Introduction
Although cholesteatoma represents the most frequent lesion in the middle ear cavity, it is not the only disease occurring in this region. There is a variety of benign neoplasms that can also be discovered within the middle ear cleft.
Tympanic paragangliomas represent the most frequent primary neoplasms of the middle ear.1 Adenomatous tumors are another class of benign neoplasms that can potentially develop in the middle ear cavity. These tumors can be benign (adenomas) or malignant (adenocarcinomas).2 Some adenomas characterized by a neuroendocrine component have been categorized by certain authors as carcinoid tumors, reflecting their histological similarity to intestinal carcinoid.3 They are now classified as middle ear adenomas with neuroendocrine differentiation (MEA-ND).
Osteomas can also sometimes develop in the tympanic cleft, although they represent a very rare finding.
As with cholesteatomas, in the majority of reported cases a retroauricular-transcanal approach is described for small benign tumors limited to the promontory, while a canal wall up mastoidectomy or canal wall down mastoidectomy is chosen to treat larger tumors extending into the hypotympanum, the eustachian tube, and/or the tympanic sinus.
17.2 Tumor Characteristics
17.2.1 Glomus Tympanicum
Glomus tumors, also known as paragangliomas, are neoplasms of neuroectodermal origin that originate in the paraganglia, a collection of small neuroendocrine organs. Temporal bone paragangliomas are classified into four categories (types A, B, C and D) according to their location and extension on the basis of high-resolution computed tomography (HRCT) examination (▶ Fig. 17.1).4 Paraganglioma tympanicum (also known as “glomus tympanicum”) represents the most frequent primary neoplasm of the middle ear1 The term “glomus tympanicum” is reserved for temporal paragangliomas limited to the middle ear and mastoid without involvement of the jugular bulb. They originate from the glomus bodies that lie along the Jacobson nerve (tympanic branch of the ninth cranial nerve), and the Arnold nerve (auricular branch of the tenth cranial nerve).1 Glomus tympanicum can also expand into the mastoid, can occlude the eustachian tube, or can protrude through the tympanic membrane into the external auditory canal.1
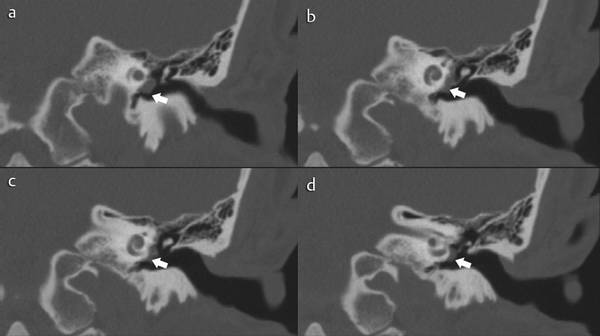
Fig. 17.1 a–d CT scan, coronal view, showing a type A glomus tympanicum (white arrow).
In contrast, the term “glomus jugulare” is reserved for those cases originating from the paraganglia located in the adventitia of the dome of the jugular bulb or those cases originating in the hypotympanum with secondary invasion of the jugular bulb.1
Pulsatile tinnitus, conductive hearing loss, and vertigo are the most common presenting complaints.1
17.2.2 Middle Ear Adenomatous Tumors
Another class of neoplasms that can potentially develop in the middle ear cavity is represented by middle ear adenomatous tumors (MEAT). These lesions can be benign (adenomas) or malignant (adenocarcinomas).2 Adenomas characterized by a neuroendocrine component have been categorized by certain authors as carcinoid tumors due to their histological similarity to intestinal carcinoid.3 They are now classified as middle ear adenomas with neuroendocrine differentiation (MEA-ND). The main clinical manifestation of MEAT is progressive conductive hearing loss.5 Vertigo, presence of a palpable mass, disturbance of equilibrium, nerve paralysis, pain, bleeding, infection, otorrhea, and otalgia can be present. Tinnitus is uncommon in MEAT.6
Middle ear adenomas, MEA-ND, and glomus tympanicum are not distinguishable on the basis of their CT and MRI presentations. All these tumors progressively enlarge and fill the tympanic cavity and the mastoid antrum.2 Ossicular involvement and destruction may occur and can be well depicted on CT scans (▶ Fig. 17.2, ▶ Fig. 17.3).2 Nevertheless, the presence of massive bone destruction should evoke differential diagnoses such as adenocarcinomas, metastatic tumors, or cholesteatomas.2
On MRI, both MEAT and glomus tympanicum appear as soft tissue tumors of intermediate T1 signal isointense to white matter, and slightly increased T2 signal compared with gray matter.7 Significant enhancement is observed after injection of contrast medium (iodine- or gadolinium-containing) in both tumors, without specific characteristics.8,9
Conservative but total resection is the recommended treatment for MEA-ND.3 Since recurrence is common if the tumor is peeled off the ossicles, their removal is recommended.3 Metastasis is extremely rare and its very occurrence is in fact controversial.10
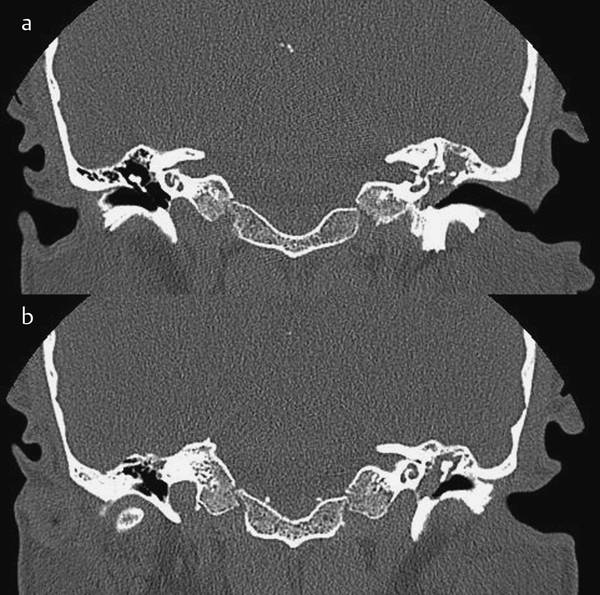
Fig. 17.2 a, b CT scans, coronal view (carcinoid tumor of the middle ear). CT shows a soft tissue mass involving the whole tympanic cavity on the left side.
