10
Introduction to Videostroboscopy
Just like the beating of hummingbird wings, human vocal folds vibrate at a rate that is faster than can be perceived by the human eye. The evaluation of vocal fold anatomy, mucosal color, and gross movement can be performed while illuminating the vocal folds with a constant light source. But the evaluation of vocal fold vibration requires special imaging technology to “slow down” vibration for assessment. At this time, the most widely used technique for assessing the vibratory characteristics of the vocal folds is videostroboscopy, which has become an accepted and essential component of the comprehensive evaluation of voice disorders (Video Clip 1).
Oertel created the first stroboscope in 1895, but videostroboscopy did not become widely clinically available until the later part of the 20th century.1 Chapter 1 in this text, on the history of laryngeal imaging, describes the development of laryngeal imaging techniques since Oertel’s initial breakthrough. Much has been learned about vocal fold vibration as a result of the clinical use of videostroboscopy during the past several decades, and that knowledge can be applied to the evaluation of patients with voice disorders. Our ability to observe vocal fold vibration using videostroboscopy has also instigated further study of vocal fold histology and of how vocal fold structure affects vibratory physiology. The knowledge gained from those studies forms the basis for the contemporary clinical evaluation of patients with voice disorders.
 Indications
Indications
Videostroboscopy is indicated when a detailed visual analysis of vocal fold vibration is desired. It is usually performed in addition to an indirect or flexible examination of the larynx. Though videostroboscopy may be performed as part of a complete evaluation of a patient in whom the diagnosis is obvious, videostroboscopy is particularly indicated in any patient who complains of hoarseness but has an otherwise normal indirect or flexible laryngoscopic examination. If these examinations have ruled out an obvious abnormality of the anatomy, such as a mass or a lesion of the vocal fold, and have ruled out an obvious movement disorder, such as vocal fold paralysis, then a further evaluation of the vocal fold vibratory characteristics is warranted. In addition to providing information regarding vocal fold vibration, the image obtained with videostroboscopy is magnified, allowing a more detailed assessment of the vocal fold anatomy than is possible with indirect or flexible laryngoscopy. Video cameras can record a digital high-definition format with phenomenal image quality.2 A detailed review of the recording, after the examination is completed, with slow motion or frame-by-frame analysis, allows for a comprehensive evaluation of the examination findings. As a result, videostroboscopy can often elucidate a vocal fold abnormality that was missed on indirect or flexible laryngoscopic examinations. Therefore, any patient with voice problems in whom the diagnosis is unclear is a candidate for videostroboscopy.
In addition to being an aid in the diagnosis of voice disorders, videostroboscopy is indicated to document vocal fold function prior to any treatment and to evaluate the outcomes of various interventions. The European Laryngological Society’s Committee on Phoniatrics has proposed a basic protocol for the assessment of every patient with voice pathology that includes videostroboscopy. The European Laryngological Society cites videostroboscopy as being integral to the protocol because they believe that “Videostroboscopy is the main clinical tool for the etiological diagnosis of voice disorders.” But the impetus behind the idea of using a protocol for the evaluation of every patient is that when the evaluation techniques are standardized across clinicians, the results of treatment can be compared between institutions.3 Because videostroboscopy provides the benefit of documenting the examination findings, subsequent examinations can be compared, so that the results of treatment can be studied. Indeed, videostroboscopy has been used successfully to document the results of certain surgical interventions by demonstrating an improvement in the vocal fold vibratory characteristics after the treatment.4,5 In addition, the results of videostroboscopy may be used during surgical planning. For example, videostroboscopy allows a detailed assessment of the degree of glottic closure, thus contributing to the planning of surgery in cases of vocal fold paralysis, along with an assessment of surgical results after treatment. Ford et al. took this concept one step further by using videostroboscopy during medialization procedures to determine when medialization was adequate as indicated by a return of the mucosal wave (indicating normal vibration) on the contralateral vocal fold.6
Videostroboscopy can be played back after completion of the examination so that patients can also view the examination during their evaluation, and the beneficial impact of patient education, with respect to the ultimate outcomes of treatment, should not be underestimated. Examination documentation and patient education have both become important indications for videostroboscopy.
