22
Vocal Fold Polyps and Cysts
Vocal fold polyps and cysts are considered vocal masses because they add weight and may displace the existing microanatomy. As such, these masses have a direct effect on the vibrating margin, so video or digital stroboscopy is especially helpful in characterizing these lesions. Although the terms polyp and cyst imply different types of lesions, there is actually a continuum of vocal fold masses with overlap in features between these lesions in some cases.1 Both types of lesions may be associated with intracordal scarring (within the lamina propria), sulcus deformities (epithelial indentations or defects bridging superficial to the deeper layers of the vocal fold microanatomy), as well as reactive callus or hyperkeratosis on the contralateral vocal fold. In this latter situation, bilateral lesions may initially appear as “nodules” if one were not to have the benefit of stroboscopy. Therefore, an understanding of the pathogenesis of these lesions and an understanding of typical findings on stroboscopy will improve accuracy of diagnosis, surgical planning, and ultimately prognosis to treatment.
 Pathogenesis of Polyps and Cysts
Pathogenesis of Polyps and Cysts
Both polyps and cysts are believed to have similar initiating factors involving mucosal injury due to a multiple of factors, although they are believed to have different final steps in their pathogenesis. Vocal overuse and misuse are central to the development of vocal fold masses. This initial trauma is exacerbated by baseline inflammation often caused by laryngopharyngeal reflux. Another source of baseline inflammation may be sinonasal or pulmonary diseases. The resulting mucosal injury leads to increased shearing forces at the midportion of the membranous vocal fold, which is the most common site of vocal fold polyps and cysts.2 In many cases, the presence of the mass causes impaired glottic closure during phonation resulting in excess air egress, so there is a tendency for the patient to compensate for resulting voice limitations with hyperfunctional voice behavior.3 This maladaptation further increases shear and prevents the natural healing process.
In the case of vocal fold polyps, it is believed that capillary hemorrhage in the superficial lamina propria leads to extravasation of blood, resultant local edema, and ultimate organization with hyalinized stroma.4 Pathologically, polyps are acellular, with thickened epithelium over superficial lamina propria, and increased vascularity in an abundant delicate fibrin stromal matrix. They have more vasculature and less organized collagen than do nodules, but the distinction may be difficult for the pathologist.4 Immunohistochemistry studies reveal clustered fibronectin and disruption of laminar pattern suggesting diffuse injury in the region of the polyp.5
The resulting mass may be broad-based (sessile) or pedunculated (fusiform) and hemorrhagic versus nonhemorrhagic (Fig. 22.1). Hemorrhagic polyps may also have an associated blood vessel or varix. Though the gross appearance may vary, the lesion is generally considered to be an out-pouching of inflamed and organized Reinke’s space. Therefore, a superficial nonhemorrhagic, broad-based polyp may be interpreted as a pseudocyst, as a true cyst has an intact epithelial lining.
Vocal fold cysts are subepidermal epitheliallined sacs located within the lamina propria and may be mucus retention or epidermoid in origin (Fig. 22.2). Mucusretention cysts form when a mucous gland duct becomes obstructed (usually during an upper respiratory infection or with overuse), retaining glandular secretions. Epidermoid cysts develop either from congenital cell rests in the subepithelium (from the 4th and 6th branchial arches) or from healing injured mucosa burying epithelium. A ruptured cyst may result in scarring within the lamina propria or in a sulcus. Varices are also often associated with vocal cysts.
 Indications and Usefulness of Stroboscopy
Indications and Usefulness of Stroboscopy
As one may infer from the discussion above, a two-dimensional picture of the vocal folds is not sufficient to characterize features that may be used to distinguish polyps from cysts. Transoral mirror evaluation and traditional indirect laryngoscopy may recognize a vocal fold mass, but the displacement of normal architecture in the vocal fold microanatomy lends itself to characteristic stroboscopic findings in the two lesions.6 Therefore, in addition to the use of traditional indirect laryngoscopy to visualize the larynx, stroboscopy is uniquely useful and indicated to characterize a lesion and its relationship to the layered microanatomy of the vocal fold and to help determine the etiology of dysphonia in patients when a lesion, or cause, is not apparent.
