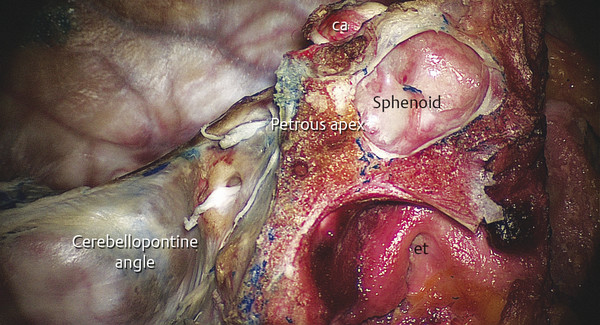
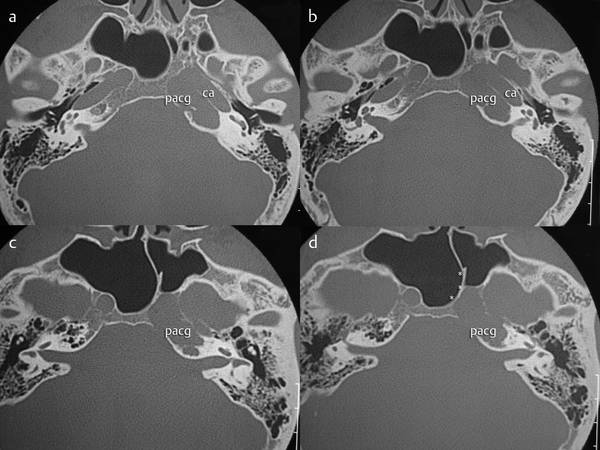
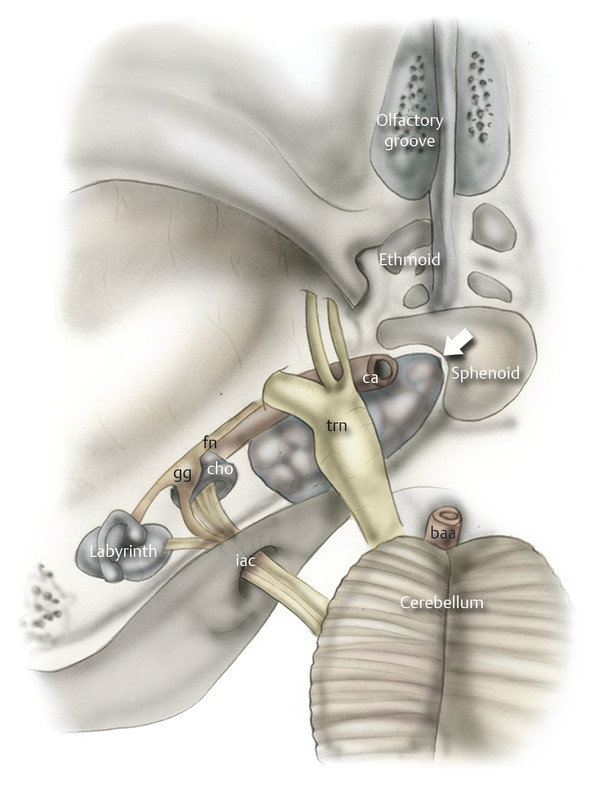
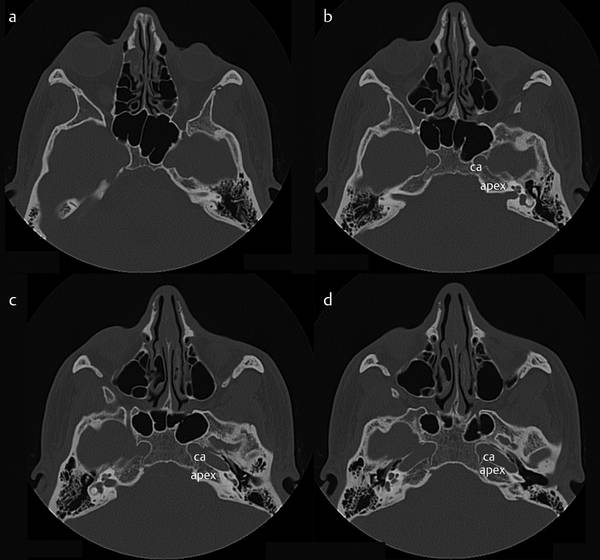
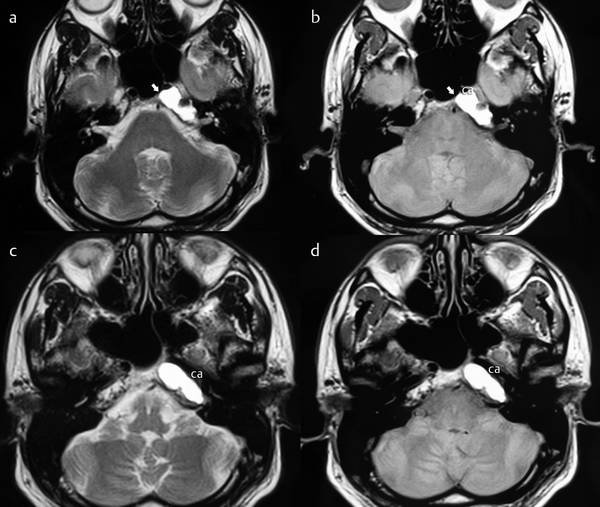
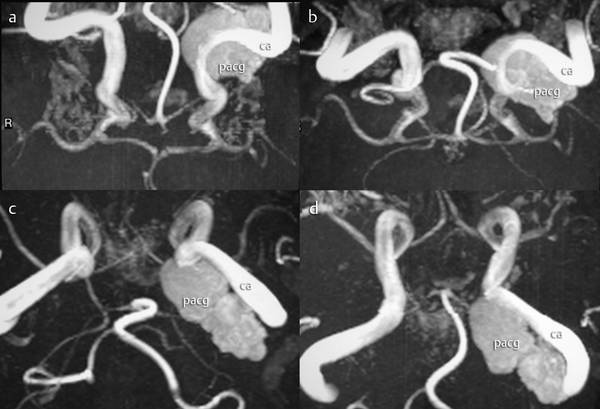
Endoscopic Endonasal Approach to the Petrous Apex Lesions of the petrous apex encompass a wide and varied range of pathologies and numerous skull base and neurosurgical procedures have been described for their removal. Problems with morbidity have in part been responsible for the trend toward the use of minimally invasive surgical approaches. Endoscopically assisted transphenoidal techniques for the petrous apex have been reported sporadically in the literature. This chapter assesses the feasibility of approaching the petrous apex endonasally using detailed anatomical and surgical landmarks. The petrous apex is a pyramid-shaped structure that is the most medial aspect of the temporal bone (▶ Fig. 20.1).1 Fig. 20.1 A global view of the petrous apex and its relationship with the surrounding structures. (Sagittal view on a cadaveric head.) et, eustachian tube; ca, carotid artery. The base of the pyramid is the otic capsule, the hemicanal of the tensor tympani, and the petrous carotid artery. The superior surface extends from the arcuate eminence to the precavernous carotid artery and the Meckel cave. The posterior surface faces the cerebellopontine angle; it begins laterally at the common crus/vestibular aqueduct and ends medially at the Dorello canal and petroclinoid ligament. The jugular fossa and inferior petrosal sinus are located at the inferior aspect of the petrous apex. The internal carotid artery (ICA) enters the petrous apex along the inferior surface via the carotid canal. The IAC begins at the porus acousticus on the posterior face of the petrous apex and ends at the fundus. The cochlear aqueduct enters the petrous apex along its inferior surface just medial to the jugular fossa. The petrous apex is primarily composed of bone marrow or dense bone with only 9% to 30% of patients showing some pneumatization. Pneumatization of the petrous apex is variable and often differs between sides in the same patient. Lesions of the petrous apex can be divided into two main groups:2,3 Inflammatory/cystic Cholesterol granuloma (more than 90%) Epidermoid or