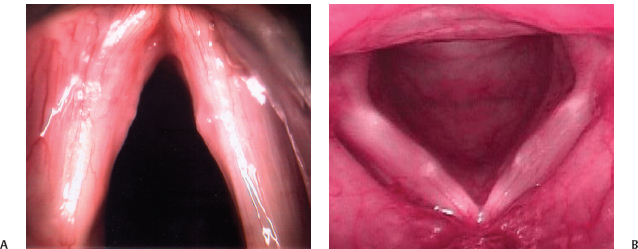
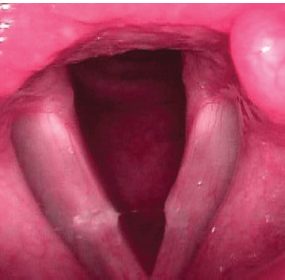
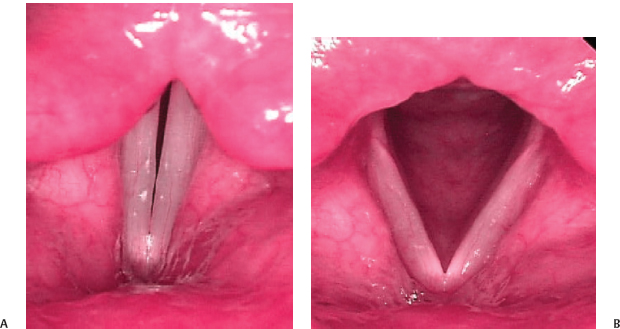
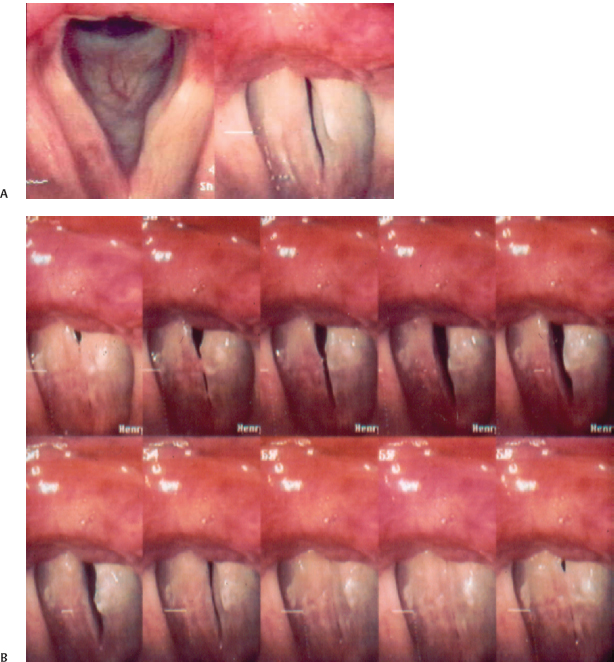
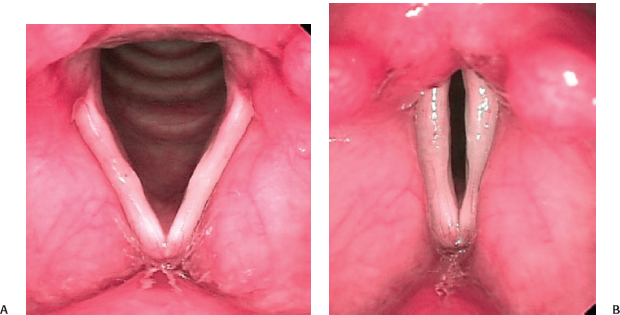
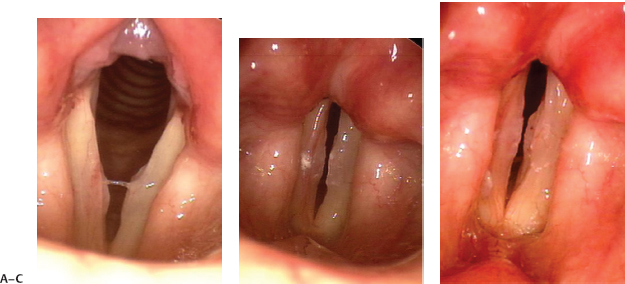
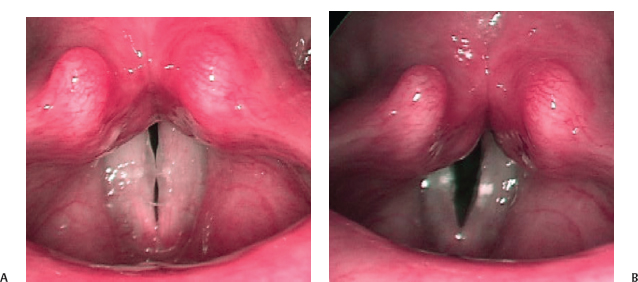
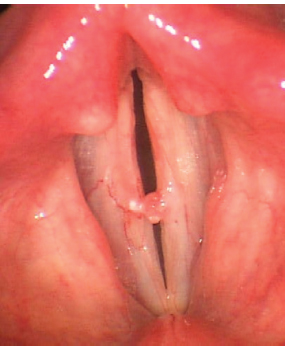
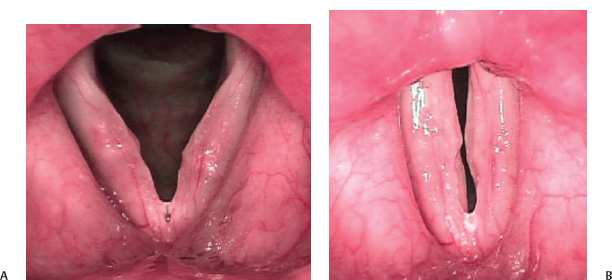
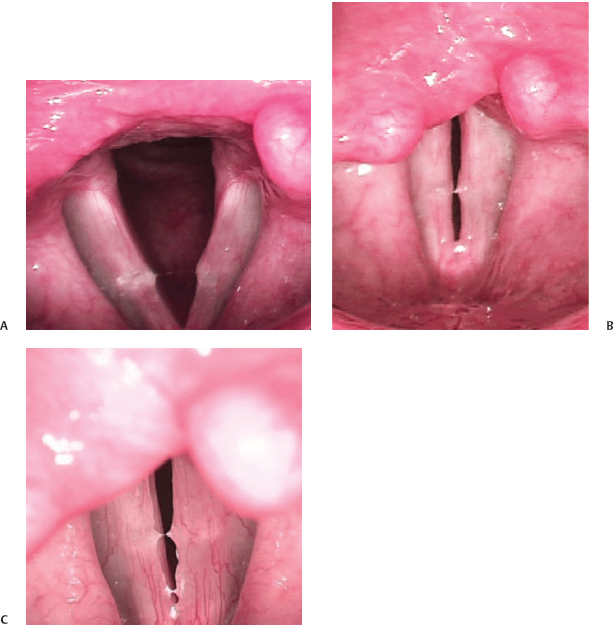
21 Vocal fold nodules are relatively symmetric areas of mucosal thickening located in the midportion of the musculomembranous vocal fold (Fig. 21.1).1,2 The cause of nodules is thought to be phonotrauma, which consists of excessive or loud voice use, excessively forceful glottic closure, and other inappropriate voicing techniques.3 Though this seems like a fairly straightforward definition, nodules can be easily confused with other benign swellings that occur in the midportion of the vibrating portion of the vocal fold, including polyps, cysts, pseudocysts, reactive nodules (opposite one of the other benign lesions), and simple edema (Figs. 21.2 to 21.4). Stroboscopy helps us differentiate between these various lesions because different lesions affect vocal fold vibration and mucosal wave propagation in different ways. Mucosal lesions (as opposed to submucosal) may dampen the mucosal wave but usually do not eliminate the wave. Lesions that involve the superficial layer of the lamina propria (submucosal, Reinke’s space) may abolish the wave altogether. Scarring, sulcus vocalis, and true cysts are the more common causes of an abolished wave because they effectively connect the mucosa to the underlying ligament (Fig. 21.5). Fig. 21.1 (A) Surgical view of hard fibrotic nodules. (B) Softer nodules located at the midportion of the musculomembranous vocal folds. Fig. 21.2 Left vocal fold cyst with reactive swelling of right vocal fold. Mucus is adherent to the right vocal fold swelling. Fig. 21.3 Left vocal fold polyp or pseudocyst with reactive swelling of right vocal fold. The masses most often confused with classic vocal fold nodules are small cysts and pseudocysts and small polyps.4 These lesions are covered in other chapters in detail. It should be noted, however, that even laryngologists, much less general otolaryngologists, cannot agree on the definition of these various lesions.1,5 Pathologists have not helped the situation. They will diagnose most benign vocal fold lesions microscopically as “nodules” even when the surgeon has observed that the lesions are different from each other grossly.3 Fig. 21.4 (A) Mild vocal fold edema at the midportion of the musculomembranous vocal folds. View with vocal folds adducted. (B) Mild vocal fold edema at the midportion of the musculomembranous vocal folds. View of patient in (A) but with