As these masses have distinct histology, the prognosis is different, and the best treatment is also different. Treatment modalities may include behavioral, medical, surgical, or office-based procedures. For example, a hemorrhagic vocal polyp with associated varix may be amenable to an office-based angiolytic laser treatment, sparing an epithelial dissection and potentially facilitating recovery of the voice.7 A vocal polyp may be amenable to resolution with strict voice rest and behavior modification in selected individuals.8 Conversely, a true cyst will not resolve with conservative management. The phonosurgical approach for cyst removal requires more extensive dissection than does that with a polyp, as the cyst is in the submucosal plane. The cyst may also be associated with intracordal scarring, requiring a more elaborate dissection. Consequently, recovery of the mucosal wave is prolonged and may never return to being completely normal. Furthermore, leaving behind a minute fragment of epithelium in the cyst sac may result in recurrence of the cyst.9 In a large series of patients, Sataloff et al. recognized the usefulness of videostroboscopy to help distinguish between polyps and cysts and thus improve surgical planning and preoperative patient counseling.10
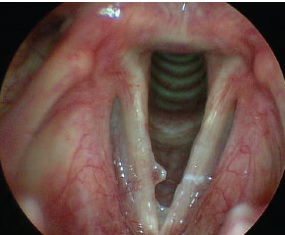
Fig. 22.1 A broad-based sessile polyp with subtle hemorrhagic component on the right vocal fold. Note that signs of posterior inflammation and thick dry mucus from laryngopharyngeal reflux pay tribute to multifactorial contributions to the pathogenesis of the polyp.
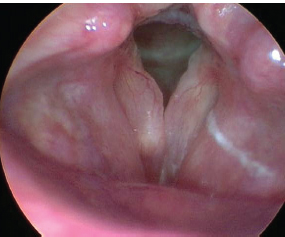
Fig. 22.2 A right vocal fold mucus inclusion cyst. Note that these vocal folds are markedly edematous consistent with polypoid corditis (Reinke’s edema), which often occurs as a result of chronic irritation/inflammation.
 Interpretation: Impact of Polyps and Cysts on Vibratory Parameters
Interpretation: Impact of Polyps and Cysts on Vibratory Parameters
As discussed elsewhere in this text, stroboscopy features may help distinguish polyps from cysts. These features include glottic configuration, amplitude of vibration, mucosal wave phase (closed, open, irregular, hourglass, anterior/posterior chink), mucosal wave symmetry/asymmetry, and periodicity (regular, irregular). Common to both lesions is the impact of the mass on the linearity of the vocal fold, which often results in premature contact at the site of the lesion and subsequently an hourglass or irregular glottic configuration on phonation.
Vocal folds with small polyps generally have intact mucosal waves but phase asymmetry due to the impaired phase closure and the mass effect of the polyp (Video Clips 23 and 46). Vocal folds with larger polyps may have increased mucosal wave amplitude due to a shearing effect tethering a pedunculated polyp to the normal adjacent mucosa or decreased amplitude due to overwhelming mass effect. As polyps are asymmetric masses of the vocal folds, they are more prone to result in chaotic vibrations and aperiodic mucosal waves.11 Examples of vocal polyps and their impact on vibratory patterns seen on stroboscopy are shown and discussed in Figs. 22.3 to 22.6.
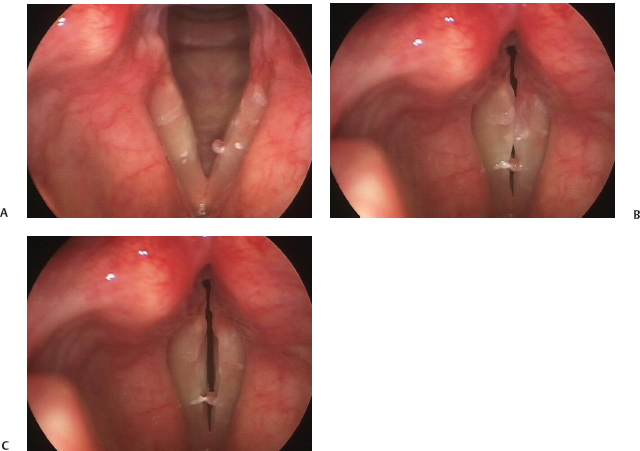
Fig. 22.3 (A) Small pedunculated hemorrhagic polyp involving the medial margin of the left vocal fold, seen on abduction and associated with left sulcus vergeture and tight contact irritation. (B) Small pedunculated hemorrhagic polyp involving the medial margin of the left vocal fold seen during phonation showing the mass effect limiting phase closure. (C) Small pedunculated hemorrhagic polyp involving the medial margin of the left vocal fold seen during latephase closure on stroboscopy demonstrating intact left vocal fold mucosal wave. Note the area of contact irritation on the right vocal fold now shows a small area of hyperkeratosis at the inferior margin of the vocal fold striking zone that is apparent only on stroboscopy because the mucosal wave allows visualization of the inferior margin.
