Vernal Keratoconjunctivitis
E. Lee Stock
David M. Meisler
Vernal keratoconjunctivitis (VKC) is a chronic and debilitating external ocular disease. The name itself reflects two aspects of the disease. Vernal means youth and spring. In general, children are affected in a large percentage of the cases. The peak age of onset is 8 to 12 years, although 10% of VKC patients are older than 20 at age of onset.1 A large number of patients with VKC have symptoms that are exacerbated in the spring, possibly due to the increase in the pollen count. However, Duke-Elder2 suggests that most symptoms appear in the summer rather than in the spring. Most series describe a male preponderance, although one series points out a female preponderance of patients with limbal vernal when cases are stratified by sex.3
Clinical Findings
Conjunctiva
Patients with VKC may be divided into two groups based on clinical presentation: palpebral vernal and limbal vernal. Palpebral vernal involves the upper tarsal conjunctiva and is characterized by cobblestone papillae, i.e., papillae that are enlarged, often having flattened tops (Fig. 1). Papillae can be distinguished from follicles by their red centers; the center is a dilated blood vessel seen on end at the core of the papilla. A sequel that may occur in VKC is conjunctival scarring that has a lacy appearance at the base of the old papillae. Although rare, there may be lacy scarring that extends superiorly into the fornix (Fig. 2). On rare occasions there may be conjunctival cysts (Fig. 3) and enough scarring to cause symblepharon formation. Fibrin that is enhanced by heat may accumulate on the giant papillae and is known as the Maxwell-Lyons sign.4
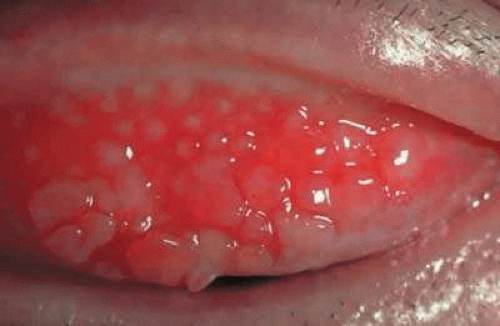 Fig. 1 Clinical photograph of the upper palpebral conjunctiva showing cobblestone papillae with their flat-top appearance. |
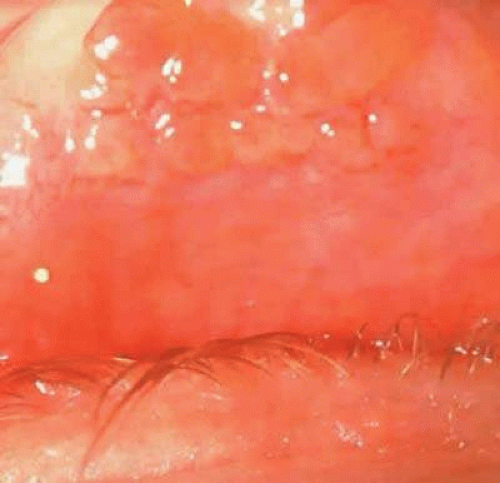 Fig. 2 Upper lid retracted with a Desmarres retractor showing the cobblestone papillae of the upper tarsal conjunctiva and lacy scarring of the upper fornix. |
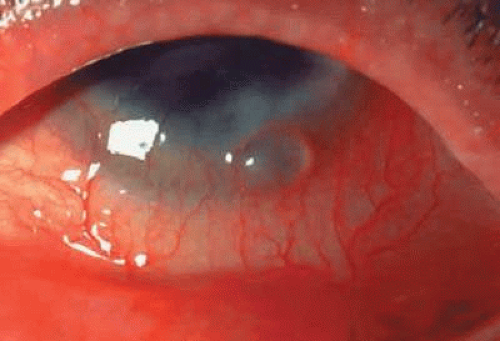 Fig. 3 Conjunctival cyst at the limbus. |
Limbal vernal begins as a thickening and opacification of the limbus. Limbal nodules appear as gelatinous, elevated lesions that may seem to coalesce and become confluent. Horner-Trantas dots are small white elevated lesions that appear at the apices of limbal excrescences that consist of desquamated epithelial cells and eosinophils (Fig. 4). Mixed vernal is a combination of limbal and palpebral lesions.