vocal folds abducted. Fig. 21.5 (A) Left vocal fold cyst. (B) In patient from (A), mucosal wave seen on the right, not on the left. The most basic description of nodules is that they are a thickening of the mucosa in the midportion of the musculomembranous portion of the vocal fold; that is, the vibratory portion. They are, therefore, located halfway between the anterior commissure and the vocal process of the arytenoid cartilage. They are generally very symmetric. Early nodules, or prenodules, may simply be edema of the mucosa, whereas chronic nodules may be fibrotic (Video Clips 18 and 40). This is differentiated from a polyp in which the mucosa is generally normal, or thin, and the bulk of the mass is a submucosal gelatinous matrix, although there are many variations of the composition of polyps (Video Clips 19 and 23). A true cyst has a well-defined capsule and is either a mucus retention cyst or an epidermoid cyst (Video Clip 26). A pseudocyst appears similar to a true cyst, but when dissected out, or examined histologically, there is no true capsule. Dikkers and Schutte in 1991 suggested the following diagnostic criteria for the most common glottic lesions. This was similar to Kleinsasser’s definitions.6 With vocal fold nodules, the superficial layer of the lamina propria and the vocal ligament are normal. The mucosa is free to slide over the underlying vocal ligament, even if the mucosa, itself, is abnormal. Stroboscopy shows the mucosal wave flowing through a nodule (soft early nodule) (Fig. 21.6) or the nodule “riding” the wave (harder fibrotic nodules) (Fig. 21.7), but the wave is not abolished (Video Clip 18). It may be dampened, especially if the nodules are hard and fibrotic or exceptionally large (Video Clip 40). A true cyst abolishes the wave at the location of the cyst, although the wave may flow around the cyst (anterior and posterior to the cyst) (Fig. 21.5) (Video Clip 26). The true cyst, residing in the superficial layer of the lamina propria, is adherent to both the mucosa and the vocal ligament, thereby tethering these two structures and preventing the normal sliding motion of the mucosa over the vocal ligament.7 Pseudocysts have variable effects on the wave. The mucosal wave flows through a soft polyp, especially the small sessile polyps that appear similar to nodules (Fig. 21.8). Harder pedunculated polyps generally interfere so much with closure and vibration that the mucosal wave is difficult to see (Fig. 21.9). Fig. 21.6 (A) Soft vocal fold nodules during vocal fold abduction. (B) Soft vocal fold nodules. Mucosal waves are normal. Fig. 21.7 (A) Large fibrotic nodules with vocal folds abducted. (B and C) Large fibrotic nodules “ride” the mucosal waves. Polypoid vocal folds (Reinke’s edema, polypoid