 Examination
Examination
Videostroboscopy is performed with a rigid endoscope with a 70-degree or 90-degree angle of view. It is passed through the mouth, into the back of the pharynx, to visualize the larynx. A stethoscope on the patient’s neck measures the frequency of vocal fold vibration and sets the frequency of strobe flashing to a frequency slightly off and several multiples slower than vocal fold vibration allowing images from sequential parts of the vibratory cycle to be recorded and viewed as a “virtual” slow-motion movie of vocal fold vibration. Recording rates are typically 30 frames per second. In addition to the “asynchronized” mode of stroboscopy described above, the strobe can be set to a “synchronized” mode wherein the strobe will flash at a frequency identical to the frequency of phonation. The “synchronized” mode records images from the same point in the vibratory cycle, and the resulting recording shows a “still” image of the larynx captured from the same point in the vibratory cycle (Video Clip 2). Chapter 11 describes the technical details of videostroboscopy and includes information about the equipment required to perform it.
Videostroboscopy allows evaluation of the following vibratory parameters:
 Symmetry of vibration refers to the movement of the right and left vocal folds relative to each other. The right and left folds normally vibrate as mirror images of one another. They begin to move laterally at the same time and at the same speed. They are displaced laterally to the same extent and reach maximal lateral displacement at the same time. They then begin to close together at the same time and at the same speed (Video Clip 3). Differences in the mechanical properties of the two vocal folds, however, will result in asymmetric movements. Symmetry of vibration is influenced by differences in the position, shape, mass, stiffness, elasticity, and tension of the vocal fold tissues.
Symmetry of vibration refers to the movement of the right and left vocal folds relative to each other. The right and left folds normally vibrate as mirror images of one another. They begin to move laterally at the same time and at the same speed. They are displaced laterally to the same extent and reach maximal lateral displacement at the same time. They then begin to close together at the same time and at the same speed (Video Clip 3). Differences in the mechanical properties of the two vocal folds, however, will result in asymmetric movements. Symmetry of vibration is influenced by differences in the position, shape, mass, stiffness, elasticity, and tension of the vocal fold tissues.
 Periodicity of vibration refers to the relative length of the glottal cycle, and this should be stable from cycle to cycle. Use of the synchronized strobe setting can confirm that vibration is periodic (Video Clip 2). If the length of the vibratory cycle is stable from cycle to cycle, then a static image will persist with the strobe set to the synchronized mode. If changes in the length of the vibratory cycle are present, there will appear to be movement of the vibratory edge in the synchronized mode. Periodicity depends on the mechanical properties of the vocal folds and the expiratory force applied to them.
Periodicity of vibration refers to the relative length of the glottal cycle, and this should be stable from cycle to cycle. Use of the synchronized strobe setting can confirm that vibration is periodic (Video Clip 2). If the length of the vibratory cycle is stable from cycle to cycle, then a static image will persist with the strobe set to the synchronized mode. If changes in the length of the vibratory cycle are present, there will appear to be movement of the vibratory edge in the synchronized mode. Periodicity depends on the mechanical properties of the vocal folds and the expiratory force applied to them.
 Phase closure refers to the percentage of time that the vocal fold edges are open and/or closed during a single cycle of vibration. The phase characteristics are normally influenced by the mode of phonation (falsetto, modal phonation, glottal fry) and the pitch and loudness of phonation (Video Clip 4) (Fig. 10.1).
Phase closure refers to the percentage of time that the vocal fold edges are open and/or closed during a single cycle of vibration. The phase characteristics are normally influenced by the mode of phonation (falsetto, modal phonation, glottal fry) and the pitch and loudness of phonation (Video Clip 4) (Fig. 10.1).
