Endoscopic Middle Ear Anatomy
4.1 Introduction
The middle ear is recognized to be a very small space, almost inaccessible by microscope in some regions. The complexity of middle ear anatomy has prompted experienced otosurgeons to develop different techniques for exploring areas that are difficult to visualize with the operating microscope. Despite the illumination and magnification offered by the operating microscope, it has proved to have distinct limitations. The surgeon can visualize structures only directly ahead and is unable to see around objects. This straight-line view offered by the microscope produces blind spots during middle ear surgery. These limitations can be overcome with the complementary help of an endoscope, which allows “looking around corners.”
The development of endoscopic techniques in recent times has given rise to a new application of this tool: endoscopic surgery of the middle ear. During the 1990s endoscopy was used in otology only as a diagnostic tool and never over the eardrum. Recent developments of endoscopy in middle ear surgery have permitted an unprecedented extremely detailed view of the “in vivo” anatomy of the middle ear. Exploration of hidden recesses such as the sinus tympani, the anterior epitympanic space, and the protympanic space with such magnification is almost impossible with traditional microscopic approaches. From our 6-year experience in endoscopic ear surgery, we believe that most of these inaccessible spaces could easily be visualized by endoscope-assisted surgery, and that new or revised anatomical concepts need to be introduced for this.
Other than a wider and clearer view of middle ear anatomy, endoscopy allows better understanding of middle ear physiology and ventilation pathways that might cause pathology if impaired.
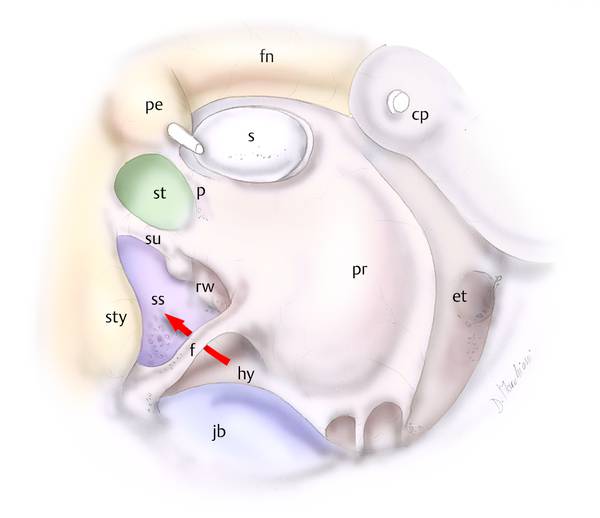
The middle ear can be conceptually divided into subspaces on the basis of their relationships with the mesotympanum: the mesotympanum is the portion that an observer can visualize through the external ear canal by the use of an otoscope or a microscope. Posteriorly to it lies the retrotympanum, superiorly the epitympanum, anteriorly the protympanum, and inferiorly the hypotympanum (▶ Fig. 4.1). The detailed endoscopic anatomy of each of these will be illustrated and discussed.
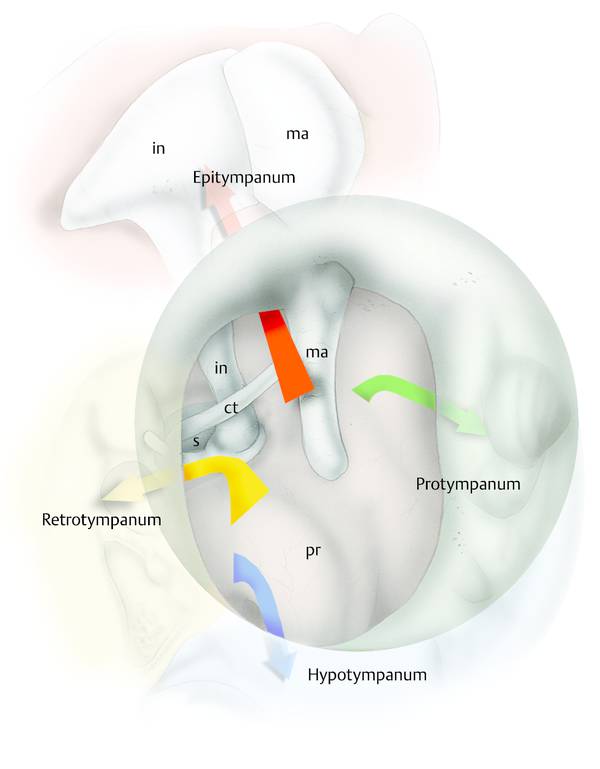
Fig. 4.1 Right ear. Drawing showing the hidden recess of the middle ear. ct, chorda; ma, malleus; in, incus; s, stapes; pr, promontory.
4.2 Retrotympanum
The retrotympanum is a complex structure consisting of different spaces lying in the posterior aspect of the tympanic cavity (▶ Fig. 4.2).1 The retrotympanum is divided into the superior retrotympanum and the inferior retrotympanum (▶ Fig. 4.3) by a bony crest termed the subiculum, described in detail below.
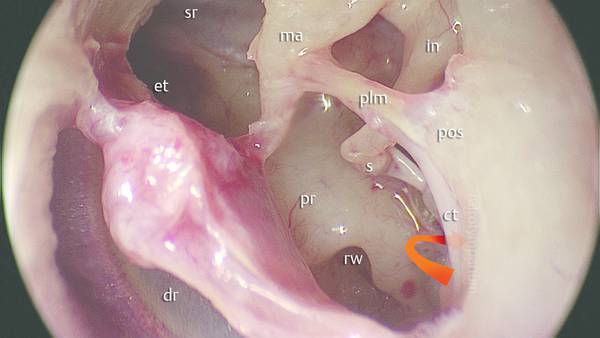
Fig. 4.2 Left ear. The position of the retrotympanic complex with respect to the tympanic cavity (the red arrow shows where the retrotympanum is located). ma, malleus; pr, promontory; s, stapes; rw, round window; et, eustachian tube; ct, chorda; in, incus; plm, posterior ligament of the malleus; pos, posterior spine; dr, eardrum; sr, supratubal recess.