degeneration, polypoid corditis), in which the entire vibratory portion of the vocal fold (anterior commissure to the vocal processes) is severely edematous, will have larger than normal mucosal waves, and the appearance is so different from vocal fold nodules that confusion regarding these two entities is rare (Video Clip 36). Nodules, however, may be present on the surface of polypoid vocal folds. In this case, the nodule is seen to ride a very large mucosal wave (Fig. 21.10). Vibration of the vocal folds is also influenced by the mass of the fold and closure. Vocal fold nodules affect both these factors. Vocal fold nodules interfere with closure by making premature contact at the midportion of the folds, resulting in an hourglass configuration. With less than complete closure, air leaks through the open gaps, decreasing the power transferred to the vocal fold edges and decreasing the amplitude of vibration and the size of the mucosal waves. The increased mass of the vocal fold edge also dampens vibration of the vocal fold. Whereas classic vocal fold nodules are symmetric, slight asymmetries often exist that affect each vocal fold slightly differently. Vibration may become aperiodic or asymmetric if the difference between the sides is significant (Video Clip 45). All of the benign lesions of the musculomembranous vocal folds will be more apparent at higher pitch, with the vocal fold stretched out under more tension. It is, therefore, important to view the folds all at aspects of the patient’s dynamic range. Fig. 21.8 (A) Right vocal fold pseudocyst or polyp with incomplete closure. (B) Right vocal fold pseudocyst or polyp. Mucosal wave is intact. Fig. 21.9 Hard pedunculated left vocal fold polyp. The differentiation between vocal fold nodules and similar lesions is not purely academic. Treatment varies for these different lesions. Voice therapy is the primary treatment for vocal fold nodules, whereas surgery is often required for polyps, pseudocysts, and true cysts.8 Soft vocal fold nodules generally respond better to voice therapy than do the more chronic fibrotic nodules, nevertheless therapy should be tried in all cases of vocal fold nodules. Occasionally, when the diagnosis is not clear, the response to therapy will reveal the nature of the vocal fold abnormalities (Fig. 21.11). There are many cases in which the diagnosis of vocal fold nodules was made without stroboscopy, but the patient did not respond to therapy as expected, and the lesions were later found not to be nodules when stroboscopy was used for better evaluation.4,9 Similarly, a surgeon who thought that he or she was about to remove nodules was instead confronted intraoperatively with a cyst. Fig. 21.10 (A) Nodules on surface of polypoid vocal folds viewed with vocal