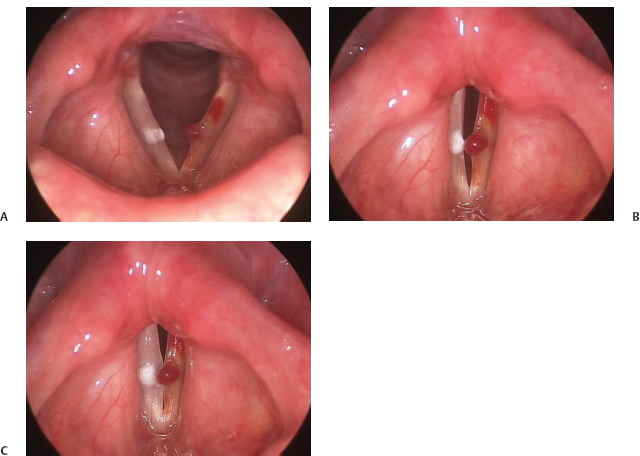
Fig. 22.4 (A) Left vocal fold hemorrhagic polyp associated with varices and active vocal fold hemorrhage, seen on abduction. (B) Early contact of the polyp with the contralateral vocal fold seen on stroboscopy. (C) Late-phase closure of the vocal folds in the case of left vocal fold hemorrhagic polyp. Note that the presence of an intact mucosal wave bilaterally permits the rotation of the polyp superiorly to allow for improved (yet compromised) phase closure on phonation.
The history of a patient with a vocal cyst is similar to those of patients with nodules and polyps, but often with less vocal limitation than expected from its size. The voice may sound diplophonic (particularly with epidermoid cysts), where there is great pitch instability and there is splitting of the fundamental frequency overtones.
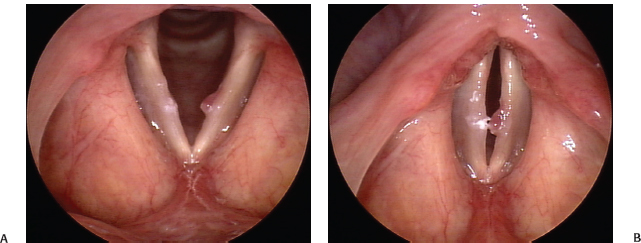
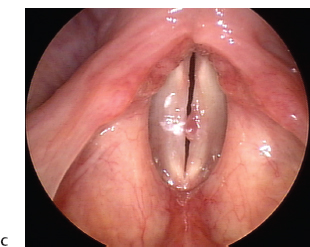
Fig. 22.5 (A) Left vocal fold oblong sessile polyp, seen on abduction, with a contralateral (right) reactive callus. (B) Early phase closure on phonation demonstrating the typical but irregular hourglass closure in a case of left vocal fold oblong sessile polyp. (C) Later phase closure seen on stroboscopywith compression of the polyp by the vocal folds. Note that there is poor excursion of the mucosal wave (with decreased amplitude) on both vocal folds associated with chronic inflammation and possible intracordal scarring.
Though it is often possible to distinguish some cysts solely by still-light endoscopy, visualizations of the outline of the cyst, associated capillary patterns, and characteristic changes in the edge or free margin are not always present. On stroboscopy, the vocal folds appear asymmetric with occasional evidence of the subepithelial mass. The free edges of the vocal folds are generally smooth.12
Due to displacement of the lamina propria and the fibrosis that frequently occurs around vocal fold cysts, there is a significant decreased or absent mucosal wave on the side of the cyst (Video Clip 26). Whereas vocal fold polyps have intact mucosal waves in 80% of all cases, Shohet et al. demonstrated the mucosal wave to be diminished or absent in 100% of vocal fold cysts.13 This can be explained by changes in the elastic coefficient of the lamina propria surrounding the cyst.14 If light reflection indicates an intact mucosal wave, the vocal fold with a cyst will not reflect light. In contrast with a polyp, a cyst would have a dynamic segment of mucosa adjacent to the cyst, lacking reflected light, with an intact mucosal wave over the contralateral cord-corresponding segment.13 The amplitude and vibration of the wave are also diminished and absent.9 Examples of vocal cysts and their impact on vibratory patterns seen on stroboscopy are shown and discussed in Figs. 22.7 to 22.10.