cholesteatoma (4% to 9%) Effusion or “trapped fluid” (1%) Mucocele (less than 1%) Arachnoid cyst (less than 1%) Petrous apicitis or abscess (less than 1%) Petrous carotid aneurysm (less than 1%) Chordoma of the clivus Neoplasms Chondrosarcoma (less than 1%) Meningioma (less than 1%) Metastasis (less than 1%). Careful preoperative evaluation is critical in minimizing intraoperative and postoperative complications.2–7,9–15 Thorough neurological examination allows the identification and understanding of preoperative deficits. Preoperative imaging studies To define the exact size of the lesion and particularly to define the exact location of the lesion relative to the sphenoid sinus (▶ Fig. 20.2, ▶ Fig. 20.3); to detect the most accessible nasal fossa for the surgical procedure; and to detect the relationship to the carotid artery or any possible displacement of the internal carotid artery that could complicate or contraindicate the procedure.2,11,15 When there is no expansion of the lesion into the sphenoidal sinus, the window between the brainstem and the vertical segment of the internal carotid artery may be very narrow. A narrow window between the brainstem and internal carotid artery has been considered a relative contraindication for an endoscopic approach (▶ Fig. 20.4). Fig. 20.2 a–d Temporal bone, preoperative CT study. Axial view. Petrous apex cholesterol granuloma (pacg) lying at the medial edge of the internal carotid artery (ca). In this case the relationship between the petrous apex cholesterol granuloma and the posterolateral wall of the sphenoid is close, allowing the transsphenoid drainage of the lesion. *, intrasinus septum. Fig. 20.3 Drawing (in axial view) representing the relationship between the petrous apex and the cerebellopontine angle posteriorly in an individual with a petrous apex lesion expanding into the sphenoidal sinus. Cho, cochlea; fn, facial nerve; trn, trigeminal nerve; iac, internal auditory canal; ca, carotid artery. Fig. 20.4 Temporal bone CT study. Axial view. a–d In this patient the petrous apex is not in direct contact with the posterior wall of the sphenoid. This anatomical condition is a contraindication for the transnasal endoscopic approach to the petrous apex. ca, carotid artery. To distinguish cholesterol granulomas from other lesions of the petrous