CHAPTER 57 Visualization of the Larynx
In most states, LVES, HSDI, and NBI can be performed by either an otolaryngologist or a qualified speech-language pathologist.1 Each professional brings a different perspective and training to the process, and the most thorough examinations are typically conducted in a team setting. The otolaryngologist is responsible for assessing mucosal health and diagnosing laryngeal pathology; the speech-language pathologist is interested in the vibratory patterns during various voicing conditions, the behavior of the laryngeal and supralaryngeal structures during phonation, and how treatment probes alter phonatory physiology. As team members work together over time, they often learn from each other and develop common skill sets.2
Endoscopes
Rigid Endoscopes
Advantages
Rigid endoscopes used with LVES are usually 70- or 90-degree scopes. Rigid scopes have the advantage of high resolution with bright, clear pictures. Contrast is excellent, there is a large selection of viewing angles, and the image is more accurately magnified than with a flexible endoscope. The examination is simple and does not usually require topical anesthesia.2–4
Disadvantages
The primary limitation of the rigid endoscope is that phonation is limited to sustained vowels, most commonly “ee.” Because visualization with a 70-degree rigid endoscope usually requires an extended neck and protruded tongue, the size of a glottic gap might appear exaggerated with the rigid endoscope.5 To counteract this problem, Rammage and colleagues2 suggest a lateral approach to the larynx to decrease neck extension during the examination. Alternatively, a 90-degree endoscope does not require the same amount of neck extension as the 70-degree endoscope does. A second limitation is that the mobility of the arytenoids might not be accurately assessed via rigid endoscopy; often, it appears as if there is a vocal fold paresis when the perceived lack of motion is, in actuality, an artifact of the tongue protrusion and neck extension. Lastly, disorders more evident in connected speech than in sustained vowels (e.g., muscle tension dysphonia and spasmodic dysphonia) are not as well documented with rigid endoscopy as they are with flexible endoscopy.
Technique
Defogging the endoscopes can be a challenge, because sterilizing beads can cause damage to both the lens and the patient. Alternatives include liquid defogger, hot (not boiling) water, soap film, surgical wax, and holding the endoscope lens briefly against the patient’s cheek or the side of the tongue. The examination is generally tolerated without topical anesthesia, but a small amount of benzocaine topical spray or a similar product is sometimes useful and does not appear to affect examination results.6
Troubleshooting
A good-quality examination means that the image is in focus, that it is large enough to show small mucosal irregularities, and that it is bright enough to show details (but not so bright as to obscure them). Contrasting color is important for differentiating subtle lesions and vascular changes. Ideally, an examination includes both a wide-angle view of the larynx and a close-up view of the vocal folds. The stroboscopic portion of the examination should include several complete stroboscopic cycles at the patient’s most comfortable pitch and loudness (MCPL) in addition to the rest of the protocol (see “Assessment”). Common imaging problems and solutions are listed in Table 57-1.
Table 57-1 Common Problems and Solutions for Laryngeal Endoscopy and Stroboscopy
Flexible Endoscopes
Advantages
The primary advantage of the flexible endoscope is the ability to view the larynx dynamically—that is, during natural functions such as speech and singing. Arytenoid mobility and the glottic gap can be more accurately described with flexible than with rigid endoscopy because of the neutral tongue and neck positions.5 Flexible endoscopy also allows the clinician to assess the nasal cavity and velopharyngeal port during the same examination. Flexible endoscopy is preferred when the question is one of movement rather than structure or mucosal health. It is particularly useful for disorders such as spasmodic dysphonia and muscle tension dysphonia, in which the voice problem is more obvious during speech than in sustained vowels, and vocal fold motion impairment, where having the patient sniff through the nose allows the examiner to assess subtle motion.
Videoendoscopy and Stroboscopy
Endoscopy: Assessment Using Continuous Light
Protocol
Endoscopic parameters that require only continuous light (as opposed to the xenon light of stroboscopy) include laryngeal structure, arytenoid and vocal-fold motion, color and quantity of mucus, vascularity, supraglottic activity or compression, and deformation of vocal fold edges. The tasks during this portion of the examination include rest breathing, deep breathing, easy cough or throat clear, and laryngeal diadochokinesis, which consists of rapid repetitions of “ee” with glottal stops between productions. Laryngeal diadochokinesis is a useful measure, and production rates of four to six syllables per second are considered normal.7 Difficulty with accurately and rhythmically producing the voice onset/offset gesture has been found in patients with neurologic impairment.8,9 If a flexible endoscope is used, several other parameters can be assessed, including repetitions of a short “ee” followed by a quick sniff through the nose, a standard set of phrases or sentences, and conversational speech if voice quality during the endoscopic examination is not consistent with what was heard before it. Examination of velopharyngeal function is indicated if nasal emission or hypernasality is heard. At a minimum, soft palate and lateral pharyngeal wall motion should be assessed during a sustained vowel and a voiceless fricative, as well as during words or phrases with nasal-oral consonant transitions. A sample protocol is outlined in Box 57-1.