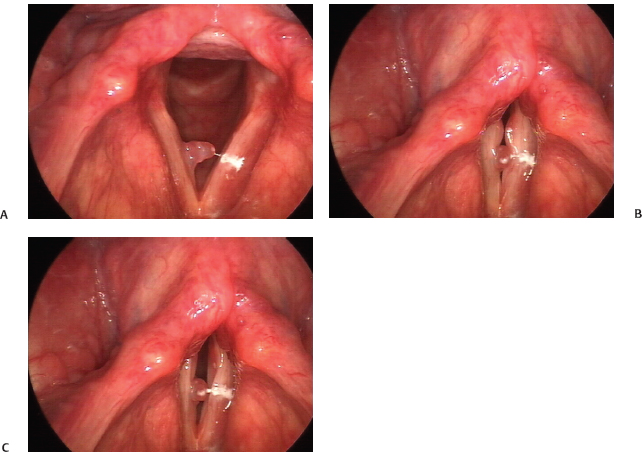
Fig. 22.6 (A) Right lobulated polyp with broad-based edema at the vocal fold margin, seen on abduction. (B) Initial phase of closure with deformity of the vibratory margin at the site of the lobulated polyp, resulting in the appearance of good phase closure. (C) However, the trailing edge of the intact mucosal wave (particularly on the left vocal fold) reveals the impaired closure and reduced right mucosal wave secondary to the mass effect of the polyp.
 Pearls and Pitfalls in the Diagnosis of Polyps and Cysts on Stroboscopy
Pearls and Pitfalls in the Diagnosis of Polyps and Cysts on Stroboscopy
The general pearls that may be assumed from the above discussion follow:
- Polyps are out-pouchings of Reinke’s space, may be pedunculated (fusiform) or broad-based (sessile), and may or may not show signs of hemorrhage.
- Cysts are epithelial-lined sacs within Reinke’s space and may be mucus or epidermoid related.
- Polyps and cysts result in an hourglass or irregular vocal fold glottic configuration on phonation.
- The amplitude of the mucosal wave is generally decreased with vocal cysts, whereas it is generally normal or increased with vocal fold polyps.
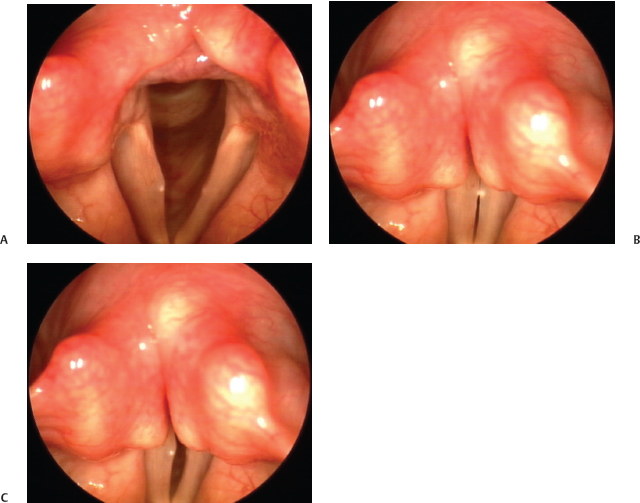
Fig. 22.7 (A) Right vocal fold cyst, seen on abduction. Although there is not a discrete submucosal mass seen, the appearance of a focal submucosal fullness is a clue to the underlying cyst. (B) Initial contact of the vibratory margin on stroboscopy reveals irregular closure and premature contact at the apex of the cyst. (C) Later phase closure reveals an intact mucosal wave on the left vocal fold with significantly reduced mucosal wave on the right.