 Amplitude of vibration refers to the amount of lateral movement of the vocal folds during vibration. Amplitude of vibration normally increases with increases in subglottic pressure, such as occurs during loud phonation. Amplitude of vibration also increases as the pitch or frequency of phonation decreases (Video Clips 5 and 6).
Amplitude of vibration refers to the amount of lateral movement of the vocal folds during vibration. Amplitude of vibration normally increases with increases in subglottic pressure, such as occurs during loud phonation. Amplitude of vibration also increases as the pitch or frequency of phonation decreases (Video Clips 5 and 6).
 Glottic configuration refers to the shape or contour of the glottic opening, if there is one, at the point of maximal closure during the vibratory cycle. Other terms for this charac teristic include the “contour of the glottal margin” and the “vocal fold closure pattern.” Chapters 14 and 17 cover the normal glottic configuration range and the differential diagnosis of abnormal glottic configurations, respectively.
Glottic configuration refers to the shape or contour of the glottic opening, if there is one, at the point of maximal closure during the vibratory cycle. Other terms for this charac teristic include the “contour of the glottal margin” and the “vocal fold closure pattern.” Chapters 14 and 17 cover the normal glottic configuration range and the differential diagnosis of abnormal glottic configurations, respectively.
 Mucosal wave refers to the movement of the superficial tissues over the vocal fold as the air moves through the glottis. The mucosal wave can be seen as a traveling wave in the superficial tissues over the top of the vocal fold surface from medial to lateral. Slow-motion or frame-by-frame analysis of the videostroboscopic recording is usually required for an adequate evaluation of the mucosal wave. The mucosal wave is interrupted with abnormalities of the vocal fold mucosal cover such as scarring, lesions, inflammation,and edema (Video Clip 7).
Mucosal wave refers to the movement of the superficial tissues over the vocal fold as the air moves through the glottis. The mucosal wave can be seen as a traveling wave in the superficial tissues over the top of the vocal fold surface from medial to lateral. Slow-motion or frame-by-frame analysis of the videostroboscopic recording is usually required for an adequate evaluation of the mucosal wave. The mucosal wave is interrupted with abnormalities of the vocal fold mucosal cover such as scarring, lesions, inflammation,and edema (Video Clip 7).
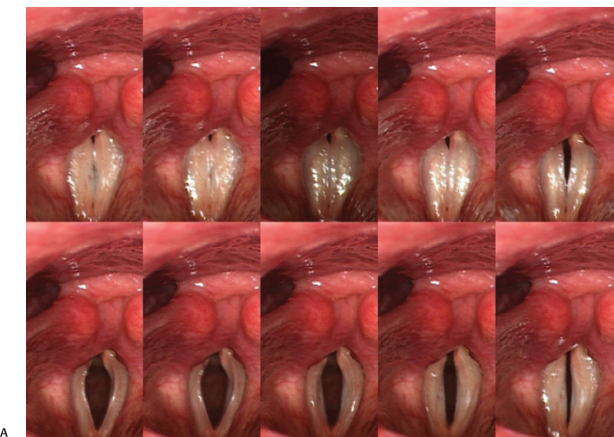
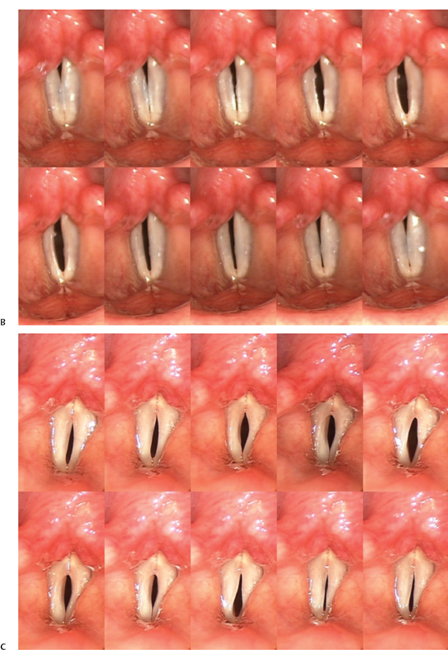
Fig. 10.1 (A) Montage function to evaluate phase characteristics. A normal open phase is 50%. (B) Montage of a single cycle of vibration reveals a subtle predominance of the open phase. (C) A persistent glottic opening throughout the vibratory cycle is consistent with more significant presbyphonia.