apex such as vascular lesions, neoplastic lesions, petrous apicitis, cholesteatoma, and mucocele.3,5,78,9 CT (▶ Table 20.1) is often the initial study used to evaluate the lesions and identify possible bone erosions; contrast enhancement is helpful in the diagnosis, and administration of contrast medium is recommended if there are no contraindications (▶ Fig. 20.2). MRI (▶ Table 20.2) provides valuable information for accurately diagnosing these lesions (▶ Fig. 20.5, ▶ Fig. 20.6). Fig. 20.5 a–d Axial T2 MRI showing a markedly hyperintense lesion in the left petrous apex protruding into the left sphenoid sinus (arrow) lying medially to the carotid artery (ca). Fig. 20.6 a–d Angio-MRI showing the relationship between the petrous apex lesion and the internal carotid artery. pacg, petrous apex cholesterol granuloma; ca, carotid artery. Drainage of a cholesterol granuloma involving the petrous apex Drainage of petrous apicitis or abscess Biopsy of a solid lesion of the petrous apex Resection of a soft lesion such as a chondrosarcoma. Anatomical conditions—a small diploetic sphenoid sinus and primarily petrous lesions that have a narrow connection with the sphenoid sinus Carotid artery in the drainage pathway (mobilization of the petrous carotid artery is possible).
20.1 Introduction
20.2 Anatomy
20.3 Lesions of the Petrous Apex
20.4 Preoperative Selection of Patients
Lesion
Bone erosion
Eroded margin
Contralateral apex
Contrast enhancement
Cholesterol granuloma
+
Smooth
Highly pneumatized
−
Cholesteatoma
+
Smooth
Often not pneumatized
−
Petrous apicitis
+
Irregular
Variable
−
Effusion
−
−
Usually pneumatized
−
Bone marrow asymmetry
−
−
Variable
−
Carotid aneurysm
+
Smooth
Variable
+
Neoplasia
+
Variable
Variable
+
Lesion
T1 images
T2 images
T1-gadolinium
Cholesteatoma
Hypointense
Hyperintense
No enhancement
Cholesterol granuloma
Hyperintense
Markedly Hyperintense
No enhancement
Petrous apicitis
Hypointense
Hyperintense
Rim enhancement
Effusion
Hypointense
Hyperintense
Mucosal enhancement
Bone marrow asymmetry
Hyperintense
Hypointense
No enhancement
Neoplasia
Hypointense
Hyperintense
Enhancing
Carotid aneurysm
Hypointense
Mixed
Rim enhancement
20.5 Indications for an Endoscopic Endonasal Approach
20.6 Contraindications for an Endoscopic Endonasal Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