folds abducted. (B) Nodules on surface of polypoid vocal folds viewed during phonation. Fig. 21.11 (A) The lesions seen in this figure were initially thought to be nodules although mucosal wave was seen on the right only. View with vocal folds abducted. (B) View with vocal folds adducted of bilateral mid-membranous lesions initially thought to be nodules. (C) View during phonation showing mucosal wave on right prior to voice therapy. In summary, differentiating between classic vocal fold nodules and those other benign vocal fold lesions that have a similar appearance is important for prognosis and treatment decisions and is best done with videostroboscopy. An easy way to remember how to differentiate nodules from cysts is that nodules are located in the midportion of the musculomembranous fold, are bilaterally symmetric, and generally do not affect the mucosal wave, whereas cysts are usually unilateral and abolish the mucosal wave at the site of the cyst. Cysts can be located anywhere on the vocal fold. 1. Dikkers FG, Schutte HK. Benign lesions of the vocal folds: uniformity in assessment of clinical diagnosis. Clin Otolaryngol Allied Sci 1991;16:8–11 2. Rosen CA, Murry T. Nomenclature of voice disorders and vocal pathology. Otolaryngol Clin North Am 2000;33:1035–1046 3. Rubin JS, Yanagisawa E. Benign vocal fold pathology through the eyes of the laryngologist. In: Rubin JS, Sataloff RT, Korovin GS, eds. Diagnosis and Treatment of Voice Disorders, 2nd ed. Clifton Park, NY: Thomson Delmar Learning; 2003:69–86 4. Woo P, Colton R, Casper J, Brewer D. Diagnostic value of stroboscopic examination in hoarse patients. J Voice 1991;5:231–238 5. Chau HN, Desai K, Georgalas C, Harries M. Variability in nomenclature of benign laryngeal pathology based on video laryngoscopy with and without stroboscopy. Clin Otolaryngol 2005;30:424–427 6. Kleinsasser O. Microlaryngoscopic and histologic appearances of polyps, nodules, cysts, Reinke’s edema, and granulomas of the vocal cords. In: Vocal Fold Histopathology, a Symposium. San Diego, CA: College Hill Press; 1986:51–56 7. Alberti PW. The diagnostic role of laryngeal stroboscopy. Otolaryngol Clin North Am 1978;11:347–354 8. Sataloff RT, Hawkshaw MJ. Common medical diagnoses in voice patients: an overview. In: Benninger MS, ed. Benign Disorders of the Voice. Alexandria, VA: American Academy of Otolaryngology–Head and Neck Surgery Foundation, Inc.; 1996:45–71 9. Sataloff RT, Spiegel JR, Hawkshaw MJ. Strobovideolaryngoscopy: results and clinical value. Ann Otol Rhinol Laryngol 1991;100(9 Pt 1):725–727
Vocal Fold Nodules

 Cyst: A unilateral lesion with a smooth surface, immobile during phonation, usually on the middle third of the vocal fold and often of a yellowish fluid-like appearance (Video Clip 26).