A detailed description of these vibratory parameters, including the range of normal findings, the impact of changes in loudness and pitch, and the expected findings in pathologic conditions of the larynx, is provided in later chapters of this book.
 Value of Videostroboscopy
Value of Videostroboscopy
The benefits of videostroboscopy in the evaluation of patients with voice symptoms have been well documented. Casiano et al. found that in patients with voice complaints and no abnormality identified on indirect laryngoscopy (previously diagnosed with a “functional voice disorder”), videostroboscopy resulted in a change of diagnosis in 44%. Furthermore, 20% of those patients diagnosed as having benign vocal fold lesions on indirect examination had a change in diagnosis after videostroboscopy. There was only a 3 to 5% rate of change in diagnosis in patients with malignant lesions of the vocal cords and neurologic disorders of the larynx, respectively, indicating that invasive vocal fold carcinoma and vocal fold paralysis are correctly identified on indirect laryngoscopy. In 70% of the cases where videostroboscopy resulted in a change of diagnosis, a previously unappreciated benign vocal fold lesion was found. In another 19%, vocal fold bowing that had not been appreciated on indirect examination was identified.7 The benefits of videostroboscopy were confirmed by Sataloff et al, who reported that videostroboscopy, using a flexible laryngoscope, resulted in a change of diagnosis in 18% of patients and provided additional diagnostic information in 47% with changes in management based on these findings in 32%.8
Studies evaluating the accuracy of stroboscopy and the usefulness of specific stroboscopy parameters in the diagnosis of vocal fold pathology have illustrated the value of the technology. For example, stroboscopy in patients with bilateral vocal fold nodules typically demonstrates symmetric but reduced amplitudes of vibration, normal periodicity, an intact mucosal wave, and an hourglass glottic opening at maximal closure.7 Dailey et al. found that in patients with vocal fold nodules, videostroboscopic findings correlated with surgical findings 100% of the time.9 The accuracy of stroboscopy was also high in patients with vocal fold polyps who often present with asymmetric vibration and variable periodicity on videostroboscopy. With polyps, the mucosal wave may be present or absent and, due to the irregularity of the vocal fold margins, glottic closure is usually irregular and asymmetric.10 In patients with polyps, stroboscopy findings have also been correlated with surgical findings in up to 100% of cases.9 The situation is similar for vocal fold cysts. Typically unilateral, cysts cause asymmetric and aperiodic vibration. An hourglass glottic configuration results from protrusion of the medial vocal fold margin over the cyst, and the mucosal wave is frequently absent over the cyst.9–11 Videostroboscopic results have been found to correlate with surgical findings 78 to 100% of the time in patients with cysts.9,11
 Limitations of Videostroboscopy
Limitations of Videostroboscopy
Although the extent of benign vocal fold lesions and their impact on surrounding vocal fold structures can be determined using videostroboscopy, superficially invasive cancer of the larynx cannot be distinguished from a benign process with videostroboscopy. If a reduced mucosal wave is identified in the area of a suspicious lesion, this may be the result of a superficial pathologic process such as epithelial atypia but could also be the result of an invasive malignancy involving deeper structures. It must be kept in mind that videostroboscopy is a two-dimensional representation of a three-dimensional process, and it is not a reliable way to diagnose cancer or to determine the depth of its invasion.12
Similarly, it is difficult to see the medial glottal surfaces using videostroboscopy, and lesions in this area may not be identified. Thus, the evaluation of cancers involving the medial vocal fold surface may be incomplete using videostroboscopy, and sulcus vocalis, a lesion of the medial surface of the vocal folds, can be difficult to diagnose on videostroboscopy. Although sulcus vocalis may present with an absent or decreased mucosal wave and a defect of glottic closure, videostroboscopy has been unable to identify sulcus vocalis in some studies and correlates with surgical findings in only 69% of cases in other studies. Similarly, mucosal bridges are frequently missed with stroboscopy.8,9