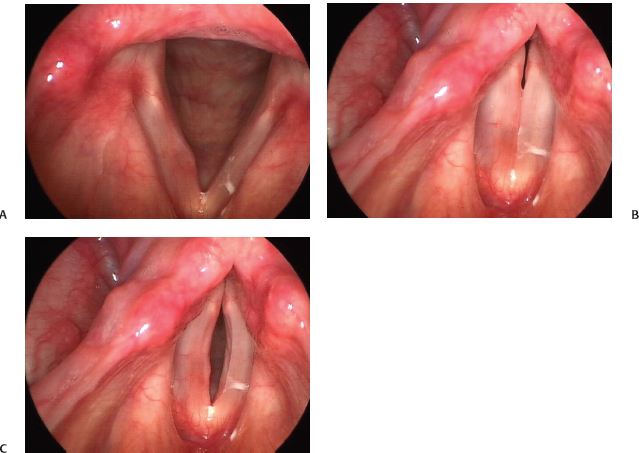
Fig. 22.8 (A) Subtle right vocal fold cyst, seen on abduction with associated hyperemia. (B) There is the initial appearance of linear vocal fold closure with only a minor posterior chink with subtle right vocal fold cyst. (C) Later phase vocal fold vibration seen on stroboscopy reveals decreased to absent right mucosal wave, intact left mucosal wave, and more obvious right submucosal contour consistent with the cyst. This is a particularly good example of how a subtle lesion may be missed on still-light two-dimensional endoscopy in the absence of stroboscopy.
- The amplitude of vibration will likely be decreased secondary to the mass of the lesion combined with an incomplete glottic closure.
- Vocal fold vibration will likely be asymmetric and possibly aperiodic.
Despite these pearls, there are pitfalls in the use of stroboscopy to distinguish vocal fold polyps from cysts or other lesions. The presence of a polyp or cyst may cause a reactive lesion, or “callus,” on the contralateral vocal fold secondary to contact irritation. A unilateral lesion with reactive callus formation may look like bilateral lesions, in other words nodules, which may confound the diagnosis, prognosis, and ultimate management. Also, though the glottic closure of the vocal folds with cysts may often be complete (for example), it depends on the cyst size and whether there is development of the callus on the contralateral vocal fold (Video Clip 26).
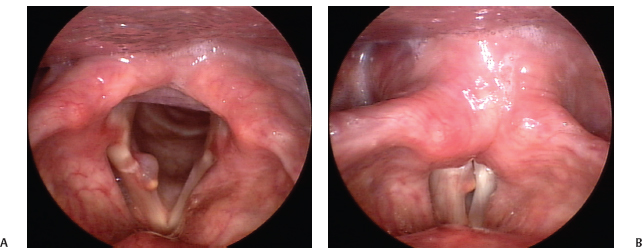
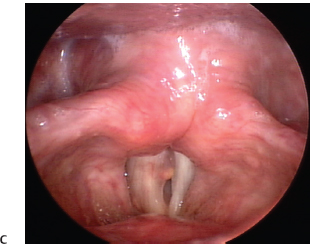
Fig. 22.9 (A) Large right posterior vocal fold mucus inclusion cyst with hemosiderin deposition superficially (seen as yellow spot) suggestive of prior hemorrhage, seen on abduction. (B) Early glottal closure is noted to be poor due to the mass effect of the cysts. (C) Intact left vocal fold mucosal wave with absent mucosal wave on the right, despite the posterior location of the cyst.
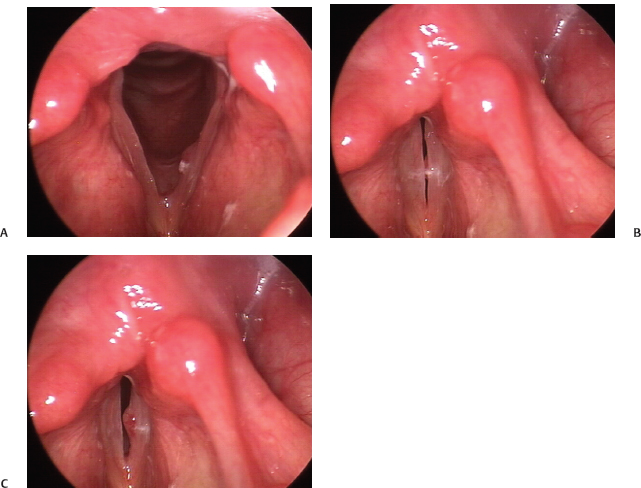
Fig. 22.10 (A) Left submucosal cyst with hemorrhage in a patient with severe chronic laryngitis (manifested by edematous and erythematous vocal folds, stagnant secretions, and interarytenoid inflammation), seen on abduction. (B) Early phase closure demonstrates only a small margin of the cyst caught tangentially on a vertical plane. (C) Intact (but decreased) left mucosal wave reveals eversion of the cyst on late phase closure during phonation, seen on stroboscopy. This example clearly demonstrates that the hemorrhagic component is within the superficial mucosa overlying the cyst and not within the cyst itself.