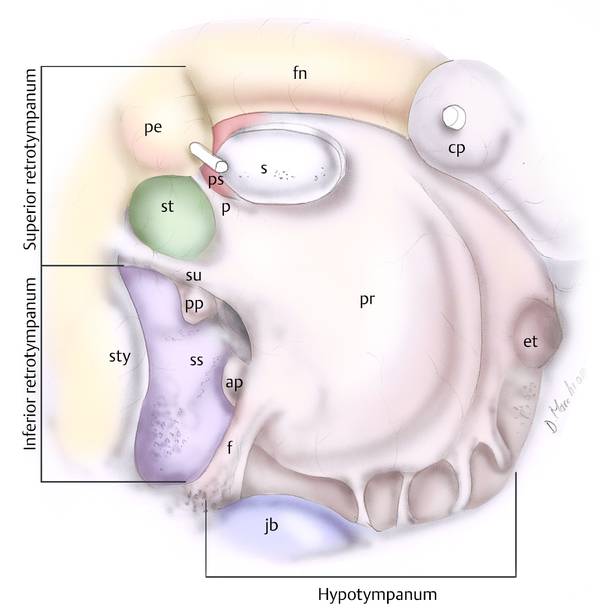
Fig. 4.3 Right ear. The subdivisions of the medial compartments of the retrotympanum. Two different portions can be distinguished: an inferior retrotympanal space composed of the sinus subtympanicus lying between the finiculus inferiorly and the subiculum superiorly; and a superior retrotympanal space composed of the sinus tympani between the subiculum inferiorly and the ponticulus superiorly, with the posterior sinus separated from the sinus tympani by the ponticulus. pr, promontory; s, stapes; et, eustachian tube; f, finiculus; ap, anterior pillar; pp, posterior pillar; jb, jugular bulb; ss, sinus subtympanicus; sty, styloid complex; su, subiculum; p, ponticulus; st, sinus tympani; ps, posterior sinus; pe, pyramidal eminence; fn, facial nerve; cp, cochleariform process.
We can identify four spaces in the superior retrotympanum: two spaces lying medial and anterior, and two spaces lying lateral and posterior to the third portion of the facial nerve and the pyramidal eminence (▶ Fig. 4.4). The pyramidal eminence is the fulcrum of the retrotympanum. From this structure arise two bony structures: the chordal ridge extending outward and transversally toward the chordal eminence, and separating the facial recess superiorly and the lateral tympanic sinus inferiorly; and the ponticulus extending inward and transversally to the promontory region dividing the sinus tympani inferiorly and the posterior tympanic sinus superiorly.
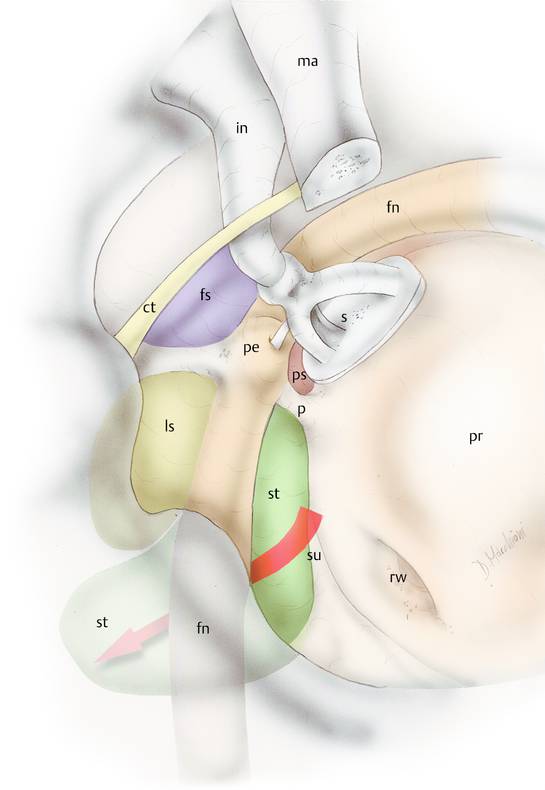
Fig. 4.4 Right ear. Drawing representing the medial and lateral spaces of the retrotympanum. pr, promontory; s, stapes; su, subiculum; p, ponticulus; st, sinus tympani; ps, posterior sinus; pe, pyramidal eminence; fn, facial nerve; fs, facial sinus; ls, lateral tympanic sinus; rw, round window; in, incus; ma, malleus; ct, chorda.
4.2.1 Sinus Tympani
The sinus tympani lies medial to the pyramidal eminence, the stapedius muscle, and the facial nerve and lies lateral to the posterior semicircular canal and vestibule. The superior limit of this space is represented by the ponticulus; the inferior anatomical limit is represented by a prominent ridge extending from the styloid eminence to the posterior rim of the cochlear window niche: the subiculum (▶ Fig. 4.5, ▶ Fig. 4.6, ▶ Fig. 4.7). The sinus has great variability in size and shape. Meckel2 described the sinus tympani for the first time but he only mentioned the portion anterior to the pyramidal eminence. Steinbrugge3 later studied the depth of the sinus tympani and was the first to describe the posterior extension of the sinus tympani: he probably found a deep sinus tympani with a posterior extension medial to the pyramidal eminence and facial nerve. Observing the variation in depth of the sinus tympani, he pointed out the importance of the disease in this kind of sinus tympani. Donaldson et al4 in the 1970s also studied the morphology and variations of the sinus tympani. He described a deep sinus tympani lying medial and posterior to the vertical portion of the facial nerve canal; he observed that when the sinus tympani is large it cannot be adequately cleaned with any known instruments using the microscope.
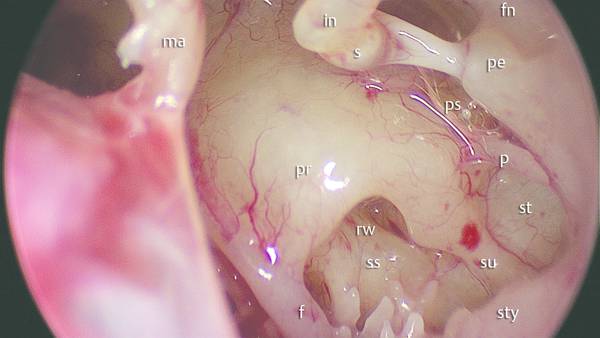
Fig. 4.5 Left ear. Transcanal endoscopic view of the medial spaces of the retrotympanum by 0° endoscope. The subiculum is a ridge of bone arising from the styloid complex to the posterior pillar of the round window niche dividing the sinus tympani from the sinus subtympanicus. pr, promontory; s, stapes; f, finiculus; jb, jugular bulb; ss, sinus subtympanicus; sty, styloid complex; su, subiculum; p, ponticulus; st, sinus tympani; ps, posterior sinus; pe, pyramidal eminence; fn, facial nerve; rw, round window; in, incus; ma, malleus.