In addition to not being appropriate for the evaluation of all lesions, videostroboscopy cannot be used effectively in all patients. Videostroboscopy requires a stable phonation frequency to activate the strobe. In other words, patients must have periodic phonation for optimal recording of vocal fold vibration with videostroboscopy. Patients with severe hoarseness, however, may have aperiodic phonation or significant, rapid changes in phonation frequency that preclude videostroboscopy. Images obtained when the strobe is unable to track due to aperiodic voicing jump from one part of the vibratory cycle to the other, rather than display vocal fold motion in a smooth sequence. Additionally, several seconds of phonation are required to activate the strobe and record a sample of vibration that is adequate for analysis. In patients who cannot phonate for 3 to 5 seconds at a stable frequency, videostroboscopy may not be possible. This may occur in up to 34% of individuals.7 Similarly, because significant aperiodicity occurs during the onset and offset of voicing, it is not possible to use videostroboscopy to evaluate vibration during those parts of phonation (Video Clips 1, 8, and 9).
Occasionally, an adequate or complete view of the larynx cannot be obtained with the rigid laryngoscope. Some patients may require topical anesthesia of the pharynx to tolerate the examination. Adequate examination may not be possible in up to 5% of patients due to anatomy or gag reflex.7 In those patients, videostroboscopy can be performed with a flexible scope, but the image quality and magnification is usually not as good. Please refer to Chapter 13 on performing the examination for a full discussion of strategies for obtaining the optimal videostroboscopic examination.
Although the best image quality is obtained by using a rigid endoscope for videostroboscopy, a transoral rigid examination requires an abnormal head position with the patient’s tongue out. Imaging is obtained during stable, periodic phonation and does not allow an analysis of what is happening during connected, articulatory speech production. As a result, functional dysphonias such as muscle tension dysphonia may be missed with videostroboscopy.
The analysis of the images recorded with videostroboscopy relies on visual perceptual judgments and is therefore susceptible to bias. Clinicians must avoid overdiagnosing or seeing pathology when none is present and also need to avoid missing pathology that is contributing to vocal symptoms. This may seem like a simple charge, but the task is complicated by the fact that vibratory features commonly associated with physiologic dysphonia are also frequently observed in the nondysphonic population and make it difficult to distinguish patients with physiologic dysphonia from nondysphonic subjects. Elias et al. discovered “abnormal findings” in 58% of healthy asymptomatic singers.13 In other words, the finding of abnormal vibratory characteristics in any one patient may or may not be related to their vocal complaints.
Further complicating the issue is the fact that our ability to subjectively rate vibratory characteristics is not very reliable. Individual scrutiny of each vibratory parameter reveals that none of them have shown a high degree of intrarater reliability. Some studies have shown that reliability improves with experience, whereas others found inexperienced raters to be as reliable as the more experienced raters.14,15 Looking at it another way, experience does not necessarily lead to greater reliability in rating videostroboscopic studies. Several factors, in addition to experience, have been shown to impact the way raters analyze videostroboscopic studies. Patient history has been demonstrated to influence severity ratings for the following parameters: vocal fold edge abnormalities, mucosal wave abnormalities, the identification of adynamic segments, and abnormalities of phase closure.16 Variations in nomenclature have also been identified and may be the source of some of the variability.15 Overall, taking all the vibratory parameters together, the agreement in diagnosis based on videostroboscopic studies has been found to be as low as 62%.15
As long as videostroboscopy remains a subjective method of vocal fold vibration analysis, there are likely to be problems with reliable rating and interpretation of the findings. Unfortunately, given the situation, small changes in vibratory characteristics that could indicate initial stages of disease or a trend during treatment may escape undetected by the clinician observer. Currently, there exists no standard reference for calibrating videostroboscopic images and therefore allowing quantitative measurements and detection of small variations. Attempts to quantify vibratory properties have been undertaken using a two-point laser dot calibration for measurement of distances. This method of laser triangulation has been found to be very accurate. When used to measure glottal width and vocal fold length, laser triangulation has demonstrated less than 5% variability.17
Until commercially available videostroboscopy systems are equipped with a method of quantitative measurement, it is important that clinicians using stroboscopy be familiar with the limitations of the technology and the subjective characteristics of the analysis. Steps can be taken to minimize rater influence on image analysis including the development of a working knowledge of the layered structure of the vocal folds, the normal appearance of the vocal folds, and how the mechanical properties of the vocal folds vary with changes in frequency and intensity.