Laryngeal Structure
The valleculae, pyriform sinuses, epiglottis, aryepiglottic folds, ventricular folds, and posterior glottic rim should be examined. Lowered pitch during sustained “ee” widens the angle, allowing better visualization of the valleculae. Abnormalities and asymmetries of laryngeal structure are noted. An omega-shaped epiglottis is a common variant in men, but it is rare in women.7,10 Signs of laryngeal irritation or possible laryngopharyngeal reflux are noted; these primarily include edema, erythema, surface irregularities, and lesions of the posterior larynx.11–14 The specificity of signs for reflux is still being evaluated. In particular, interarytenoid bar, arytenoid medial wall erythema, and posterior pharyngeal wall cobblestoning have been found in a substantial number of “normal” volunteers.13
Arytenoid and Vocal Fold Motion
Movement and position of the arytenoids inform the examiner about the integrity of the cricoarytenoid joint and the recurrent laryngeal nerve. Arytenoids are typically described as mobile or immobile, symmetric or asymmetric, and upright or rotated. Immobility is further described by position: median, paramedian, intermediate, or lateral. Motion of the arytenoid should be described separately from movement of the posterior third of the vocal fold because sometimes the arytenoid is mobile when the vocal fold is fixed. Mobility is rated when patients phonate then breathe, and during laryngeal diadochokinesis, cough, whistling, and sniff. The etiology of the motion impairment, along with particular characteristics such as arytenoid position, gap size, shape, and vocal-fold plane difference, can influence management strategy as described in Chapters 66 through 68.
Supraglottic Activity
Supraglottic activity refers to any abnormal motion above the true vocal folds. Examples are tremor of the larynx or pharynx, other involuntary contractions (e.g., myoclonic movements), and compression of the supraglottic structures. Supraglottic movements help tease apart neurologic voice disorders from disorders caused by abnormal muscle tension; tremor and myoclonic movement are evidence of a neurologic disorder, whereas sustained constriction is more typically found in muscle tension disorders. Constriction is often categorized by direction (anteroposterior or lateromedial) and frequency (constant or intermittent). Anteroposterior constriction during phonation is shown in Figure 57-1, and lateromedial constriction in Figure 57-2. The Stroboscopy Evaluation Rating Form proposed by Poburka15 displays a superior view diagram of the vocal folds with superimposed concentric circles on which raters estimate the extent of constriction. Aryepiglottic narrowing or dilation and pharyngeal shape for different vowels can alter vocal-fold vibratory characteristics.2,16,17
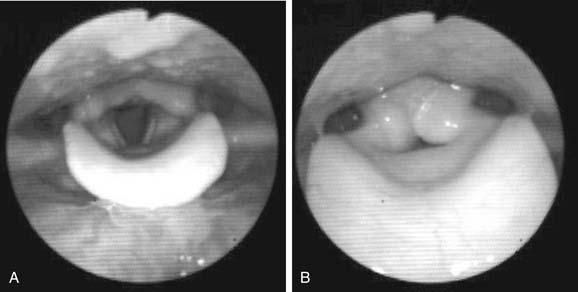
Figure 57-1. A, Vocal folds during respiration. B, Vocal folds with anteroposterior constriction during phonation.
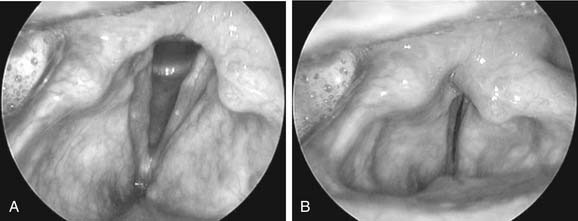
Figure 57-2. A, Vocal folds during respiration. B, Vocal folds with lateromedial constriction during phonation.
The frequency and severity of supraglottic constriction in subjects without voice disorders is still somewhat uncertain, although it is clear that both anteroposterior and lateromedial constrictions are sometimes normal variants.18–20 Stager and associates20 found that supraglottic movements were present at the initiation of phonation in normal controls. Behrman and colleagues18
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


