Chapter 79 Vertical strabismus
Physiology
The cyclovertical muscles have a triple function that includes a vertical, torsional, and, to a lesser degree, horizontal action. With head tilt right or left, there is a small partial compensatory torsional rotation of each eye, which corrects for about 5−10% of the head tilt.1 This comes from stimulation of the intorters (superior oblique and superior rectus) in the eye on the side to which the head is tilted, and the extorters (inferior oblique and inferior rectus) in the fellow eye, and forms the basis for the Bielschowksy Head Tilt Test and the Parks’ 3-Step Test.2 Although the vertical rectus muscles have their main vertical action in adduction, they are still the primary elevators and depressors across the horizontal gaze fields. Oblique muscles have a relatively weak vertical action. If the superior rectus is detached from the globe, the inferior oblique alone cannot elevate the eye above the midline. The superior oblique, however, has a stronger vertical action than the inferior oblique.
Patient evaluation
History
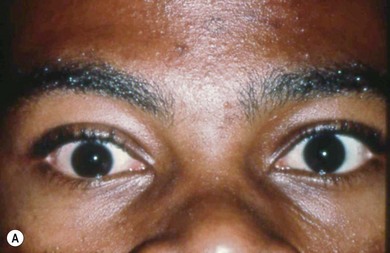
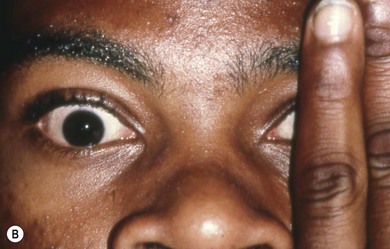
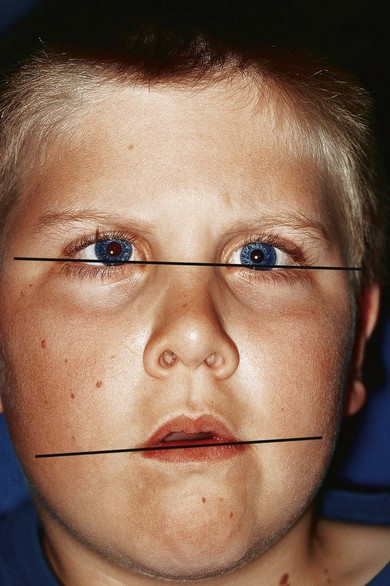
Before measuring the deviation, observe whether the patient has a spontaneous compensatory head posture (CHP) with visual effort. Although there are many causes for CHPs, I find they mostly serve to place the eyes in a gaze field in which the deviation is less, or to damp nystagmus (see Chapters 87, 88, and 89). The presence of facial asymmetry typically identifies the CHP as dating back to early childhood. There is a shortening of the midface between the horizontal canthus laterally and the corner of the child’s mouth on the side to which the head is habitually tilted3 (Fig. 79.1). Measure the deviation with the head posture using the prism and alternative cover test, and then in the head erect position. Although a diagnosis can often be made by just measuring a patient in seven fields of gaze (primary, up, down, right and left) and on head tilt right and left, an optimum treatment plan often requires additional measurements in the four oblique fields. Ductions and versions should be assessed with particular attention to the presence of overelevation or overdepression in the oblique fields. If there is overelevation of the adducting eye on side gaze, do a cover test in that gaze field to ascertain if the vertical deviation is a manifestation of DVD or true inferior oblique overaction.
Determine if the deviation is dissociated or not. With a non-dissociated deviation, a hypotropia is present in the contralateral eye when fixation is with the higher eye. Unless a secondary deviation is present due to paresis or restriction, the hypotropia in one eye will be of equal size to the hypertropia of the other eye. With DVD, the hypotropia of the fellow eye is either smaller or absent when fixation is with the eye with the DVD (see section on Dissociated vertical divergence).