In addition, the results of stroboscopy studies are influenced by the examiner’s instructions to the patient regarding the pitch and loudness of phonation during the examination. A standard protocol for every stroboscopy study should be developed. Using a protocol minimizes the variation of the study parameters secondary to the pitch and loudness of phonation and also allows for comparison of individual patients over time and the comparison of one patient with another. A standard protocol may include imaging during low-, normal-, and high-pitch phonation in addition to phonation in range of the patient’s speaking or singing problem. Documentation of vocal intensity at each pitch range should be performed, and the protocol may include loud and soft phonation at various pitches. Soft high-pitched phonation may provide differentiation of benign vocal fold lesions such as bilateral vocal fold nodules versus a unilateral vocal fold lesion with a contralateral reactive lesion.18
 Interdisciplinary Communication and the Videostroboscopy Report
Interdisciplinary Communication and the Videostroboscopy Report
Both otolaryngologists and speech-language pathologists perform videostroboscopy, although it is common for the otolaryngologist to refer a patient to the speech-language pathologist for videostroboscopy. Both specialties use the results of the videostroboscopic examination to evaluate patients with voice disorders but may have a different perspective based on their approaches to treatment. A speech-language pathologist may be more interested in the functional voicing technique demonstrated by the patient, whereas the otolaryngologist may be more interested in the anatomic pathology. Of course, these elements of the examination are not mutually exclusive. Optimal patient management involves a team approach with both the physician and the speech-language pathologist involved in the evaluation and management of any given patient. It is therefore critical that these two specialties communicate well with respect to the results of videostroboscopy.
The ideal videostroboscopy report not only includes a description of the vibratory characteristics of the vocal folds observed during the examination but also includes an interpretation of those findings with regard to optimal management. It must be kept in mind that the referral of a patient for videostroboscopy is usually done because the referring clinician is interested in evaluating the patient for evidence of disease to make treatment decisions. Perhaps the patient has an unexplained dysphonia or is a professional voice user with subtle voice difficulties. Perhaps the referring clinician wishes to further distinguish between a functional versus organic dysphonia. In any case, the information obtained from videostroboscopy will be integrated into a treatment plan designed to improve or resolve the patient’s voicing difficulties. It is important that the speech-language pathologist is able to determine if pathology exists that will respond to voice therapy, and it is important that the otolaryngologist is able to make plans for surgical treatment if that is needed. For example, when the evaluation of the vocal fold vibratory characteristics identifies stiffness, the examination interpretation must then help the clinician to determine if the stiffness is secondary to scarring or is due to hyperfunction.
Information gleaned from the videostroboscopic examination that is important for surgical planning often includes an evaluation of glottic competence. The glottic shape during maximal closure is important because defects in glottic competence may be amenable to surgical correction. In cases of unilateral vocal fold paralysis, for example, the position of the arytenoid cartilage is variable. In some patients, the arytenoid position is abducted, resulting in a significant posterior glottic opening during maximal vocal fold closure (Fig. 10.2). In other patients, the arytenoid cartilage is positioned in such a way that the posterior glottis is closed during voicing (Fig. 10.3). In the first case, an arytenoid adduction should be part of the surgical correction of the defect, and in the second case, arytenoid adduction is probably not necessary. The videostroboscopy report in a patient with vocal fold paralysis should include information about the position of the arytenoid cartilages and the closure of the posterior part of the larynx during voicing.
