Chapter 67 Child maltreatment, abusive head injury and the eye
RISK FACTORS FOR CHILD MALTREATMENT
PRESENTATION OF CHILD ABUSE VICTIMS TO THE OPHTHALMOLOGIST
EVALUATION OF CHILD MALTREATMENT LITERATURE
OPHTHALMIC FEATURES OF PHYSICAL ABUSE
OPHTHALMOLOGY OUTCOME ON FOLLOW-UP OF ABUSIVE HEAD INJURY
DIFFERENTIAL DIAGNOSIS OF RETINAL HEMORRHAGES
SYSTEMIC FEATURES OF ABUSIVE HEAD INJURY
BIOMECHANICS OF RETINAL HEMORRHAGES
MUNCHAUSEN’S SYNDROME BY PROXY
THE OPHTHALMOLOGIST AND CHILD MALTREATMENT
Definitions
• Child maltreatment covers both child abuse and neglect.1
• Child maltreatment is defined as any act, or series of acts, of commission or omission by a parent or caregiver that results in harm, potential harm, or threat of harm to a child (Box 67.1).
Epidemiology
Child maltreatment is common with a total of 581 911 cases reported in the year ending March 2008 in England2 and Wales.3 In the USA 1 in 58 children suffers from maltreatment.4 Child maltreatment is often missed or unrecognized and the figures presented may underestimate the problem.
The incidence of severe physical abuse is highest (54/100 000) in infants less than a year old and less in older children (9.2/100 000 in children 1−4 years old and 0.47/100 000 in children 5−13 years).5
Ophthalmological features are commonly associated with abusive head injury which represent 1.8% of physical abuse.6 The incidence of abusive head injury varies between 14.2/100 000 and 33.8/100 000 infants in the UK, and is commonest in infants less than 6 months of age.7,8 Abusive head trauma accounts for the majority of fatal or life-threatening injuries due to abuse in infants.5
Risk factors for child maltreatment
The risk factors for child maltreatment include social, family, and community factors. Perpetrators may be those who are responsible for the care and supervision of their victims. Parents either acting alone, or with another person, account for 71% of abuse of children in their care. Though there is no single profile that fits all perpetrators, a number of common characteristics are reported in many studies (Box 67.2).
Presentation of child abuse victims to the ophthalmologist
In the majority of cases the child is referred to the ophthalmologist by pediatricians who suspect an abusive injury. However, it is incumbent on the ophthalmologist to not only recognize cases that occasionally present to them with bruising or unexplained injury who may be maltreated, but to also refer them on for multiagency assessment of possible abuse or neglect.9
The presenting features alerting the professional to child maltreatment include:
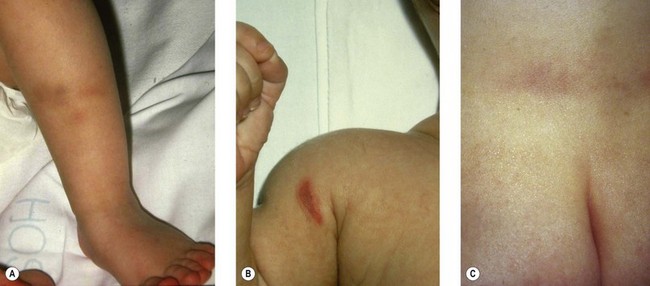
a. Physical signs of unusual bruising in non-mobile infants for which there is no explanation (Fig. 67.1). Bruising in non independently mobile infants is very rare (< 1%)10 and bruising that is periocular in infants should be investigated when there is no verifiable explanation. Other signs include bites, burns, and scalds; ligature or strangulation marks and abrasions may accompany a story without a plausible explanation.
b. Anogenital injuries and sexually transmitted diseases in children point to sexual abuse.
c. Clinical presentations include an apparent life-threatening event (where the child presents floppy and apneic), seizures, ingestion of poisonous substances, nasal bleeding, near drowning, and unusual or poor attendance at medical services or school due to ill health.
d. An unkempt child with infestations or tooth decay may signify neglect.
e. Behavioral signs include sexualized behavior, “frozen watchfulness” of a withdrawn child, overt hostility or friendliness of the carers, and a child who acts aggressively.
Management
Clinical presentation to an ophthalmologist may be either:
1. The child is referred as part of a multidisciplinary assessment where abusive head injury is suspected.
2. An ophthalmologist suspects maltreatment during a consultation for the presenting complaint or presentation of an unkempt dirty child or an unusual injury or pattern of bruising is noticed without an innocent explanation. The ophthalmologist has the duty of care to safeguard the rights of the child by referral to the named child protection lead doctor or a named child protection nurse. This may initiate a multiagency assessment to confirm or rule out maltreatment. Contact details of the child protection team are kept in a prominent and accessible place.
