Clinical Testing for Normal and Abnormal Binocular Perception
Lawrence Tychsen
Marshall M. Parks
Clinical testing of binocular perception should examine both two-dimensional (2D) fusion (binocular correspondence) and three-dimensional (3D) fusion (binocular disparity sensitivity or stereopsis). We describe the common tests used in ophthalmology clinics to discern fusion, stereopsis, suppression, and diplopia.
WORTH 4-DOT OR POLAROID 4-DOT TEST
One of the simpler methods for investigating fusion, diplopia, and suppression is the “4-dot test.” For the Worth (colored) 4-dot test, the testing target consists of four illuminated dots that are clustered equidistant from each other: two dots are green, one is red, and one is white (Fig. 9.1). The patient views the target with a red filter in front of one eye and a green filter in front of the other (dichoptic viewing through anaglyphic glasses*). Viewed through the red filter, the green dots are invisible; viewed through the green filter, the red dot is invisible. The white dot is seen as red when viewed through the red filter and as green when viewed through the green filter. Thus, the test subject when viewing monocularly sees two red dots through the red filter and three green dots through the green filter. Binocularly, however, the fusing subject perceives the target as four dots because the white dot is seen as either a single red or green dot, according to which eye is dominant. If the dominance pattern vacillates between the eyes, the white dot manifests color rivalry by changing from red to green. The patient may alternatively report a dot of blended, yellowish hue.
The examiner must consider that the response of the patient may vary according to the size of the projection angle that the cluster of the four dots presents to the retinas. A patient with normal binocular vision perceives four dots, regardless of how minute the projection angle that the target subtends on the retina. A patient with a small-angle strabismus (or monofixation syndrome) and intact, but subnormal binocular vision may not fuse the target when the target subtends an angle of about 3° or less, but may fuse larger targets (e.g., 6°).
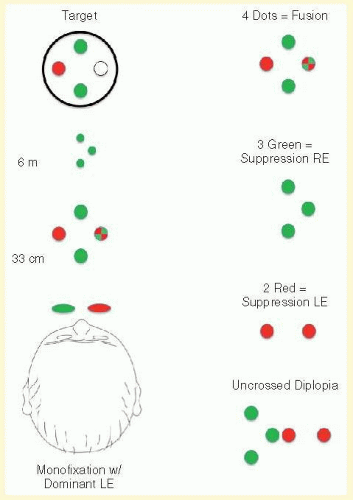 FIG. 9.1 Worth 4-dot test. The patient views four illuminated dots in the pattern of a diamond. The top and bottom dots are green, the left dot is red, and the right dot is white. When wearing red-green glasses, the red dot can be seen with the right (red filter) eye only, the green dots with the left (green filter) eye only, and the white dot with either eye (as an additional red or green dot) or both eyes (as a blended hue, typically yellowish). The patient is asked to count the dots and report their colors. |
Two methods are often used to perform the test. One is to have the target at a fixed distance from the subject (e.g., 6 m), which may either be contained in an illuminated box or be projected on a video screen. This is referred to as the distant Worth dot test. The other method is a near Worth dot test, which consists of a flashlight moved closer to or farther from the subject to alter the projection angle (size) of the target image on the retinas. The latter can be accomplished also with the fixed-distance Worth dot test by having the subject walk closer to or farther from the target. At 6 m, the distant Worth dots project an image of approximately 1.25°; at 0.33 m, the near Worth dots project an approximately 6° angle (Fig. 9.1). The projection angle of the image is the imaginary circumference encircling the outer border of the four dots collectively, not simply the projection angle of each of the four dots. The patient should be tested wearing any necessary refractive correction behind the red-green filters.
Monofixation syndrome patients characteristically have a foveal (suppression†) scotoma in the nonfixating eye (Fig. 9.1), which precludes a fusion response unless the projection size of the target image exceeds 3°. If the distant Worth dot test is 6 m from the patient, it is not fused. If the right eye is dominant, the patient reports two red dots. By advancing toward the target (enlarging the target angle), fusion is achieved. Similarly, the Worth flashlight test can begin with the target farther than 0.33 m (6° image) from the eye. As the flashlight target approaches 0.33 m, the response will convert from monocular (suppression of one eye) to binocular (fusion of the four dots).
Strabismic patients with deviations of 10Δ or more typically have a monocular response (two red if dominant right eye and three green if dominant left eye) or, alternatively, a diplopic response. The diplopic response to the Worth dot test is five lights (two red and three green). The dots seen by the fixating eye are clear, whereas those seen by the deviating eye are indistinct. The indistinct/blurred dots are projected in space opposite the direction of the deviated eye, causing uncrossed diplopia in esotropia (left eye dots to the left and right eye dots to the right) and crossed diplopia in exotropia (left eye dots to the right and right eye dots to the left). The dots seen by a hypertropic eye appear lower; those seen by a hypotropic eye appear higher. Horizontal or vertical diplopia can be eliminated by the appropriate prism(s) placed before the strabismic eyes. Some strabismic patients with angles 10Δ or more may report fusion of the dots at near. But this response is the exception rather than the rule. The monocular or diplopic responses are the rule.
One precaution must be exercised by the examiner so that alternating monocular fixation is not mistaken for diplopia. Rapid alternation between fixating eyes can produce a false response of five dots: summation of the three green dots seen by one eye and the two red dots seen by the other. The key question is whether the five lights are seen simultaneously, or true diplopia.
The 4-dot test is simple enough to be performed on children who can count to five. If visual acuity using symbols can be determined, so can the 4-dot response. The test should be performed with low room illumination, but not darkness, to provide other fusion clues.
The Polaroid 4-dot test resembles the Worth 4-dot test in all important respects. The difference is that the separating of dots to the right or left eye is achieved by polarizing filter spectacles and targets rather than colored filters.
BAGOLINI STRIATED LENS (GLASSES) TEST
Most tests for fusion, suppression, and diplopia entail unnatural (dichoptic) viewing conditions. Normal viewing is not through a combination of red-green filters. The striated glasses popularized by Bagolini, however, allow the patient to view naturally with only a faint reference line added to the scene viewed by each eye (Fig. 9.2). The reference lines for the two eyes are oriented at right angles. If using trial frame lenses, the examiner adjusts (rotates) the lenses so that the striations before the right eye and the left eye are perpendicular to each other. For example, the striations are placed at 135° in the trial frame in front of the right eye and at 45° in front of the left eye. The patient views a fixation light at any distance the examiner chooses; low background room illumination is maintained. The patient reports seeing the fixation light and observing streaks extending out into the peripheral field of vision.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


