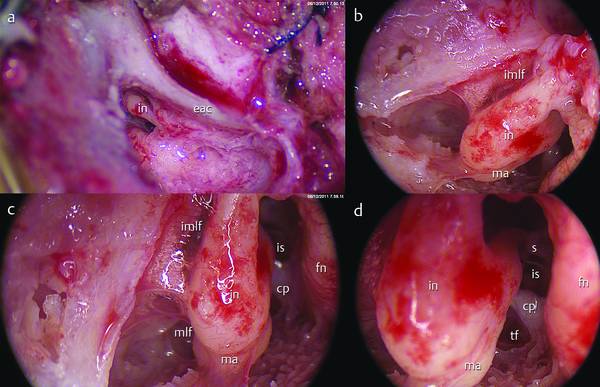
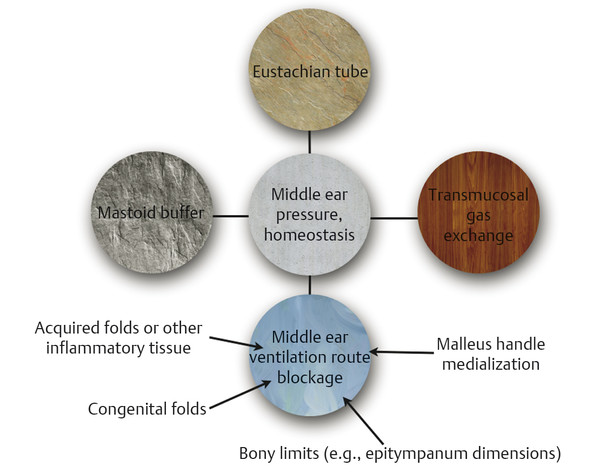
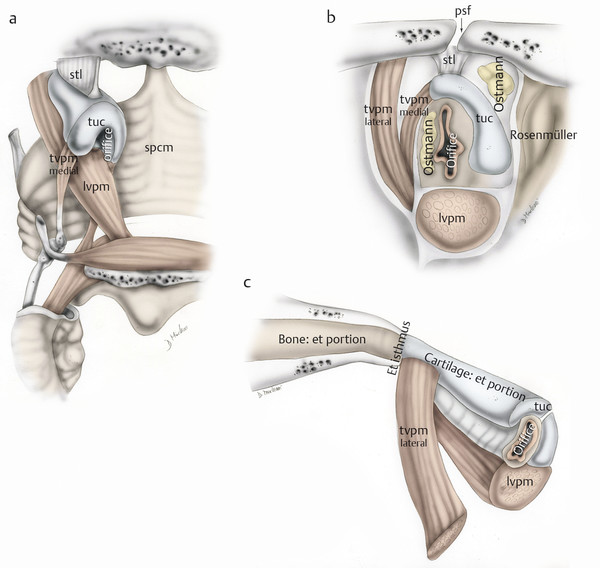
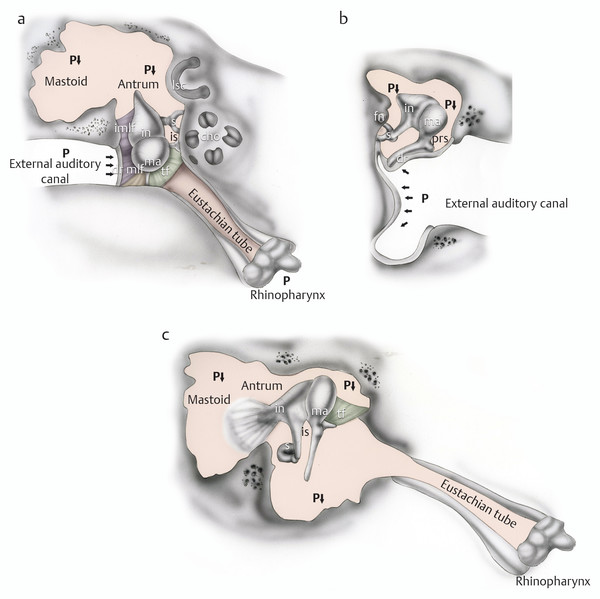
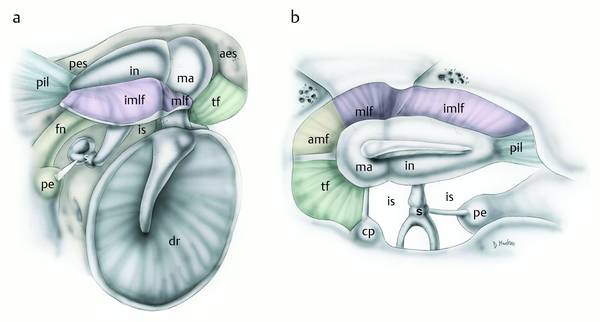
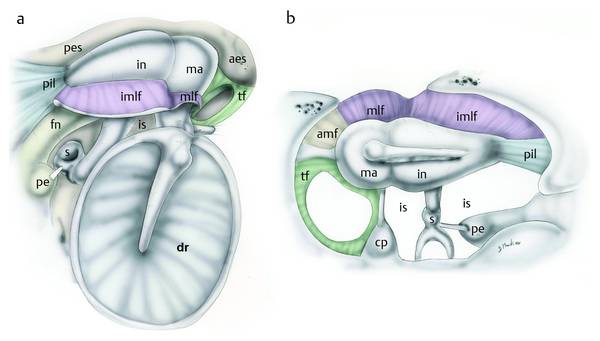
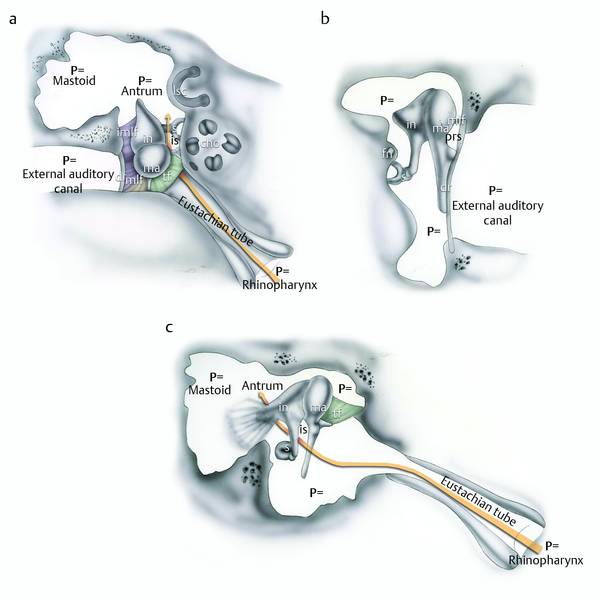
Barometric perturbation of the tympanic cavity can result in nonfunctional ventilation and consequently in creation of negative middle ear pressure. This is the basis for the generation of a retraction pocket at the level of the tympanic membrane (TM), mainly at the level of the pars flaccida, and if the process perpetuates, of primary acquired cholesteatoma formation. It is well known from the literature that there are some factors that can control the ventilation of the middle ear (ME); of these, the most important are: (a) eustachian tube (ET) function, (b) the pressure buffer mechanism produced by the middle ear and mastoid bone, and (c) transmucosal gas exchange in the tympanic cavity (▶ Fig. 5.1). In clinical practice it is not uncommon to find an isolated retraction pocket of the pars flaccida and/or a cholesteatoma limited to the posterior epitympanum, with an otherwise normal pars tensa and mesotympanum (▶ Fig. 5.2). In these cases it is hard to imagine that is the ET provoking the alterations, since it is not clear why only a part of the eardrum should be involved. Observations obtained during middle ear endoscopic procedures, and advances in anatomical knowledge of the middle ear, make it possible to postulate a further factor influencing middle ear gas homeostasis: the role of selective dysventilation, as described in detail later. Fig. 5.1 Factors playing a role in middle ear ventilation. Fig. 5.2 a–d Right ear. Isolated retraction pocket of the pars flaccida, endoscopic views (0° endoscope). It is well known that the normal physiological state of the ME is to have equal pressure between the tympanic cavity and the external side, and the ET function and its role as an ME pressure regulator have already been reported in several studies.1,2 When the ET fails to equalize pressure, a negative pressure occurs, leading to atelectasis of the TM and so to creation of a retraction pocket in the attic or posterosuperior quadrant and consequently to adhesive otitis media that can cause a cholesteatoma.3 Normally, the ET stays closed and opens when necessary to equalize pressure. Other functions include clearance of middle ear fluid while at the same time preventing nasopharyngeal secretions refluxing into the middle ear space. Both the ME and ET are lined by a mucociliary system as found in the respiratory system. A thin layer of mucus excreted by mucous cells lies on top of the cilia, which beat continuously and convey it and any debris as if on a conveyor belt from the ME through the ET into the nasopharynx.1 The ET opening is highly sensitive to the applied muscle forces and relatively insensitive to cartilage elastic properties. In an