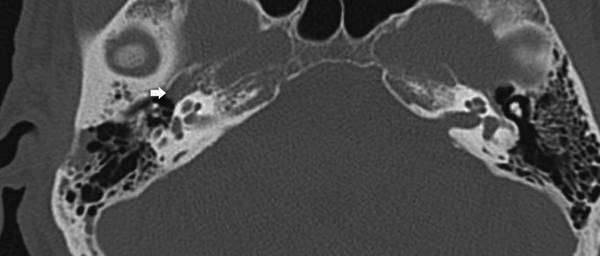
Fig. 17.3 CT scan, axial view (carcinoid tumor of the middle ear). CT shows a soft tissue mass lying anteriorly in the protympanic space involving the eustachian tube opening (white arrow).
17.2.3 Middle Ear Osteoma
Osteoma represents a benign neoplasm that can be detected inside the middle ear. Osteomas are benign slow-growing tumors histologically characterized by dense lamellae with organized haversian canals. Within the temporal bone they are most commonly seen in the external auditory canal but may also arise from other sites such the mastoid, the eustachian tube, the petrous apex, the internal auditory canal, and the styloid process, with corresponding symptoms (▶ Fig. 17.4, ▶ Fig. 17.5).11 Although osteomas of the middle ear can remain asymptomatic, conductive hearing loss is the most common symptom. In addition, when the eustachian tube is obstructed, otitis media with effusion may appear.12
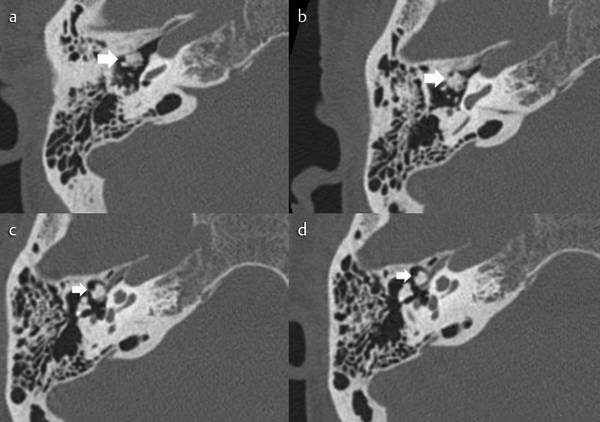
Fig. 17.4 a–d CT scan, axial view, showing a bony tissue mass in the tympanic cavity involving the anterior epitympanic space and the protympanum (white arrow) suspected as middle ear osteoma.
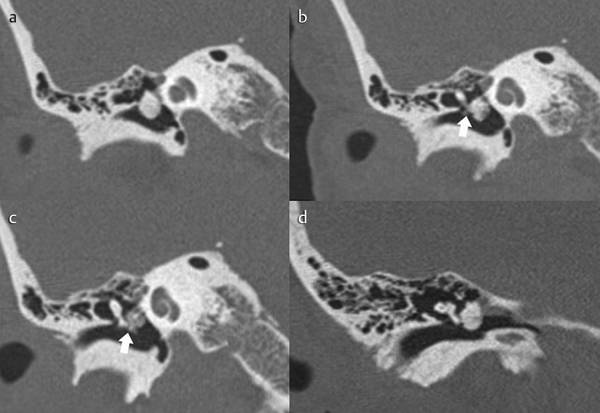
Fig. 17.5 a–c CT scans, coronal view, showing a bony tissue mass into the tympanic cavity involving the malleus (white arrow). d Sagittal view of the ear: osteoma on the handle of the malleus.