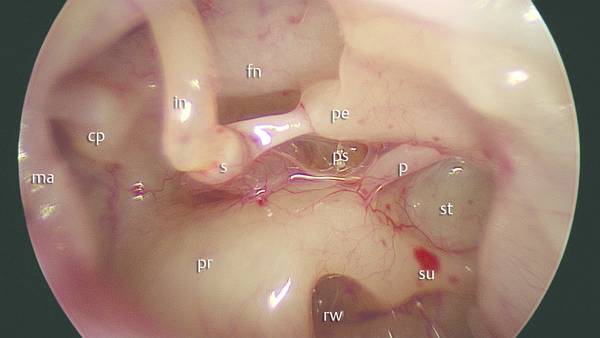
Fig. 4.6 Left ear. Transcanal endoscopic view of the retrotympanum and pyramidal eminence with a 0° endoscope. The ponticulus is a ridge of bone arising from the pyramidal eminence to the promontory region dividing the sinus tympani from the posterior sinus. pr, promontory; s, stapes; su, subiculum; p, ponticulus; st, sinus tympani; ps, posterior sinus; pe, pyramidal eminence; fn, facial nerve; rw, round window; in, incus; ma, malleus; cp, cochleariform process.
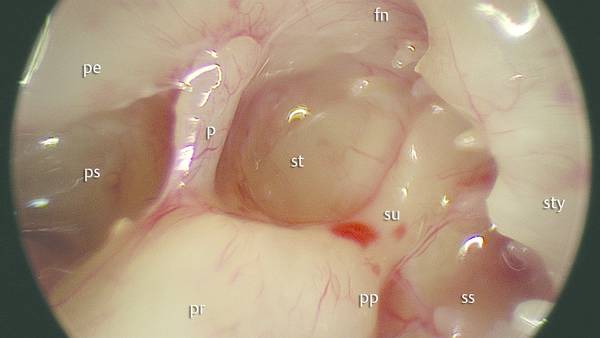
Fig. 4.7 Left ear. Endoscopic magnification of the medial boundary of the sinus tympani with a 45° endoscope. Classical shape: the sinus is located between the ponticulus and subiculum lying medial to the facial nerve and to the pyramidal process. pr, promontory; su, subiculum; p, ponticulus; st, sinus tympani; ps, posterior sinus; pe, pyramidal eminence; fn, facial nerve; ss, sinus subtympanicus; sty, styloid complex; pp, posterior pillar.
More recently the endoscopic anatomy of the sinus tympani and the feasibility of the endoscopic approach to the sinus tympani were studied by the present authors.1 The morphology of the sinus tympani was classified on the basis of intraoperative findings and the anatomical variations of the ponticulus were also observed.
Endoscopic study of the retrotympanum is facilitated by particular positioning of the surgeon. During an endoscopic approach to the retrotympanum the surgeon stands on the opposite side of the middle ear observed: by introducing the endoscope into the external ear canal with a 45° angle from the opposite side, a wide view of the medial boundary of the sinus tympani and of the ponticulus area is obtained.
The sinus tympani is classified into different types on the basis of shape.
Classical shape: the sinus is located between the ponticulus and subiculum lying medial to the facial nerve and to the pyramidal process (▶ Fig. 4.8).
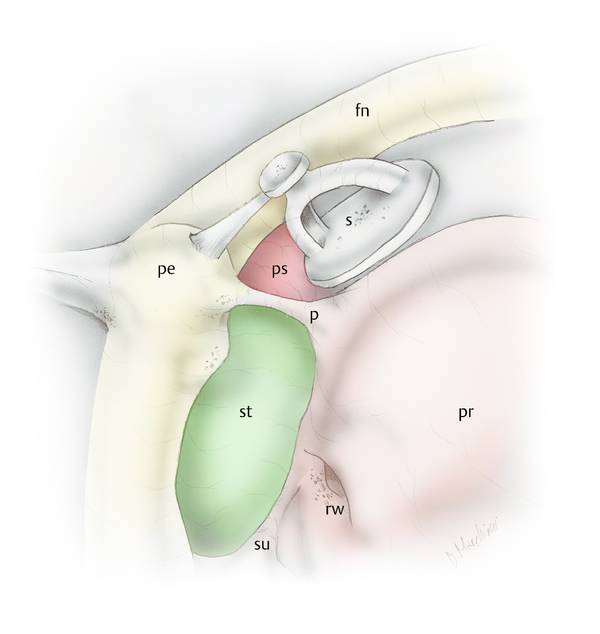
Fig. 4.8 Right ear. Sinus tympani with classical shape. pr, promontory; su, subiculum; p, ponticulus; st, sinus tympani; ps, posterior sinus; pe, pyramidal eminence; fn, facial nerve; rw, round window; s, stapes.
Confluent shape: an incomplete ponticulus is present and the sinus tympani is confluent to the posterior sinus (▶ Fig. 4.9).
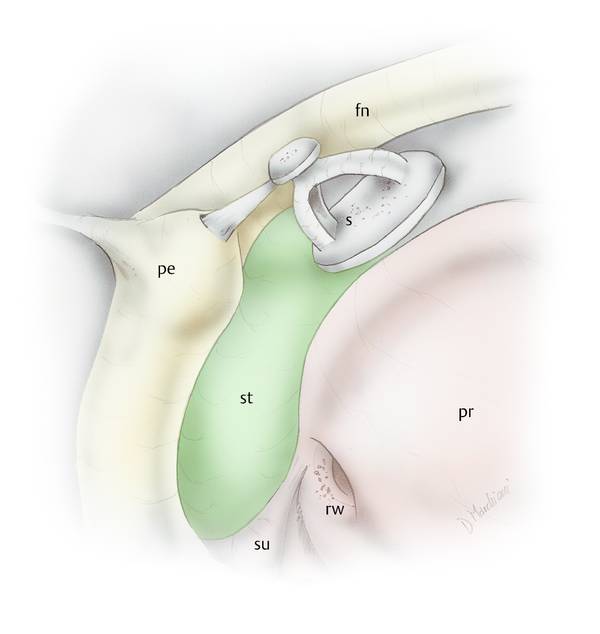
Fig. 4.9 Right ear. Sinus tympani with confluent shape. pr, promontory; su, subiculum; st, sinus tympani; pe, pyramidal eminence; fn, facial nerve; rw, round window; s, stapes.