A description of the glottic configuration is also important in cases of vocal fold bowing due to presbyphonia. Subtle cases of presbyphonia may not be visible during indirect laryngoscopy, and videostroboscopy may be required to document this condition. A small anterior gap at maximal vocal fold closure may be all that is identified during the videostroboscopic examination. Very early presbyphonia can also present as mild abnormalities in the phase characteristics: a predominately open phase during modal phonation. A montage function can be used to identify the open phase characteristics (Fig. 10.1). When abnormalities of phase are identified on videostroboscopy, the question then becomes: Would the patient respond to voice therapy or would bilateral vocal fold medialization be of benefit? Other phonatory measures, such as maximum phonation duration, may be required to answer this question and can be integrated into the videostroboscopy report.
Benign vocal fold pathology will also likely impact the glottic configuration. Nodules typically result in an hourglass glottic configuration, whereas polyps and cysts cause irregularities of the glottic shape. It is important to distinguish between these types of pathology because the treatment approach can be very different. The interpretation of the videostroboscopy report in such cases should include information about whether or not the lesions identified are responsible for the patient’s voice complaints, and if so, will the lesions likely respond to voice therapy or is surgical correction required? If surgery is required, polyps ideally should be distinguished from cysts before surgery, as the surgical approach is different depending on the lesion. Nodules should be distinguished from a unilateral polyp or cyst with a contrecoup lesion (Fig. 10.4). An evaluation of vibratory symmetry as well as a description of the glottic configuration aid in making these distinctions and should be included in the interpretation of the results of videostroboscopy.
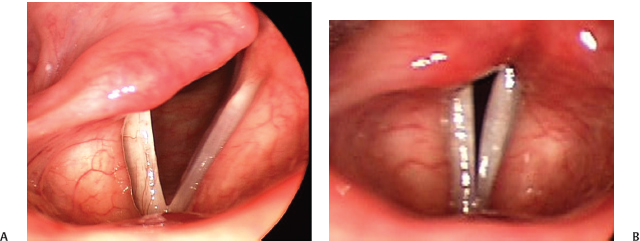
Fig. 10.2 (A) Unilateral right vocal fold paralysis with the vocal folds abducted. (B) When the vocal folds are adducted, there is a persistent posterior glottic gap identified. This patient would benefit from an arytenoid adduction as part of a vocal fold medialization procedure.
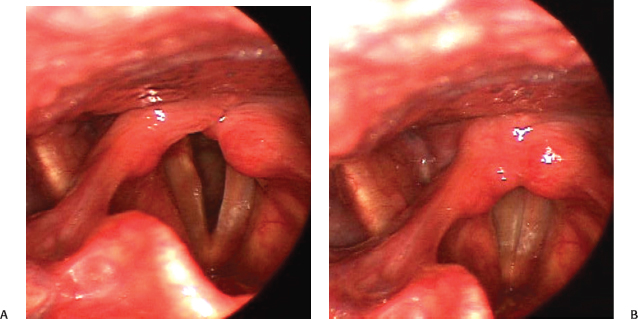
Fig. 10.3 (A) Unilateral left vocal fold paralysis with the vocal folds abducted. (B) During vocal fold closure for voicing, the posterior glottis is closed. Arytenoid adduction is not likely to be necessary. An evaluation of phase characteristics would determine the potential benefit of vocal fold medialization.
Ideally, clinicians who refer patients for videostroboscopy would communicate any specific clinical concerns to the stroboscopist before the examination to ensure that those concerns are addressed in the videostroboscopic examination and report. Performing the examination with a protocol can minimize the possibility that information critical to treatment decision-making will inadvertently be omitted from the examination. With respect to interpretation of the results of videostroboscopy, both specialties must be cognizant of the other’s point of view to maximize interdisciplinary communication for the patient’s benefit.