This lesion appears as a well-circumscribed mass with soft tissue density, eggshell-like density, or bone density in CT scan.13
Surgical intervention is only recommended for symptomatic lesions, such as osteomas with ossicular chain involvement, otic capsule erosion, eustachian tube obstruction, and round window obstruction.13
These different benign tumors can be circumscribed exclusively in the middle ear cleft or can expand to the adjacent regions. Different surgical approaches must be planned depending on the extension of the lesion. For a very limited mass occupying the middle ear, it might be easy for the surgeon to observe and control the lesion using only a microscopic transcanal approach. Unfortunately, these masses often involve some “hidden regions” of the middle ear such as the protympanic and the retrotympanic areas. Epitympanic and/or hypotympanic involvement are also possible. In these situations a microscopic transcanal approach becomes almost impossible and a retroauricular-transcanal approach or even a canal wall up/wall down mastoidectomy becomes necessary in order to achieve the best exposure of the hidden areas.
The use of an endoscopic approach makes it possible to maintain an exclusively transcanalar access for lesions involving the hidden areas of the tympanic cleft as well. This technique allows more conservative surgery to be realized than does the microscopic approach.
17.3 Treatment
The surgical approaches to benign neoplasms of the middle ear depend on the involvement of particular regions within the cavity (▶ Fig. 17.6).
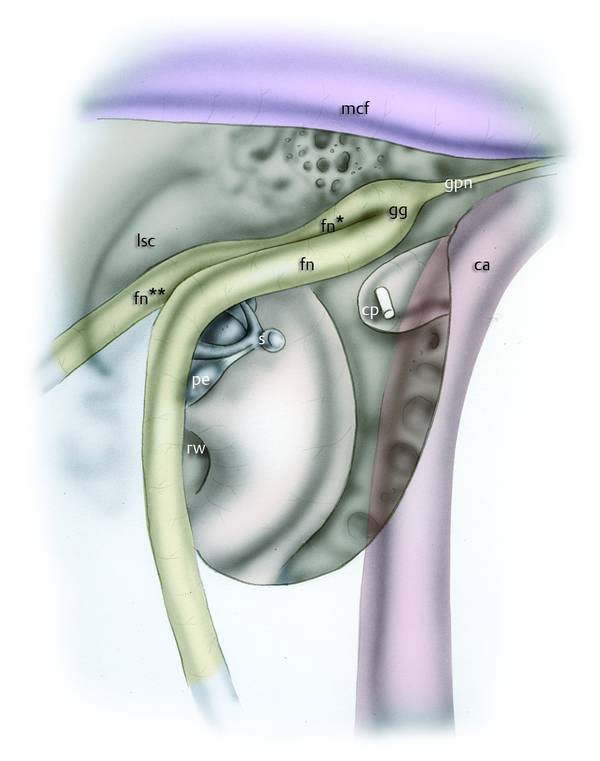
Fig. 17.6 Right ear. Surgical anatomy of the most important anatomical structures lying in the medial wall of the tympanic cavity. s, stapes; rw, round window; fn, facial nerve; ca, carotid artery; mcf, middle cranial fossa; gg, geniculate ganglion; fn*, labyrinthine facial nerve; cp, cochleariform process; gpn, greater petrosal nerve; lsc, lateral semicircular canal; pe, pyramidal eminence.
All these tumors can be circumscribed in the central part of the middle ear cleft or can extend to the adjacent regions. Different surgical approaches must be planned on the basis of their extension. In cases of a very limited mass, it might be easy for the surgeon to observe and control the lesion using only a microscopic transcanal approach. Unfortunately, these masses can often involve some “hidden regions” of the middle ear. In particular the protympanic and the retrotympanic areas represent sites that can hardly be observed with transcanal microscopic vision, but epitympanic and/or hypotympanic involvement can also represent a difficult challenge. In these situations, with exclusively microscopic management, it becomes almost impossible to obtain a clear visualization of the neoplasm without performing a retroauricular-transcanal approach or even a canal wall up/wall down mastoidectomy. From our experience, with the use of the endoscopic technique, hidden regions such as the protympanum, hypotympanum, and retrotympanum can be more easily visualized, without the necessity of retroauricular incisions, mastoidectomies, or extended approaches.
17.3.1 Indications
Benign tumors limited to the tympanic cavity, without extension to the mastoid. The main contraindication is represented by tumors involving the mastoid region. A relative contraindication can be the presence of a narrow external auditory canal.
17.3.2 Surgical Technique
A circular incision is made in the external auditory canal about 3 cm from the fibrous anulus with a circular scalpel or Vesalius (▶ Fig. 17.7). A lateral-medial skin dissection is performed, interposing cottonoids soaked in epinephrine between the skin flap and the underlying bone of the external auditory canal; pushing the cottonoids forward with the dissector, the skin is detached from the bone until the fibrous anulus is exposed (▶ Fig. 17.8, see Clinical case 1 [▶ Fig. 17.9

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