Partitioned shape: a ridge of bone extending from the third portion of the facial nerve to the promontory area is present, separating the sinus tympani into two portions (superior and inferior) (▶ Fig. 4.10).
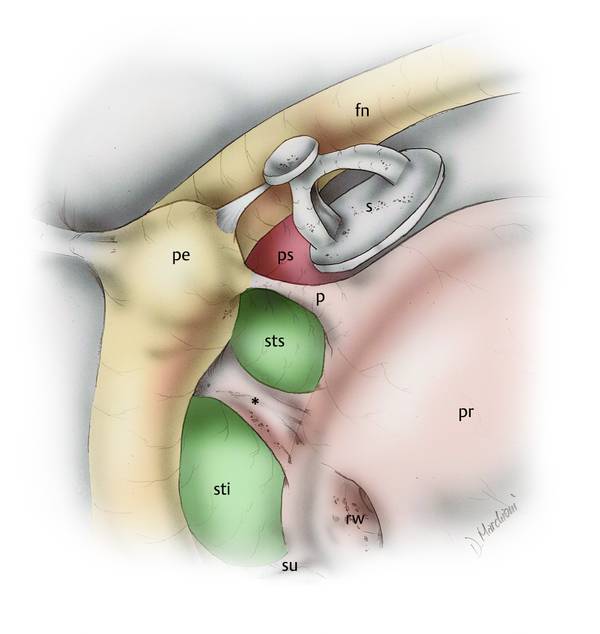
Fig. 4.10 Right ear. Sinus tympani with partitioned shape. pr, promontory; su, subiculum; sti, inferior portion of sinus tympani; sts, superior portion of sinus tympani; *, ridge of bone dividing the sinus tympani; pe, pyramidal eminence; fn, facial nerve; rw, round window; s, stapes; ps, posterior sinus; p, ponticulus.
Restricted shape: a high jugular bulb is present, reducing the inferior extension of the sinus tympani (▶ Fig. 4.11).
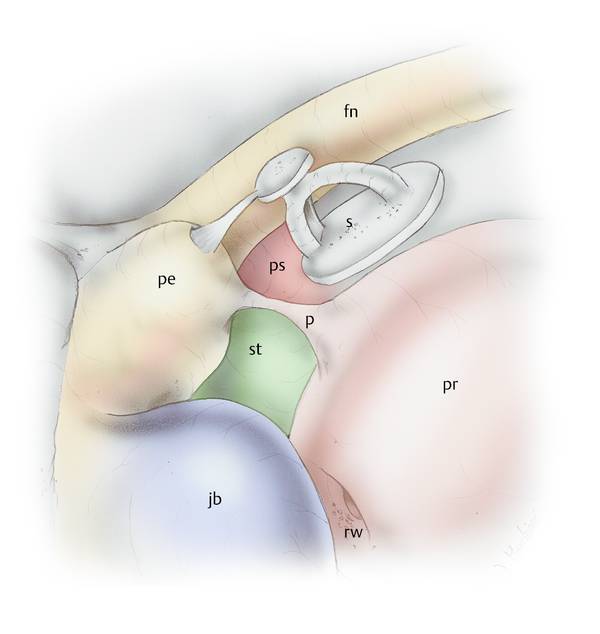
Fig. 4.11 Right ear. Sinus tympani with restricted shape. pr, promontory; st, sinus tympani; pe, pyramidal eminence; fn, facial nerve; rw, round window; s, stapes; ps, posterior sinus; jb, jugular bulb; p, ponticulus.
Several anatomical studies have focused on the depth of the sinus tympani. This is a very important detail because the deeper the sinus tympani the more difficult it is to achieve radical removal of cholesteatoma. This is especially true when the sinus tympani is very deep. For this reason it will be useful for the surgeon to study the extension of the sinus tympani before surgery. We have classified the depth of the sinus tympani into three types as follows (▶ Fig. 4.12).
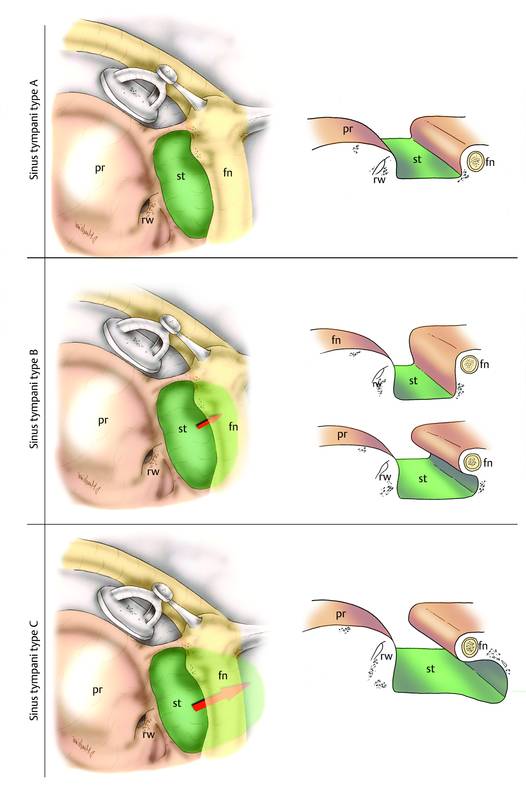
Fig. 4.12 Right ear. The depth classification of the sinus tympani. fn, facial nerve; rw, round window; pr, promontory; st, sinus tympani.
Type A: small sinus tympani. The medial limit of the third portion of the facial nerve corresponds to the depth of the sinus. In these cases, the sinus tympani is small and does not exhibit medial and posterior extension to the facial nerve.
Type B: deep sinus tympani. The medial boundary of the sinus tympani lies medially with respect to the third portion of the facial nerve and does not exhibit posterior extension to the facial nerve.
Type C: deep sinus tympani with posterior extension. The medial boundary of the sinus tympani lies medial and posterior to the third portion of the facial nerve. In these cases, the sinus tympani is very large and deep and all these patients have a well-developed mastoid.
In our experience, the transcanal endoscopic approach is indicated in patients with sinus tympani types A and B. When the patient has a type C sinus tympani it is not possible to explore the entire depth of the sinus, even with the endoscope, especially when it is associated with a well-developed mastoid cells. In these cases it is necessary to take a posterior retrofacial approach.