Clinical records
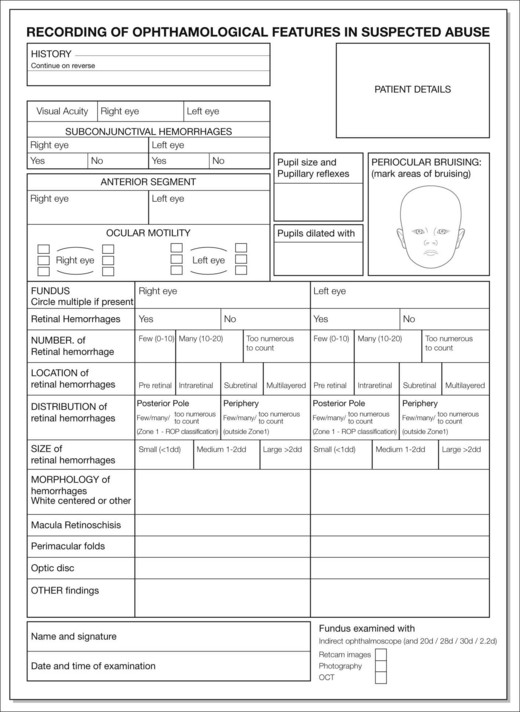
This should contain a detailed history, supplementing information recorded by other medical personnel and a thorough clinical examination. Local protocols for child protection records vary; however, completion of a standardized ophthalmology clinical record supplemented with wide field retinal photography (i.e. Retcam 130) improves documentation, which is helpful when giving evidence in family or criminal courts11,12 (Fig. 67.2).
There are a number of ways of describing the distribution, location, and types of retinal hemorrhages. Their use in routine clinical practice, however, has not been evaluated.13,14 Recent systematic reviews of retinal hemorrhages in abusive injury identified the need for consistent and standardized description of retinal findings that would hold under scrutiny in medico-legal cases and help with future research in differentiating patterns of retinal hemorrhages from various causes.
Fluorescein angiography and optical coherence tomography help demonstrate retinal perfusion and vitreo-retinal interface pathology, but their use is yet to be established in practice.15,16
Each page of the clinical record should be identified with the child’s name and date of birth. The entry should include the clinician’s name, designation, signature, date, and time of examination. It should include a differential diagnosis, suggesting appropriate further investigations. A standard list of investigations in suspected abusive head injury has been suggested along with a multidisciplinary assessment involving medical teams, social services, and the police.17
A date for a follow-up examination should be clearly indicated on the clinical record.
Examination
• External eye examination should include descriptions, drawings, and photography of any periocular injury or subconjunctival hemorrhages.
• If the condition of the child permits, assessment of visual acuity and ocular motility should be noted.
• An assessment of the pupillary reactions, anterior chamber, and lens position should be undertaken before the pupils are dilated for assessment of the fundus. Poor pupillary responses are strongly associated with increased mortality and poor visual outcomes.18
• Examination of the retina with an indirect ophthalmoscope and a wide field lens following dilation of the pupils with short-acting mydriatics (phenylephrine 2.5% and tropicamide 1%) is standard practice. Pupillary dilation affects neurological observations and should only be undertaken following discussion with the physicians under whose care the child is admitted. Descriptions of retinal findings should include their distribution, location in terms of the retinal layers, morphology, and severity in terms of number and size.
Medico-legal issues19
The case considered may be subject to:
1. Care proceedings in a civil or family court: a verdict reached by the court based on the “balance of probability.”
2. Criminal court proceedings: a verdict is reached when it satisfies the statement of “beyond reasonable doubt.”
Expert witness
When writing a report or giving expert evidence as a witness it must be remembered that the expert’s duty is to the court and not to any side or to the lawyers who commissioned the report. Common threads of enquiry include the causes of positive findings, the differential diagnosis, the forces required to produce the injuries sustained, the mechanisms of injury, the timing of injury, and the role of confounding issues such as seizures, cardiopulmonary resuscitation (CPR), apparent life-threatening events, and coughing, which frequently coexist in a child with traumatic brain injury. The report should take into account all material sent to the witness and should be well researched. A summary of publications addressing pertinent issues is often useful in providing a balanced view of the literature.20,21
The court will look for clarity in presentation and conclusions. The following issues are required by the court in any expert report:19
Evaluation of child maltreatment literature
Ophthalmology literature frequently lacks strict definitions of abuse. This introduces circular reasoning where the certainty of the findings being truly due to abusive injury cannot be confirmed. Evaluation of the literature should be supported by the use of a ranking system of various levels of certainty of abuse based on criminal or family court proceedings, perpetrator confessions, multidisciplinary team assessments, and defined clinical criteria. The various levels of certainty of child abuse may be defined as definite, probable, or possible, or ranked 1 to 5 where rank 1 represents the highest level of certainty and 5 the least22,23 (Table 67.1). This does not eliminate circularity, but makes it less likely if cases of “definite” or a high ranking (1 or 2) abuse represent the cases of the studies we need to rely on.