The Parks’ 3-Step Test will tell, in theory, which of the eight cyclovertical muscles is paretic; however, in practice it works best for confirming the diagnosis of unilateral superior oblique palsy.2,4 Even in cases of isolated superior or inferior rectus palsy, it may be misleading. Most importantly, it does not tell whether a vertical strabismus is due to a palsy of one of the cyclovertical muscle, but is based on the assumption that it is. Box 79.1 lists some of the common situations in which the 3-Step Test leads to an incorrect diagnosis (see  Video 79.1). The man in this video developed vertical diplopia immediately after closed head trauma from a motor vehicle accident. He had a left hypertropia which increased in right gaze and on left head tilt, thus meeting the 3-Step Test criteria for a left superior oblique palsy. In fact, he had an orbital floor fracture in his right eye. He consistently fixed with his right eye due to mild amblyopia in his left eye. His diplopia resolved when the fracture was repaired
Video 79.1). The man in this video developed vertical diplopia immediately after closed head trauma from a motor vehicle accident. He had a left hypertropia which increased in right gaze and on left head tilt, thus meeting the 3-Step Test criteria for a left superior oblique palsy. In fact, he had an orbital floor fracture in his right eye. He consistently fixed with his right eye due to mild amblyopia in his left eye. His diplopia resolved when the fracture was repaired
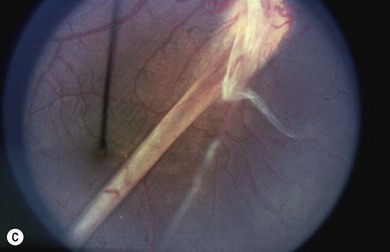
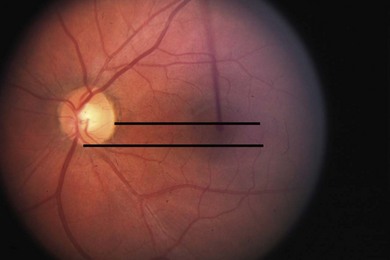
You should test for the presence of torsion both objectively and subjectively. The latter is accomplished with the double Maddox rod test using two red lenses, because the use of one red and one white lens frequently leads to a localization artifact; if the eye behind the white lens is the one that is torted, the patient will frequently perceive the torsion as being in the eye behind the red lens.5 However, even when I use two red lenses, I sometimes find that the double Maddox rod test just tells me the total amount of torsion between the two eyes, and may be misleading with respect to localizing to the specific eye affected. Objective torsion is determined with the indirect ophthalmoscope and may be more useful in determining which eye actually is torted.6 Normally the position of the fovea should be level with the lower one-third of the optic disk (Fig. 79.2). The absence of subjective torsion in the presence of objective fundus torsion usually means the deviation is long-standing and sensory adaptations have occurred. If a patient describes torsion, determine if the patient can fuse when the vertical and horizontal deviations are offset with prisms. If the patient can fuse comfortably despite the presence of torsion, it may be possible to ignore the torsion when designing a surgical strategy. If they cannot fuse, there may be a central disruption of fusion. Testing on the synoptophore, which can offset the torsion and may determine whether you can expect fusion if the strabismus is successfully treated.
General diagnostic pointers
1. Are history and symptoms helpful in determining etiology? Is there diplopia, childhood strabismus (if the patient is an adult), and is there DVD?
2. Is incomitance greater vertically or horizontally? If it is greater vertically, consider a restriction or palsy of a vertical rectus. If the largest difference is horizontal, consider an oblique problem.
3. Is there a limitation of rotation? Differentiate restriction from paresis with forced duction and active force generation testing.
4. Is there substantial torsion? If so, consider oblique problems or a vertical restriction.
5. Might the patient be fixing with the involved eye? Always consider this if there is asymmetric corrected visual acuity. Check for a secondary deviation.
General treatment principles
In general, surgery on the inferior rectus or superior oblique is least “forgiving.” Inferior rectus recessions of 5 mm or more may cause a lag of that eye in downgaze unless there was a hypotropia that increased in downgaze prior to surgery. Also, large recessions of the inferior rectus may cause lower eyelid retraction postoperatively, minimized by advancement of the capsulopalpebral head at surgery.7 Large resections of the inferior rectus muscle may cause narrowing of the palpebral fissure, and large recessions of the inferior rectus using a suspension technique (hangback adjustable suture) have a higher incidence of muscle slippage or non-adherance. This is probably caused by the shorter arc of contact of that muscle, which can cause the muscle to lose apposition with the globe in downgaze after surgery if the muscle is not fixed to the sclera.8 Slippage can be prevented by using the semi-adjustable suture technique,9 or a non-absorbable suture.
Specific clinical entities
Pseudohypertropia
Some patients may appear to have a hypertropia when in fact they do not. These include cases of orbital dystopia, anterior segment anomalies, or vertical angle kappa (Fig. 79.3). This latter may be due to a displaced fovea secondary to retinopathy of prematurity (see Chapter 43) or other causes of retinal dragging.