4.2.2 Ponticulus
The endoscopic approach to the sinus tympani permits a good view of the ponticulus as well.1,5 As described above, the ponticulus is a bony ridge extending from the pyramidal process to the promontory region, which separates the sinus tympani from the posterior tympanic sinus. Three different variants of the ponticulus can be distinguished.
Classical morphology (▶ Fig. 4.13): In these patients the ponticulus is completely formed and is like a ridge of bone extending from the pyramidal process to the promontory area; this structure represents the superior limit of the sinus tympani, dividing it from the posterior sinus.
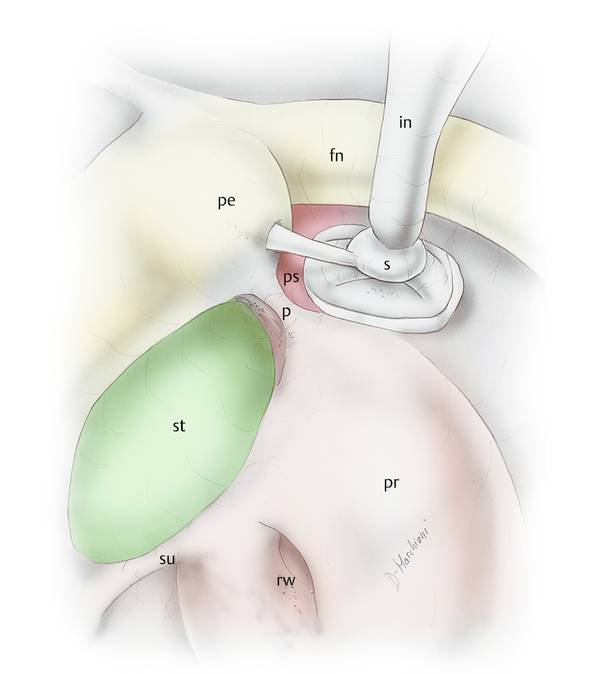
Fig. 4.13 Right ear. Ponticulus with classical morphology dividing the sinus tympani from posterior sinus. pr, promontory; su, subiculum; p, ponticulus; st, sinus tympani; ps, posterior sinus; pe, pyramidal eminence; fn, facial nerve; rw, round window; s, stapes; in, incus.
Incomplete ponticulus (▶ Fig. 4.14): In these cases, the sinus tympani and posterior sinus are confluent.
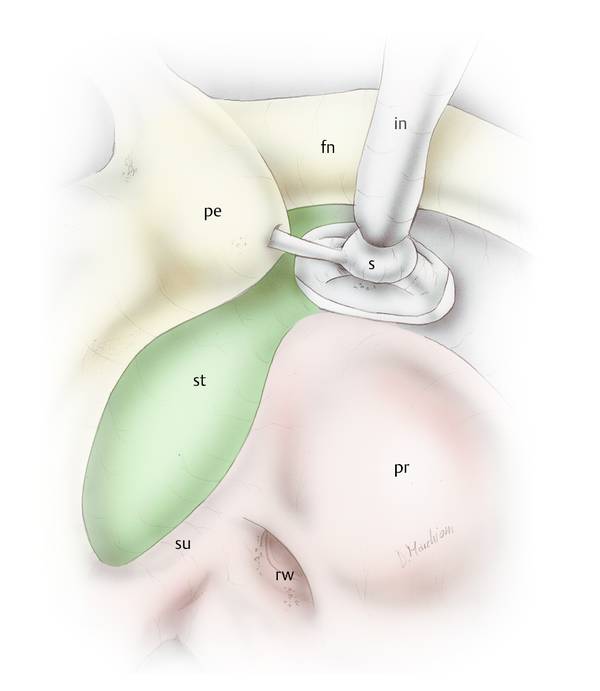
Fig. 4.14 Right ear. Ponticulus with incomplete morphology, in this case the sinus tympani is confluent with the posterior sinus. pr, promontory; su, subiculum; st, sinus tympani; pe, pyramidal eminence; fn, facial nerve; rw, round window; s, stapes; in, incus.
Communicating ponticulus: In these patients, the ponticulus is like a small bridge of bone and there is a communication between the sinus tympani and the posterior sinus below it (▶ Fig. 4.15, ▶ Fig. 4.16).
When the ponticulus resembles a small bridge, intraoperative endoscopic evaluation of the area is especially useful because a residual cholesteatoma could be present under the bony bridge.
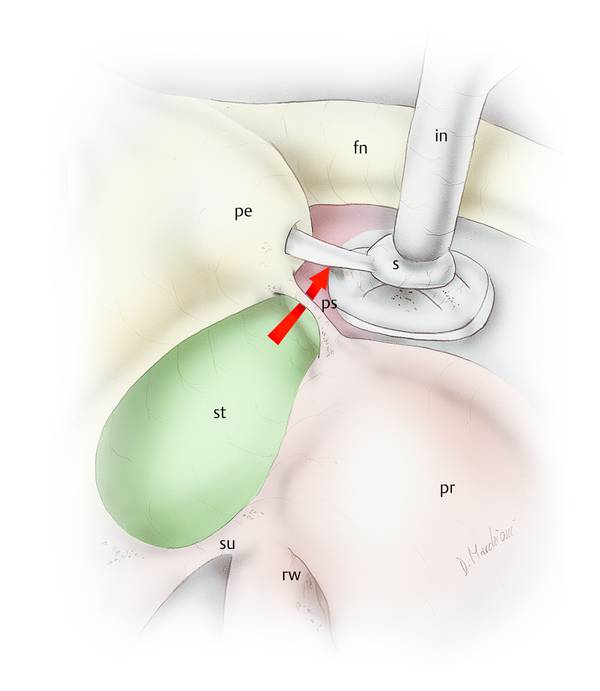
Fig. 4.15 Right ear. Ponticulus with bridge morphology; in this case the sinus tympani communicates with the posterior sinus under the ponticulus. The red arrow shows the communicating space between the sinus tympani and the posterior sinus. pr, promontory; su, subiculum; st, sinus tympani; ps, posterior sinus; p, ponticulus; pe, pyramidal eminence; fn, facial nerve; rw, round window; s, stapes; in, incus; ps, posterior sinus.