Table 67.1 Ranking of abusive injury
| Ranking | Criteria used to define abuse23 |
|---|---|
| 1 | Abuse confirmed at case conference or civil or criminal court proceedings or admitted by perpetrator or independently witnessed |
| 2 | Abuse confirmed by stated criteria including multidisciplinary assessment (social services/law enforcement/medical) |
| 3 | Abuse defined by stated criteria |
| 4 | Abuse stated but no supporting detail given |
| 5 | Suspected abuse |
Ophthalmic features of physical abuse
Direct injury
Early literature suggested that direct injury to the eye and orbit may manifest with periocular swelling and bruising (Fig. 67.3), burns, lid lacerations, hyphema, cataracts, retinal dialysis, and retinal detachments.24,25

Indirect injury
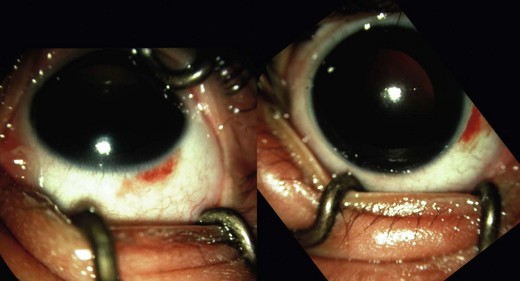
1. Subconjunctival hemorrhages. These may be present in AHT with or without intraocular injury.26 The presence of subconjunctival hemorrhages in cases of suspected child abuse should prompt a full child protection and ophthalmology assessment (Fig. 67.4).
2. Retinal hemorrhages. The presence of retinal hemorrhages is not necessary to establish the diagnosis of AHT though they are highly suggestive. There is no pathognomic type (flame shaped, dome shaped, dot, blot, white-centered), size, distribution, or location of retinal hemorrhages seen exclusively in abusive head injury27 (Fig. 67.5). Bilateral hemorrhages are reported in 74% of cases (sensitivity of 75% and specificity of 94%) of abusive head injury.28

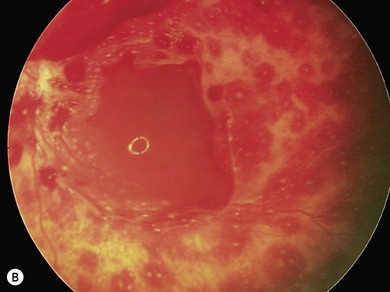
Retinal hemorrhages in the presence of head injury have a 71% positive predictive rate of abusive injury29 (Fig. 67.6). The prevalence of retinal hemorrhages in AHT varies between 77% and 83%.18 Preretinal hemorrhages, dome-shaped hemorrhages, situated in the posterior pole are seen commonly in AHT27 (Fig. 67.7). Retinal hemorrhages may range from a few scattered hemorrhages to widespread hemorrhages extending from the posterior pole to the periphery and situated in multiple layers of the retina30 (Fig. 67.8). Extensive retinal hemorrhages correlate with severe intracranial injury and poor visual outcome.31 A recent systematic review reported that in the presence of head injury retinal hemorrhages have a 91% probability of abusive etiology (odds ratio 14.7).32
3. Retinal folds. Perimacular folds, an important sign, are seen in 6% to 8% of live AHT cases (Fig. 67.9) and 23% of postmortem cases18,28,33 ( Fig. 67.10). There are also isolated case reports in Terson’s syndrome in adult patients34 and accidental head injury.35–38
4. Retinoschisis. Cystic intraretinal cavities (Fig. 67.11) in the macular area are recognized by vessels coursing over the surface or an electronegative electroretinogram. Schisis cavities are seen in 14% to 23% of case studies involving live and postmortem findings. It has been stated that traumatic hemorrhagic macular schisis in not seen in any other condition except AHT;39 however, recent case reports suggest similar cavities are seen with severe trauma or crush injury.37,38
5. Vitreous hemorrhage. Hemorrhage in the vitreous occurs in 14% of cases and is more frequent in autopsy specimens.18 It is believed to occur with break-through of the dome shaped preretinal hemorrhages into the vitreous cavity (Fig. 67.12
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