analysis of the muscle forces (tensor and levator veli palatini) and soft tissue elastic properties, luminal dilatation of the ET is caused by muscle contraction causing medial-superior rotation of the medial lamina, which in turn causes a deformation of fatty tissue surrounding the ET (Ostmann’s fat pad) (▶ Fig. 5.3).4 Fig. 5.3 Right ear. Anatomy of the eustachian tube. The cartilaginous portion and related muscles of the eustachian tube; posterior view (a). The eustachian tube orifice: a view tangential to the eustachian tube lumen at the level of the rhinopharynx (b). Bony and cartilaginous portions of the eustachian tube, coronal view (c). tvpm, tensor veli palatini muscle; lvpm, levator veli palatine muscle; tuc, cartilaginous component of the eustachian tube; psf, petrosphenoidal fissure; spcm, superior pharyngeal constrictor muscle; stl, suspensory tubal ligament. This sequence of pathogenesis of the progression to cholesteatoma could involve functional failure of the ET, leading to increased negative middle ear pressure, atelectasis of the tympanic membrane, formation of a retraction pocket in the attic or posterosuperior quadrant, and subsequent adhesive otitis media (▶ Fig. 5.4). Although otological surgery generally has been successful in clearing cholesteatomas, those patients with nonfunctioning or marginally functioning ET traditionally have been considered as having less successful results, and possible frequent recurrent pathology. Fig. 5.4 Right ear. Total retraction of the eardrum in a patient with failure of eustachian tube function: axial view at the epitympanic level (a), coronal view (b), sagittal view (c). In this case we observe a decrease of the pressure throughout the middle ear and mastoid, with subsequent retraction of the pars flaccida and pars tensa. in, incus; ma, malleus; s, stapes; is, isthmus; tf, tensor fold; fn, facial nerve; dr, eardrum; prs, Prussak space; imlf, lateral incudomalleal fold; mlf, lateral malleal fold; cho, cochlea; lsc, lateral semicircular canal. Another possible ET dysfunction is a continuous opening of the ET (patulous eustachian tube). Patients with this disorder complain about autophony or hearing their own breathing or echolike vocalizations. Causes can include hormonal changes (decreased estrogen levels), rapid weight loss, or chronic middle ear dysfunction. Although a causal relationship between tubal obstruction, development of negative middle ear pressure with subsequent effusion of fluid in the middle ear, and retraction of the tympanic membrane was postulated—the “hydrops ex vacuo” theory—this theory has been questioned for various reasons. First, anatomical tubal obstruction is rare. Second, the only demonstrated physiological way to create high negative middle ear pressure is active evacuation by sniffing, a mechanism that presupposes tubal closing failure. Third, the hydrops ex vacuo theory was based on the assumption that gas is continuously absorbed by