinal detachment. One case example is discussed below.
Case
A 48-year-old man presented with no light perception in left eye for 2 years. He gave a history of gradual, painless loss of vision in the left eye for 2 months. On examination, the intra-ocular pressure was low. Examination of the anterior segment showed early cataract changes. Fundus examination of the right eye showed a complicated and old retinal detachment. Fundus examination of the left eye showed a slight media haze with retinal exudation and detachment. At the 5 o’clock position on the periphery lay a circumscribed exophytic retinal capillary hemangioma approximately 2 disc diameter with a prominent dilated and tortuous feeding artery and draining vein (Fig. 38.1–38.4).
All treatment options were discussed in great detail with the patient, including the risks involved and the possibility of uncontrollable bleeding. The Fugo blade was our instrument of choice for dealing with this tumor.
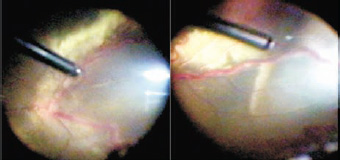
Figure 38.1. Dilated vessels with retinal detachment and exudation.

Figure 38.2. Dilated and tortous feeding and draining vessels.

Figure 38.3. Extensive subretinal exudation.
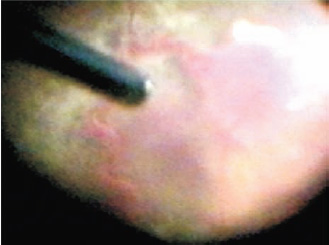
Figure 38.4. The vascular tumor with feeding and draining vessels.
Surgical Technique
- Perform a complete pars plana vitrectomy and remove the membranes from the retinal surface with end-gripping forceps.
- Ablate the tumor with the activated Fugo tip until no sign of it is left (Fig. 38.5 and 38.6). No bleeding from the tumor should occur. The engorged vessels retract and slowly thin.
- Flatten the retina using perfluorocarbon liquid and then use a laser after releasing the retinal traction from the periphery of the vascular tumor (Fig. 38.7).
- After settling the retina, inject silicone oil to tamponade the retina.
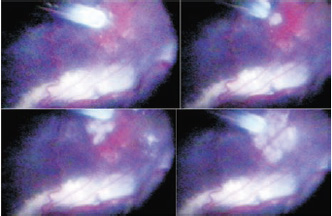
Figure 38.5. Direct ablation of the vascular tumor with the Fugo blade. No bleeding is present.
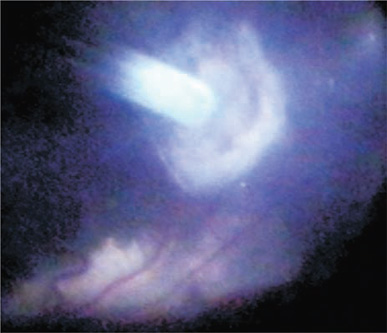
Figure 38.6. Nearly completed tumor ablation.

Figure 38.7. Subretinal fluid drainage and endo-laser were applied around the vascular tumor. The large vessels connected to the tumor have shrunk.
Postoperative Management
Postoperatively, our patient was followed for 4 months before the silicone oil was removed. The patient recovered with 6/24 vision.
Because there was no tumor left, blood vessels supplying the area lost their tortuosity and diminished in size. All that remained of the tumor was a dense white scar in the periphery.
Summary
This surgery is generally not attempted for fear of bleeding from the engorged vessels of Von Hippel–Lindau disease and the tumor, but the Fugo blade made this procedure simple and safe.
Suggested Reading
Singh IR. Managing proliferative vitreo-retinopathy with the Fugo blade—a case report. Trop Ophthalmol. 2001;1:24–25.
Singh IR. Vitreo-retinal surgery with plasma blade: a case report. Trop Ophthalmol. 2001;1:13–16.
Singh IR, Singh D, Singh RK, et al. The plasma blade in vitreoretinal surgery. Ann Ophthalmol. 2001;33:280–289.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