Cyst: A unilateral lesion with a smooth surface, immobile during phonation, usually on the middle third of the vocal fold and often of a yellowish fluid-like appearance (Video Clip 26).
 Reinke’s edema: A condition with a unilateral or bilateral bleach-white swelling of the vocal fold, filled with fluid, is sessile, and very mobile during phonation (Video Clip 36).
Reinke’s edema: A condition with a unilateral or bilateral bleach-white swelling of the vocal fold, filled with fluid, is sessile, and very mobile during phonation (Video Clip 36).
 Polyp: A unilateral lesion on the anterior third of the vocal fold, often on the free edge, sessile or pedunculated, and very mobile when pedunculated—a pedunculated polyp on the free edge can sometimes be heard popping through the glottis during the initiation of a phonation (Video Clips 19, 23, and 46).
Polyp: A unilateral lesion on the anterior third of the vocal fold, often on the free edge, sessile or pedunculated, and very mobile when pedunculated—a pedunculated polyp on the free edge can sometimes be heard popping through the glottis during the initiation of a phonation (Video Clips 19, 23, and 46).
 Nodules: Small lesions occurring on both sides of the larynx, strictly symmetrical on the border of the anterior and middle third of the vocal folds, and usually immobile during phonation—they can be divided, with the aid of stroboscopy, into the early spindle type (soft) or more chronic, white, cone-like form (hard)1 (Video Clips 18 and 40).
Nodules: Small lesions occurring on both sides of the larynx, strictly symmetrical on the border of the anterior and middle third of the vocal folds, and usually immobile during phonation—they can be divided, with the aid of stroboscopy, into the early spindle type (soft) or more chronic, white, cone-like form (hard)1 (Video Clips 18 and 40).
 Summary: The Effect of Nodules on Vocal Fold Vibratory Characteristics
Summary: The Effect of Nodules on Vocal Fold Vibratory Characteristics
 Nodules are due to phonotrauma.
Nodules are due to phonotrauma.
 Nodules are bilateral, symmetric, and located in the mid-membranous portion of the vocal fold.
Nodules are bilateral, symmetric, and located in the mid-membranous portion of the vocal fold.
 The mucosal wave is normal with nodules or slightly dampened if the nodules are particularly fibrotic.
The mucosal wave is normal with nodules or slightly dampened if the nodules are particularly fibrotic.
 The nodules result in an hourglass glottic configuration.
The nodules result in an hourglass glottic configuration.
 The amplitude of vibration will be decreased secondary to the open glottic configuration and the mass of the nodules on the folds.
The amplitude of vibration will be decreased secondary to the open glottic configuration and the mass of the nodules on the folds.
 If the nodules are symmetric, there is nor mal symmetric vibration. If the nodules are asymmetric, there may be asymmetry of vibration.
If the nodules are symmetric, there is nor mal symmetric vibration. If the nodules are asymmetric, there may be asymmetry of vibration.
References
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