Rosen et al. evaluated a series of 85 patients with bilateral vocal fold lesions and found 21 to have nodules and 64 to have a unilateral vocal fold lesion with a contralateral reactive lesion (UVFL/RL).15 When comparing patients with nodules and those with UVFL/RL, they found statistically significant differences in (1) symmetry of vocal fold vibration, (2) amplitude perturbations, (3) estimated subglottic pressure, and (4) voice handicap index, suggesting that these parameters be used as tools to differentiate nodules from UVFL/RL.
Repeated inflammation, vocal trauma, vocal hemorrhage, and the presence of an intracordal cyst predispose to scarring in Reinke’s space. Intracordal scarring is often found in association with a cyst, particularly if it is epidermoid in origin and has ruptured. Intracordal scarring is suspected on stroboscopy when there is markedly reduced or absent mucosal wave (usually asymmetric) that often affects phase closure (Video Clip 33). It is crucial to differentiate between an uncomplicated subepithelial cyst and an intracordal scar, as the latter is a more complex problem with worse prognosis for voice rehabilitation. With these factors in mind, the typical “pearls” used to distinguish polyps from cysts on stroboscopy have understandable limitations. Nevertheless, the utility of stroboscopy in appropriate diagnosis, patient counseling, and treatment intervention is vital to obtaining the best outcome.
References
1. Altman KW. Vocal fold masses. Otolaryngol Clin North Am 2007;40:1091–1108, viii
2. Jiang JJ, Diaz CE, Hanson DG. Finite element modeling of vocal fold vibration in normal phonation and hyperfunctional dysphonia: implications for the pathogenesis of vocal nodules. Ann Otol Rhinol Laryngol 1998;107:603–610
3. Altman KW, Atkinson C, Lazarus C. Current and emerging concepts in muscle tension dysphonia: a 30-month review. J Voice 2005;19:261–267
4. Kotby MN, Nassar AM, Seif EI, Helal EH, Saleh MM. Ultrastructural features of vocal fold nodules and polyps. Acta Otolaryngol 1988;105:477–482
5. Courey MS, Shohet JA, Scott MA, Ossoff RH. Immunohistochemical characterization of benign laryngeal lesions. Ann Otol Rhinol Laryngol 1996; 105:525–531
6. Hirano M. Surgical Anatomy and Physiology of the Vocal Folds. Chicago, IL: Mosby-Year Book; 1993: 125–158
7. Ivey CM, Woo P, Altman KW, Shapshay SM. Office pulsed dye laser treatment for benign laryngeal vascular polyps: a preliminary study. Ann Otol Rhinol Laryngol 2008;117:353–358
8. Srirompotong S, Saeseow P, Vatanasapt P. Small vocal cord polyps: completely resolved with conservative treatment. Southeast Asian J Trop Med Public Health 2004;35:169–171
9. Johns MM. Update on the etiology, diagnosis, and treatment of vocal fold nodules, polyps, and cysts. Curr Opin Otolaryngol Head Neck Surg 2003;11:456–461
10. Sataloff RT, Spiegel JR, Hawkshaw MJ. Strobovideolaryngoscopy: results and clinical value. Ann Otol Rhinol Laryngol 1991;100(9 Pt 1):725–727
11. Zhang Y, Jiang JJ. Chaotic vibrations of a vocal fold model with a unilateral polyp. J Acoust Soc Am 2004; 115:1266–1269
12. Bouchayer M, Cornut G, Witzig E, Loire R, Roch JB, Bastian RW. Epidermoid cysts, sulci, and mucosal bridges of the true vocal cord: a report of 157 cases. Laryngoscope 1985;95(9 Pt 1):1087–1094
13. Shohet JA, Courey MS, Scott MA, Ossoff RH. Value of videostroboscopic parameters in differentiating true vocal fold cysts from polyps. Laryngoscope 1996; 106(1 Pt 1):19–26
14. Loire R, Bouchayer M, Cornut G, Bastian RW. Pathology of benign vocal fold lesions. Ear Nose Throat J 1988;67:357–358, 360–362
15. Rosen CA, Lombard LE, Murry T. Acoustic, aerodynamic, and videostroboscopic features of bilateral vocal fold lesions. Ann Otol Rhinol Laryngol 2000;109:823–828
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