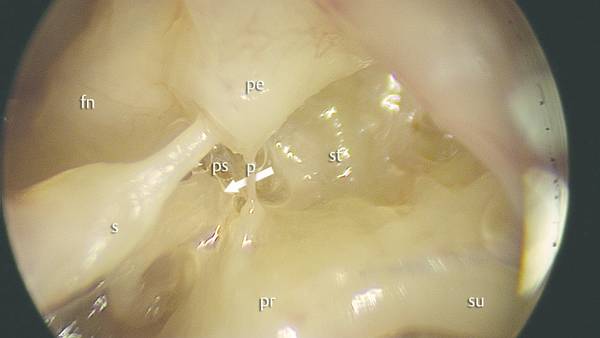
Fig. 4.16 Left ear. Ponticulus with bridge morphology, endoscopic view with 45° endoscope. White arrow shows the communicating space between the sinus tympani and the posterior sinus. pr, promontory; su, subiculum; st, sinus tympani; ps, posterior sinus; pe, pyramidal eminence; p, ponticulus; fn, facial nerve; s, stapes.
4.2.3 Subiculum
The endoscopic approach to the sinus tympani permits a good view of the subiculum also.5 The subiculum is a bony ridge extending from the posterior lip of the round window niche outward to the styloid eminence region, which separates the sinus tympani from the sinus subtympanicus, as explained in more detail below.
The subiculum may be present—in which case the sinus tympani is separated by the inferior retrotympanum (▶ Fig. 4.17)—or may be absent, and in this case the sinus tympani is confluent with the inferior retrotympanum (▶ Fig. 4.18). The bridge subiculum is a rare conformation; when present, under this bridge of bone there is a communication between the inferior retrotympanum and the sinus tympani (▶ Fig. 4.19).
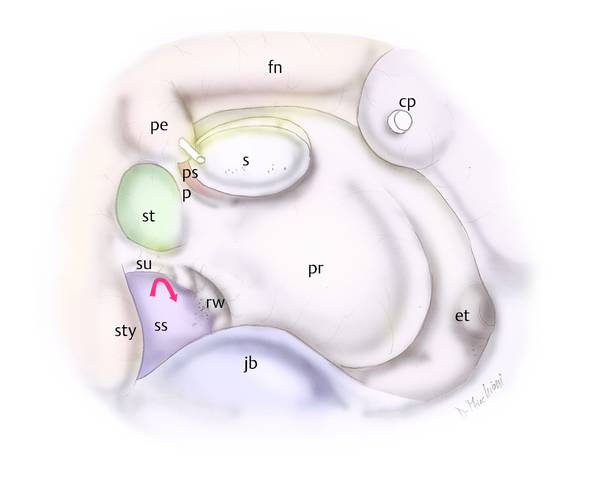
Fig. 4.17 Right ear. The subiculum is a ridge of bone arising from the styloid complex to the posterior pillar to the round window niche, dividing the sinus tympani from inferior retrotympanum. pr, promontory; s, stapes; et, eustachian tube; jb, jugular bulb; ss, sinus subtympanicus (inferior retrotympanum); sty, styloid complex; su, subiculum; p, ponticulus; st, sinus tympani; ps, posterior sinus; pe, pyramidal eminence; fn, facial nerve; cp, cochleariform process; rw, round window.
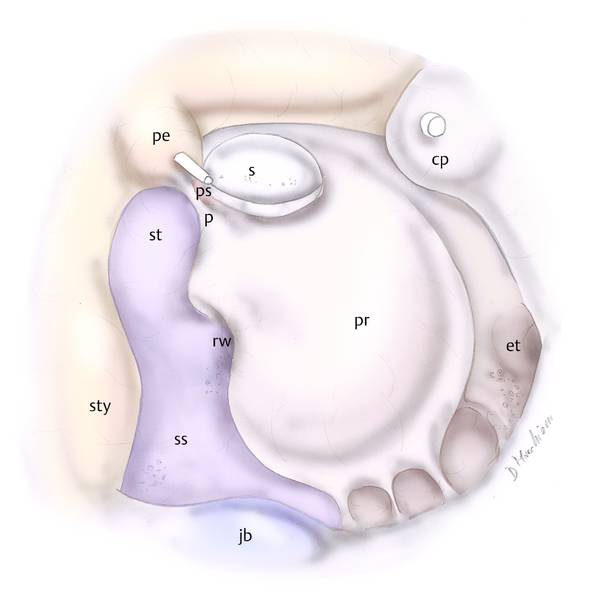
Fig. 4.18 Right ear. In this case the sinus tympani is confluent with the inferior retrotympanum (sinus subtympanicus) and the subiculum is absent. pr, promontory; s, stapes; et, eustachian tube; jb, jugular bulb; ss, sinus subtympanicus (inferior retrotympanum); sty, styloid complex; p, ponticulus; st, sinus tympani; ps, posterior sinus; pe, pyramidal eminence; cp, cochleariform process; rw, round window.
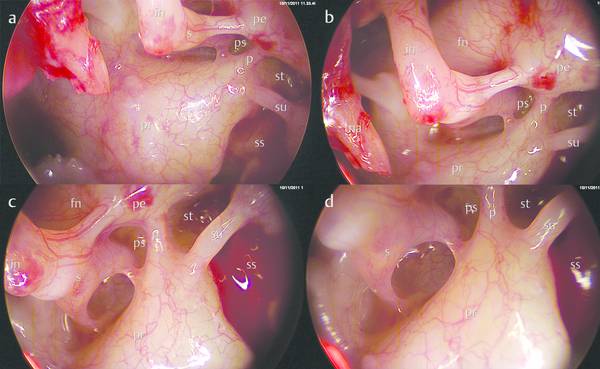
Fig. 4.19 a–d Left ear. Endoscopic views of the retrotympanum in patients with bridge subiculum (0° endoscope). pr, promontory; s, stapes; ss, sinus subtympanicus (inferior retrotympanum); p, ponticulus; st, sinus tympani; ps, posterior sinus; pe, pyramidal eminence; fn, facial nerve; in, incus; ma, malleus; su, subiculum.