 Conclusion
Conclusion
In summary, the use of videostroboscopy has greatly improved our diagnostic capabilities, has improved patient education, and has allowed for examination documentation. Like all medical testing methods, it has some limitations. A thorough understanding of both the utility and the limitations is required for optimal efficacy in use of the technology. Parts III, IV, and V of this book provide the reader with detailed information about the technology, performing the examination, and videostro-boscopy study analysis.

Fig. 10.4 Is this a left vocal fold polyp with a contrecoup lesion or bilateral polyps?
References
1. Oertel MJ. Das Laryngo-stoboskop und die Larngosckopische Untersuchung. Arch Larngol Rhinol (Berl) 1895;3:1–6
2. Tsunoda A, Hatanaka A, Tsunoda R, Kishimoto S, Tsunoda K. A full digital, high definition video system (1080i) for laryngoscopy and stroboscopy. J Laryngol Otol 2008;122:78–81
3. Dejonckere PH, Bradley P, Clemente P, et al; Committee on Phoniatrics of the European Laryngological Society (ELS). A basic protocol for functional assessment of voice pathology, especially for investigating the efficacy of (phonosurgical) treatments and evaluating new assessment techniques. Guideline elaborated by the Committee on Phoniatrics of the European Laryngological Society (ELS). Eur Arch Otorhinolaryngol 2001;258:77–82
4. Chang HP, Chang SY. An alternative surgical procedure for the treatment of vocal fold retention cyst. Otolaryngol Head Neck Surg 2003;128:470–477
5. Finck C, Lefebvre P. Implantation of esterified hyaluronic acid in microdissected Reinke’s space after vocal fold microsurgery: first clinical experiences. Laryngoscope 2005;115:1841–1847
6. Ford CN, Roy N, Sandage M, Bless DM. Rigid endoscopy for monitoring indirect vocal fold injection. Laryngoscope 1998;108:1584–1586
7. Casiano RR, Zaveri V, Lundy DS. Efficacy of videostroboscopy in the diagnosis of voice disorders. Otolaryngol Head Neck Surg 1992;107:95–100
8. Sataloff RT, Spiegel JR, Hawkshaw MJ. Strobovideolaryngoscopy: results and clinical value. Ann Otol Rhinol Laryngol 1991;100(9 Pt 1):725–727
9. Dailey SH, Spanou K, Zeitels SM. The evaluation of benign glottic lesions: rigid telescopic stroboscopy versus suspension microlaryngoscopy. J Voice 2007; 21:112–118
10. Kaszuba SM, Garrett CG. Strobovideolaryngoscopy and laboratory voice evaluation. Otolaryngol Clin North Am 2007;40:991–1001, vi
11. Hernando M, Cobeta I, Lara A, García F, Gamboa FJ. Vocal pathologies of difficult diagnosis. J Voice 2008;22:607–610
12. Colden D, Zeitels SM, Hillman RE, Jarboe J, Bunting G, Spanou K. Stroboscopic assessment of vocal fold keratosis and glottic cancer. Ann Otol Rhinol Laryngol 2001;110:293–298
13. Elias ME, Sataloff RT, Rosen DC, Heuer RJ, Spiegel JR. Normal strobovideolaryngoscopy: variability in healthy singers. J Voice 1997;11:104–107
14. Rosen CA. Stroboscopy as a research instrument: development of a perceptual evaluation tool. Laryngoscope 2005;115:423–428
15. Chau HN, Desai K, Georgalas C, Harries M. Variability in nomenclature of benign laryngeal pathology based on video laryngoscopy with and without stroboscopy. Clin Otolaryngol 2005;30:424–427
16. Teitler N. Examiner bias: influence of patient history on perceptual ratings of videostroboscopy. J Voice 1995;9:95–105
17. Popolo PS, Titze IR. Qualification of a quantitative laryngeal imaging system using videostroboscopy and videokymography. Ann Otol Rhinol Laryngol 2008;117:404–412
18. Rosen CA, Murry T. Diagnostic laryngeal endoscopy. Otolaryngol Clin North Am 2000;33:751–758
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