the middle ear mucosa, but several recent studies have shown that transmucosal gas transport is bidirectional. Also, middle ear pressure can be maintained at ambient pressure or even be positive without tubal openings in healthy ears. These findings support the view that gas exchange over the mucosa is the basic mechanism for regulation of the middle ear pressure, whereas the eustachian tube serves as a release valve for excessive positive middle ear pressure and can also be opened by muscular forces to equalize excessive negative middle ear pressure. It is likely that the tubal capacity to open becomes more important in pathological conditions with impaired transmucosal gas exchange.2 The middle ear mucosa exchanges gas in a similar fashion to alveoli in the lung. The direction of gas exchange is predicated on the differences in partial pressure of the component gases in the middle ear cleft and mucosa (▶ Fig. 5.5). Inflammatory processes that affect the thickness and blood flow of the middle ear mucosa have a direct effect on the rate of diffusion.5 Fig. 5.5 The exchange of gas between the middle ear cleft and vascular space. Arrows represent direction of diffusion. From Danner CJ. Middle ear atelectasis: what causes it and how is it corrected?5 Several authors have studied the correlation between the gas exchange mechanism in the ME and the development of pathology in this area (otitis media with effusion and cholesteatoma),6,7 and Miura and colleagues8 published a paper in which the influence of gas exchange function through the middle ear mucosa was investigated in the development of sniff-induced ME diseases. They found that hypopneumatized mastoid (an indirect sign of a poor gas exchange function due to a low amount of mucosa in the ME) as well as ET dysfunction may be closely related to these pathologies due to a negative pressure level in the tympanum. In Miura’s study the authors examined mastoid pneumatization among patients with a sniffing habit using CT, and also examined the change of negative middle ear pressure induced by sniffing using tympanography. In ears with exudative otitis media or attic retraction, the areas of mastoid cavity were significantly smaller than those in eight normal ears of patients with a sniffing habit. These findings suggested that impairment of gas exchange function through the middle ear mucosa might be closely related to the development of sniff-induced middle ear disease.8 Changes in the middle ear pressure are due to gas exchange that occurs between the capillaries and the middle ear cavity via the middle ear mucosa. However, it is thought that the mucosal hemodynamics is altered in the case of inflammation of the middle ear mucosa, and that those changes influence the cross-mucosal gas exchange function.1,9 In a previous study in rabbits the middle ear tended to shrink when the mucosa was inflamed, probably due to disruption of the diffusion and absorption of CO2.10 Yaguci