4.2.4 Pyramidal Eminence and Subpyramidal Space
In our experience of performing endoscopic middle ear surgery, close and variable relationships have been noted between the sinus tympani (ST), the posterior tympanic sinus (PTS), and the pyramidal eminence (PE). Pneumatization of the retrotympanum may extend variably into a recess under the pyramidal eminence. We denoted this anatomical finding as the “subpyramidal space” (▶ Fig. 4.20).6 This space is limited laterally by the medial aspect of the pyramidal process, medially by the lateral wall of the tympanum, inferiorly by the ponticulus, and posteriorly and superiorly by the fallopian canal, and it may be in direct anatomical continuity with the sinus tympani or with the posterior tympanic sinus, depending on the position of the ponticulus (▶ Fig. 4.21, ▶ Fig. 4.22, ▶ Fig. 4.23). Features of this space (particularly its depth) vary significantly and we found that it could range from a total absence due to a complete development of the medial aspect of the pyramidal process, up to a clear representation of the subpyramidal space with significant depth. When the medial face of the pyramidal eminence was completely formed, the subpyramidal space was large and bounded by both the sinus tympani and the posterior tympanic sinus (independent morphology of the pyramidal eminence) (▶ Fig. 4.23); when the medial face of the pyramidal eminence was partially formed (partial morphology of the pyramidal eminence), the subpyramidal space was narrow and in some cases very deep and the posterior extension of this space was not explorable with an endoscope (▶ Fig. 4.21, ▶ Fig. 4.22). In some cases, the medial bony wall of the pyramidal eminence was absent and the eminence was completely merged with the medial bone of the retrotympanum; in this case, the subpyramidal space was not present (merged morphology of the pyramidal eminence) (▶ Fig. 4.24).
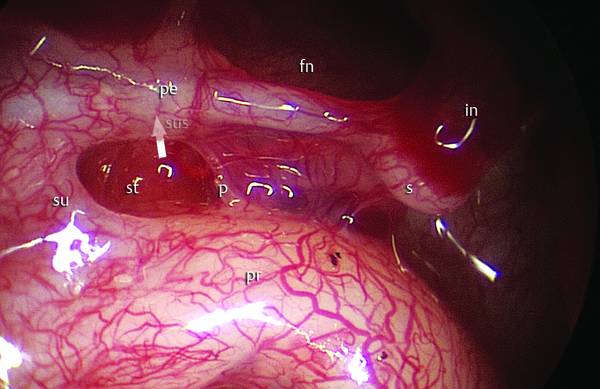
Fig. 4.20 Right ear. Endoscopic magnification of the pyramidal eminence and sinus tympani. The white arrow shows the subpyramidal space. pr, promontory; s, stapes; p, ponticulus; st, sinus tympani; pe, pyramidal eminence; fn, facial nerve; in, incus; su, subiculum; sus, subpyramidal space.
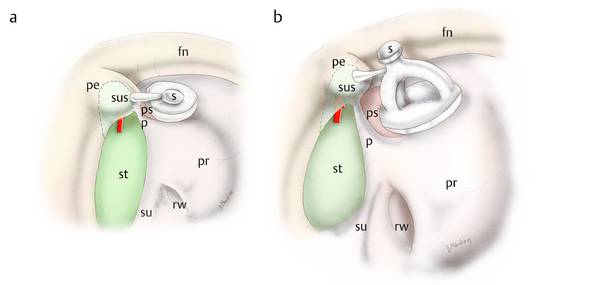
Fig. 4.21 a, b Right ear. Dependence of the subpyramidal space on the conformation of the pyramidal eminence. Partial triangular morphology of the pyramidal eminence: in this case the subpyramidal space communicates with the sinus tympani (red arrow). pr, promontory; s, stapes; p, ponticulus; st, sinus tympani; pe, pyramidal eminence; fn, facial nerve; su, subiculum; sus, subpyramidal space; ps, posterior sinus; rw, round window.
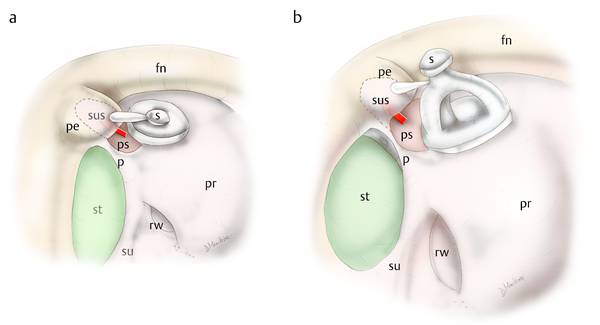
Fig. 4.22 a, b Right ear. Dependence of the subpyramidal space on the conformation of the pyramidal eminence. Partial triangular morphology of the pyramidal eminence: in this case the subpyramidal space communicates with the posterior tympanic sinus (red arrow). pr, promontory; s, stapes; p, ponticulus; st, sinus tympani; pe, pyramidal eminence; fn, facial nerve; su, subiculum; sus, subpyramidal space; ps, posterior sinus; rw, round window.
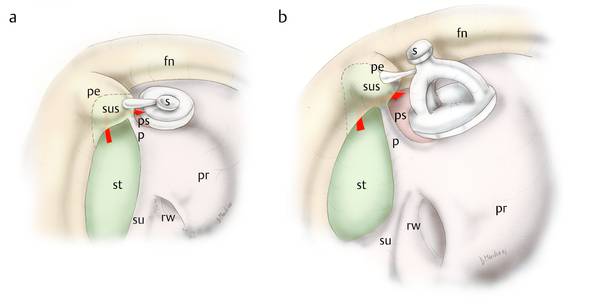
Fig. 4.23 a, b Right ear. Dependence of the subpyramidal space on the conformation of the pyramidal eminence. Complete triangular morphology of the pyramidal eminence and communicating sinus tympani and posterior tympanic sinus through the subpyramidal space (red arrow). pr, promontory; s, stapes; p, ponticulus; st, sinus tympani; pe, pyramidal eminence; fn, facial nerve; su, subiculum; sus, subpyramidal space; ps, posterior sinus; rw, round window.