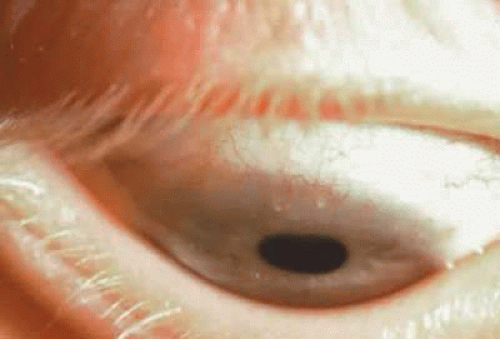 Fig. 4 Limbal vernal: Horner-Trantas dots and elevated gelatinous lesions. |
Cornea
Corneal involvement may be severe enough to interrupt a child’s social development and education. If uncontrolled, corneal inflammation may cause permanent scarring and loss of vision. VKC is characterized by a combination of punctate epithelial erosions and keratitis.5 Punctate epithelial erosions are tiny areas of absent epithelium that stain with fluorescein. Punctate epithelial keratitis is comprised of multifocal collections of inflammatory cells into the corneal epithelium. The epithelium in this area stains with rose bengal, which stains devitalized cells.6 Keratitis epithelialis of Tobgy7 is the early phase of vernal keratitis, consisting of punctate epithelial keratitis. When the keratitis coalesces, a vernal VKC ulcer is formed. Vernal corneal ulcers, also known as shield ulcers, are usually horizontally oval in orientation and involve the upper third of the cornea (Fig. 5). There is often white material deposited as a plaque at the base of the ulcer, which has been reported to be mucopolysaccharides. In general, these ulcers are sterile, but there have been reports of superimposed infections occurring in VKC corneal ulcers. Kerr and Stern8 described four patients with VKC who developed bacterial corneal ulcers. These patients showed infiltrates in the cornea, corneal edema, iritis, and hypopyon. Staphylococcus aureus grew out of the ulcer from all four, and three of the four ulcers were polymicrobial. These acute ulcers were differentiated from vernal shield ulcers, which are indolent in nature.
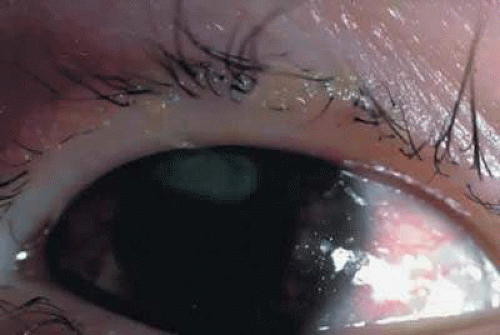 Fig. 5 Vernal ulcer that is horizontal in upper one third of cornea. |
Mucus
VKC is often accompanied by a thick, tenacious mucous discharge that may be so thick that it adheres to the giant cobblestones of the upper tarsus. When removed, it may form a cast of the cobblestones. Patients report symptomatic relief when the stringy, ropy secretions are removed from the cul-de-sac. In addition, the combination of punctate epithelial keratitis and increased mucus may predispose to the patient developing filamentary keratitis.
Associated Diseases
Butrus et al.28 described ten patients with the hyperimmunoglobulin E syndrome, which comprises chronic pruritic dermatitis, marked elevation in systemic IgE levels, severe recurrent systemic infections, and coarse facial features. Four of these patients had systemic atopic symptoms consistent with asthma or allergic rhinoconjunctivitis. Three of these four had ocular findings “similar to those of vernal conjunctivitis,” including papillary hypertrophy of the upper tarsal conjunctiva, corneal shield ulcer, and Trantas dots. There is also a strong association between ectatic corneal disease, such as keratoconus and pellucid marginal degeneration, and VKC.29
Pathophysiology
Type I Hypersensitivity
There is evidence that VKC is an allergic disease, appearing in patients who are atopic (i.e., having signs of asthma, eczema, or hay fever). The mechanism of disease involves fixation of IgE molecules on the surface of mast cells and release of mediators, including histamine and prostaglandins.9
Frankland and Easty10 noted that 93% of their 35 patients from the United Kingdom had manifestations of atopic disease, including asthma, eczema, or hay fever, but 7% did not. In another study, serum IgE levels were elevated in 75% of patients with VKC.11 These authors suggested two subgroups based on the presence or absence of IgE in the serum. In support of this concept, Zavaro et al.12 studied two patients in depth, one of whom had evidence of atopic disease, including elevated serum and tear IgE; the other had no evidence of atopic disease. Further support of the concept of two subclasses of VKC was given by Neumann et al.,1 who suggested that the prevalence of atopy in their VKC population in Israel was the same as in the general population (10%). However, Zavaro et al.12 stated that 80% of their Israeli patients had elevated IgE in the tears and marked eosinophilic infiltration of the conjunctiva.
Abu El-Asrar et al.13 investigated the immunopathology of VKC patients. They found numerous plasma cells that were producing IgA and IgG, but rarely IgE. However, they also found numerous mast cells with IgE on the surface. Allansmith14 reported IgE as well as IgA and IgD plasma cells in the tarsal conjunctiva of patients with VKC.
Allansmith and Frick15 noted antibodies to grass in the tears of patients with VKC. In addition increased IgE levels in the tears of patients with VKC have been reported, although these authors believed that the increased tear levels were a function of increased serum IgE levels. Subsequently, specific IgE antibodies to pollen allergens were identified in the tears,16 and there have been other reports of specific IgE antibodies in the tears.17 In addition, these investigators found higher levels of antibody in the tears than in the serum, suggesting local production of antibody in the conjunctiva.
Mediators
Mediators of immediate hypersensitivity reactions such as histamine have been found to be elevated in the tears of patients with VKC.21 Leukotrienes, potent chemoattractants for eosinophils and neutrophils, are produced by the mast cell after the initiation of degranulation. They are elevated in the tears of patients with VKC.22
Eosinophil granule major basic protein is the main protein found in the eosinophil granule. It causes desquamation of respiratory epithelium in vitro and mast cell degranulation and is deposited at sites of damage in vivo. It has been found in the tears of patients with VKC,23 as well as in the tissue24 and in corneal ulcers of these patients.25
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