also demonstrated that mucosal gas exchange improved significantly after implantation of artificial mucosa,11 and this could be considered an indirect demonstration of the role of middle ear mucosa in gas homeostasis. Further studies based on comparison between gas exchanges in patients who had mastoidectomy and control patients showed that, in ears after surgery, recovery of both the gas exchange function and aeration in the mastoid is to be expected only when the mastoid mucosa can be preserved even partially.12 The relationship between volume and pressure is best represented by Boyle’s law, which states that at a constant temperature, pressure multiplied by volume equals a constant (P × V = C). Thus, pressure and volume are inversely proportional. Applied to the mastoid bone, this means that small mastoid volumes tend to cause greater changes in pressure.5 Therefore, the volume of mastoid aeration plays a significant role in middle ear compliance and the resultant forces impressed on the tympanic membrane. Cinamon and Sadé13 studied how the aerated spaces of the ME and mastoid as well as the mobility of the TM can diminish physiological pressure changes that occur regularly in the ME. The mastoid air volume “dilutes” pressure changes in relation to its size: the volume change required to alter a given pressure in an average mastoid (6 mL) is six times that which is needed in a small mastoid (1 mL). In the rigid TM model, the volume changes correlated linearly with the induced pressures and were confirmed to fit Boyle’s law. Altogether, a large “mastoid” required a greater volume change than a small one to induce the same pressure. Thus Cinamon and Sadé found that it is the ME with a small mastoid that is most vulnerable to pressure changes and that may develop compensatory buffering mechanisms, such as additional TM retraction (atelectasis) or ME volume reduction by fluid accumulation. Recently a further study also confirmed the role of the mastoid in middle ear pressure regulation; the results showed that the inert gas time constant decreases with increasing ME volume.13 In 1946, Chatellier and Lemoine formulated the concept of the “epitympanic diaphragm.” The detailed anatomical description has already been given in Chapter 4 (▶ Fig. 5.6, ▶ Fig. 5.7). As described, all epitympanic compartments receive their aeration via the large tympanic isthmus between the medial part of the posterior incudal ligament and the tensor tendon (▶ Fig. 5.8, ▶ Fig. 5.9, ▶ Fig. 5.10, ▶ Fig. 5.11). Some authors have suggested that obstruction of the tympanic isthmus is common in various types of middle ear disease and causes significant disturbance to air diffusion within the temporal bone pneumatic system, leading to complete or incomplete separation of the tubotympanic cavity from atticomastoid airspace (▶ Fig. 5.12). Since 1978, some authors have demonstrated the presence of a morphofunctional partition that separates the middle ear into