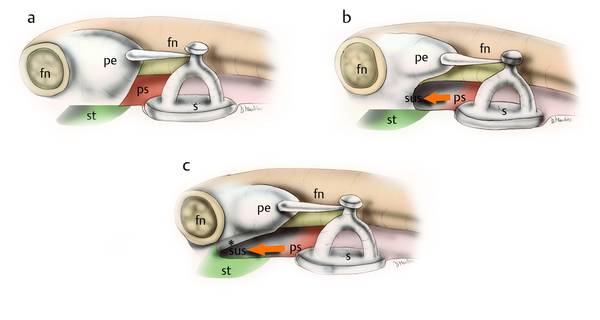
Fig. 4.24 Right ear. Different shapes of the pyramidal eminence and depths of the subpyramidal space. a Merged morphology of the pyramidal eminence without a subpyramidal space. b Partial triangular morphology of the pyramidal eminence; in this patient the subpyramidal space is quite deep and endoscopic exploration is possible. c Partial triangular morphology of the pyramidal eminence with very deep subpyramidal space; in this case endoscopic explorability is partial. Asterisk (*) marks the anatomically hidden area. pr, promontory; s, stapes; p, ponticulus; st, sinus tympani; pe, pyramidal eminence; fn, facial nerve; sus, subpyramidal space; ps, posterior sinus.
The deeper the subpyramidal space the greater the risk of a surgical approach leaving residual cholesteatoma. Hence, a good knowledge of these anatomical spaces may help in reducing the risk of residual cholesteatoma during middle ear surgery.
4.2.5 Inferior Retrotympanum
Some authors have studied the anatomy of the inferior retrotympanum, but the region has been largely neglected in the literature. This is probably because of the poor accessibility of that space during conventional microscopic procedures. In fact, Proctor in his studies7,8 had already identified almost all of the structures in that region, based on several temporal bone dissections (▶ Fig. 4.25, ▶ Fig. 4.26, ▶ Fig. 4.27). He identified a fairly constant structure, a ridge of bone connecting the basal helix of the cochlea to the jugular wall of the tympanum, in relation to the anterior pillar of the round window niche: the sustentaculum promontorii. He called it the sustentaculum (from the Latin sustentaculum, support) because he thought that it sustained the inferior tympanic artery, enveloping it during the development of the middle ear. The present authors have confirmed the presence of that structure in relation to the anterior pillar of the round niche, identifying two variants: a ridge shape and a bridge shape. We decided to rename the sustentaculum promontorii the finiculus for several reasons. First of all, we deem it quite unlikely that the inferior tympanic artery always lies in this structure, particularly in the case of the bridge shape, since it could be a very thin structure in some cases. Moreover, we wanted to identify a clear borderline between the retrotympanum and the hypotympanum, and for this we chose the name finiculus (from the Latin finis, borderline). This anatomical structure can have different conformations (▶ Fig. 4.28, ▶ Fig. 4.29).
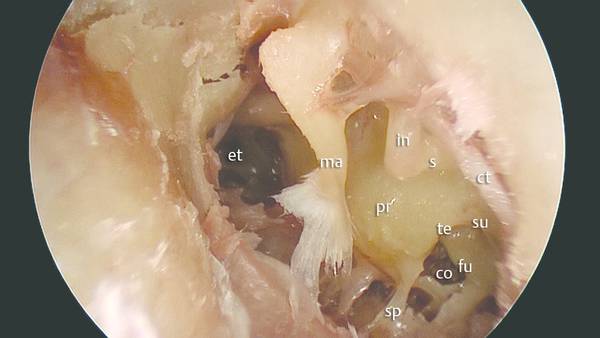
Fig. 4.25 Left ear. Transcanal endoscopic view of the inferior retrotympanum and hypotympanum. pr, promontory; s, stapes; in, incus; ma, malleus; te, tegmen of round window niche; su, subiculum; fu, fustis; co, sinus concameratus; sp, sustentaculum promontorii; et, eustachian tube; ct, chorda.
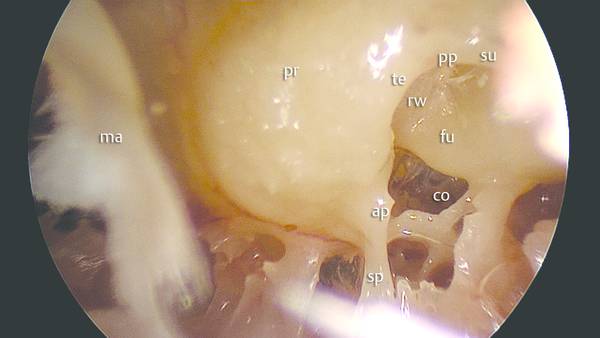
Fig. 4.26 Left ear. Endoscopic magnification of the inferior retrotympanum (0° endoscope) and round window niche. pr, promontory; te, tegmen of round window niche; su, subiculum; fu, fustis; co, sinus concameratus; sp, sustentaculum promontorii; ma, malleus; ap, anterior pillar; pp, posterior pillar; rw, round window.
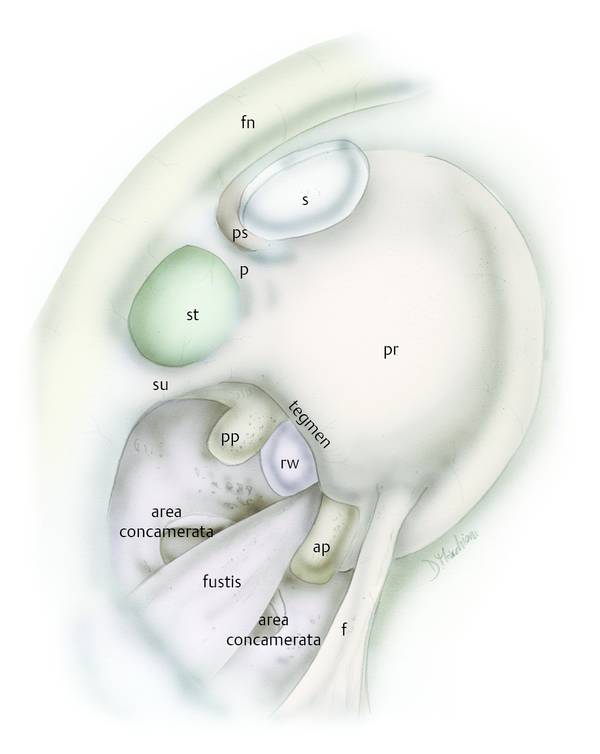
Fig. 4.27 Right ear. Drawing showing Proctor’s anatomical identification of the inferior retrotympanum and round window niche. pr, promontory; su, subiculum; fu, fustis (Proctor’s sustentaculum promontorii); ap, anterior pillar; pp, posterior pillar; rw, round window; p, ponticulus; st, sinus tympani; ps, posterior sinus; s, stapes; fn, facial nerve.