an anteroinferior and a posterosuperior compartment.14 The anteroinferior compartment corresponds to the middle ear cleft (mesotympanum, protympanum, retrotympanum, and protympanum) and could be compared to the nose, while the posterosuperior compartment corresponds to the epitympanum, antrum, and mastoid cells and could be compared to the lung (▶ Fig. 5.13). These two divisions are separated by the epitympanic diaphragm. There are also some histological differences between these two compartments. The epithelial layer in the anteroinferior compartment is mainly pseudostratified and ciliated; there are also mucous cells; and the connective tissue is relatively thick and dense. The function of this compartment is mainly mucociliary clearance. In the posterosuperior compartment the epithelial layer is monocellular and contains flat cells; there are no ciliated or mucous cells; the connective tissue is loose and thin; and the function of this compartment is gas exchange.14 The authors also noted that the factors that caused obstruction of the tympanic isthmus were mucosal fold variations, inflammatory webs and exudate, retracted tympanic membrane, diseased attic mucosa, and cholesteatoma.15 In some more recent work we have found that obstruction of the tympanic isthmus and blockage of middle ear ventilation routes are frequent findings in patients affected by attic pathology (▶ Fig. 5.14, ▶ Fig. 5.15, ▶ Fig. 5.16).16,18 Fig. 5.6 a, b Right ear. Drawings representing the “epitympanic diaphragm” in a patient with a complete tensor fold. s, stapes; fn, facial nerve; cp, cochleariform process; ma, malleus; in, incus; aes, anterior epitympanic compartment; amf, anterior malleolar fold; pes, posterior epitympanic compartment; pil, posterior incudal ligaments; tf, tensor fold; mlf, lateral malleal fold; imlf, lateral incudomalleal fold; is, isthmus; pe, pyramidal eminence. Fig. 5.7 a, b Right ear. Drawings representing the “epitympanic diaphragm” in a patient with an incomplete tensor fold. s, stapes; fn, facial nerve; cp, cochleariform process; ma, malleus; in, incus; aes, anterior epitympanic compartment; amf, anterior malleolar fold; pes, posterior epitympanic compartment; pil, posterior incudal ligaments; tf, tensor fold; mlf, lateral malleal fold; imlf, lateral incudomalleal fold; is, isthmus; pe, pyramidal eminence. Fig. 5.8 Right ear. Middle ear aeration pathway in a patient with normal function of the eustachian tube: axial view at the epitympanic level (a), coronal view (b), sagittal view (c). in, incus; ma, malleus; s, stapes; is, isthmus; tf, tensor fold; fn, facial nerve; dr, eardrum; prs, Prussak space; imlf, lateral incudomalleal fold; mlf, lateral malleal fold; cho, cochlea; lsc, lateral semicircular canal.

5.2 Eustachian Tube
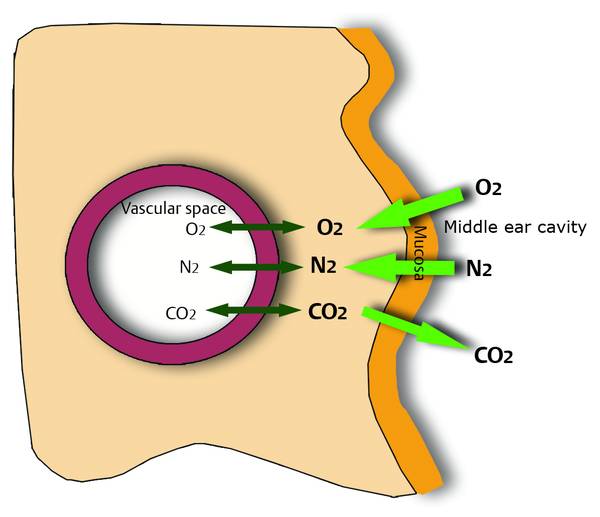
5.3 Transmucosal Gas Exchange
5.4 Mastoid Buffer
5.5 Blockage of Middle Ear Ventilation Routes
Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine