Exclusively Endoscopic Treatment of Retrotympanic Cholesteatoma
13.1 Surgical Anatomy
The retrotympanum is located in the posterior portion of the middle ear and houses a number of important anatomical and surgical structures (▶ Fig. 13.1). The sinus tympani is the most important space and is represented by a posterior outpouching cavity lying between the medial wall of the middle ear medially and the pyramidal eminence laterally, and delineated posterolaterally by the second genu and third tract of the seventh cranial nerve; anteriorly it is in a close relationship with the superior portion of the promontory. It is bordered superiorly by the ponticulus, which separates it from the posterior tympanic sinus (▶ Fig. 13.2) (a bone niche of the superior portion of the retrotympanum not always present, depending on the presence of ponticulus and the extension of the sinus tympani), and the oval window; and inferiorly by the subiculum, which separates it from the inferior retrotympanum and round window. On the basis of the depth, the sinus tympani can be divided into three types depending on its posterior extension with respect to the third segment of the facial nerve (▶ Fig. 13.3, ▶ Fig. 13.4).
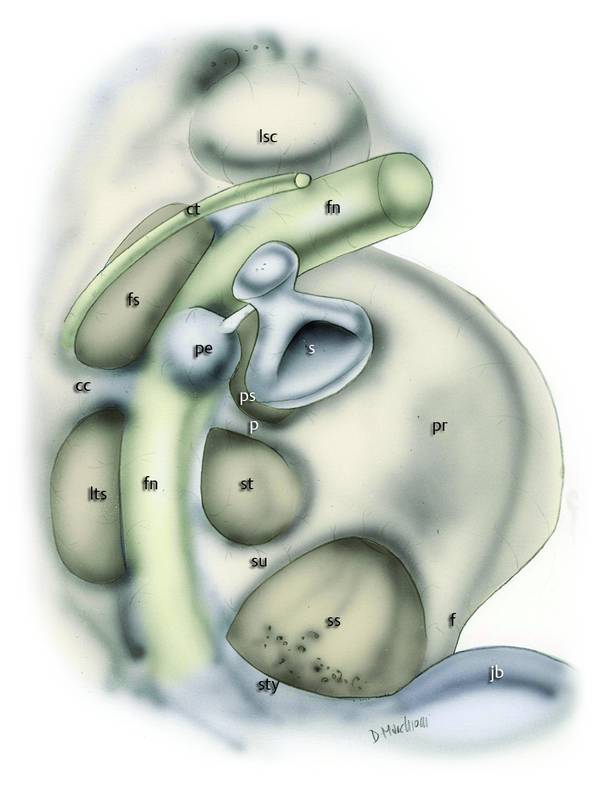
Fig. 13.1 Right ear. Anatomical global view of the retrotympanum. fn, facial nerve; s, stapes; st, sinus tympani; ps, posterior sinus; ss, sinus subtympanicus; p, ponticulus; su, subiculum; f, finiculus; fs, facial sinus; its, inferior tympanic sinus; cc, crista chordalis; ct, chorda tympani; lsc, lateral semicircular canal; sty, styloid complex; jb, jugular bulb; pr, promontory; pe, pyramidal eminence.
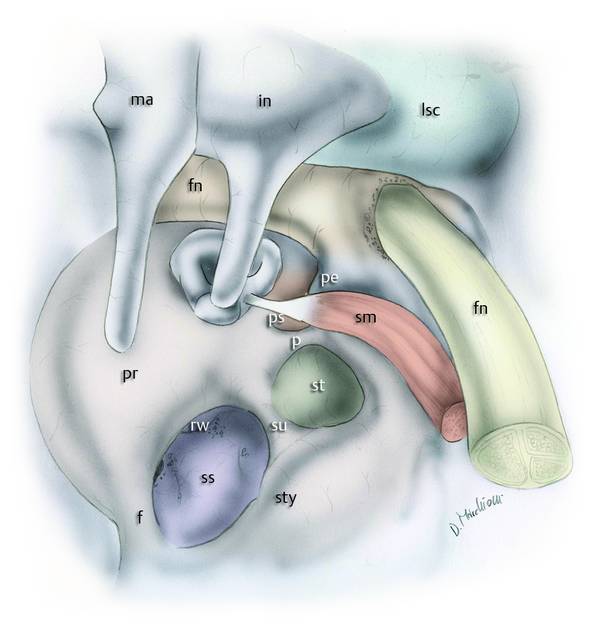
Fig. 13.2 Left ear. Anatomical relationships of the sinus tympani with the surrounding structures; the facial nerve and the pyramidal eminence with the muscle form the posterolateral limit of the sinus tympani. fn, facial nerve; in, incus; ma, malleus; st, sinus tympani; ps, posterior sinus; ss, sinus subtympanicus; p, ponticulus; su, subiculum; f, finiculus; lsc, lateral semicircular canal; sty, styloid complex; pr, promontory; pe, pyramidal eminence; sm, stapedial muscle; rw, round window.

Fig. 13.3 Right ear. Sinus tympani (ST) depth classification in relation to the seventh cranial nerve. Type A, small sinus tympani. The medial limit of the third segment of the facial nerve corresponds to the depth of the sinus. In these cases, the ST is small and does not present an extension medial and posterior to the facial nerve. Type B, deep sinus tympani. The medial boundary of the ST lies medially with respect to the third segment of the facial nerve and the ST does not present an extension posterior to the facial nerve. Type C, deep sinus tympani with posterior extension. The medial boundary of the ST lies medial and posterior to the third segment of the facial nerve. In these cases, the ST is very large and deep and all these patients have a well-developed mastoid.
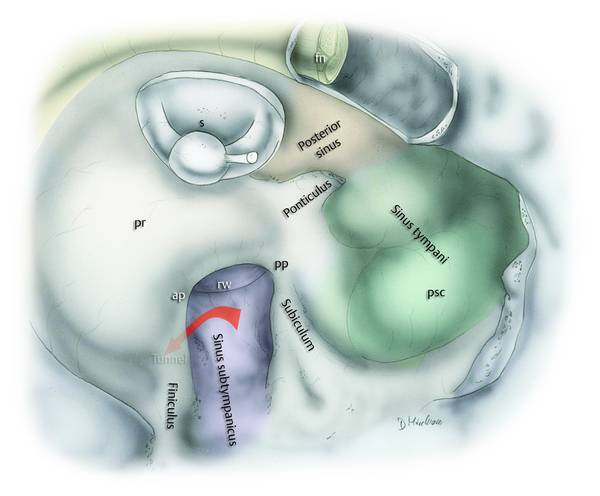
Fig. 13.4 Left ear. Sinus tympani (ST) dissection after removal of the pyramidal eminence, fallopian canal, and second genu of the seventh cranial nerve and section of the ponticulus. Exploration of the medial aspect of the ST in this case (type C) shows close relationship with the posterior semicircular canal. Note the presence of a particularly deep sinus subtympanicus. The red arrow shows the deep tunnel under the finiculus crest inferior to the round window membrane. pp, posterior pillar; ap, anterior pillar; s, stapes; pr, promontory; rw, round window; fn, facial nerve; psc, posterior semicircular canal.
Lateral and posterior to the second genu and vertical portion of the seventh cranial nerve are two anatomical bone niches: the facial sinus and the lateral tympanic sinus (▶ Fig. 13.1). These are separated by the chordal ridge, originating from the posterior portion of the pyramidal eminence. These anatomical regions are more accessible than the sinus tympani and posterior tympanic sinus because they are located laterally to a plane tangential to the seventh cranial nerve course and the anatomy of the facial sinus and the lateral tympanic sinus is more constant.
The pyramidal eminence is a triangular bony structure with its base oriented posteriorly and the tip anteriorly, that houses the stapes tendon and is oriented horizontally, lying anteriorly and laterally to the second genu of the facial nerve. Under this bone structure located in the middle of the retrotympanum can be found the subpyramidal space that is delimited laterally by the medial aspect of the pyramidal eminence, medially by the medial side of the bony wall of the retrotympanum, and posteriorly by the vertical tract of the seventh cranial nerve (▶ Fig. 13.5). This space exhibits varying morphology, mostly in terms of its depth, ranging from a total absence due to a total ossification of the medial aspect of the pyramidal eminence with the medial wall of the retrotympanum to a particularly deep subpyramidal space lying beneath the facial nerve. It can be included in the sinus tympani space or in the posterior tympanic sinus depending on the position and orientation of the ponticulus.
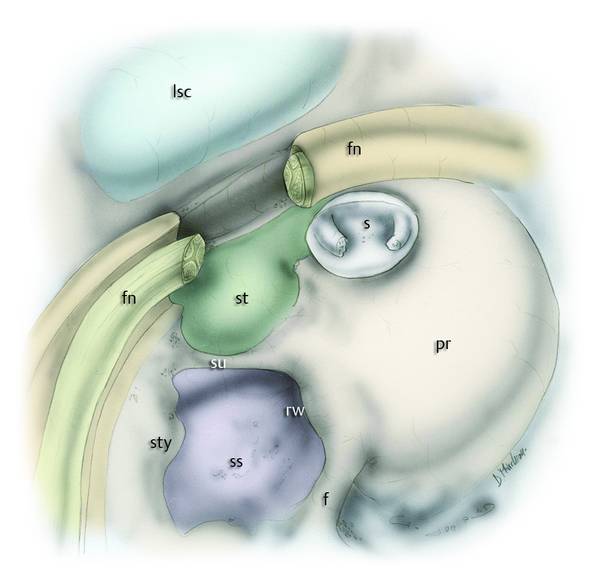
Fig. 13.5 Right ear. Subpyramidal space anatomical dissection. To expose this particular sinus we performed a partial removal of the pyramidal eminence and fallopian canal (second genu) and section of the seventh cranial nerve. Note the relationship of the medial and posterior aspects of the sinus tympani with the medial aspect of the fallopian canal and the exposure of the subpyramidal space. lsc, lateral semicircular canal; st, sinus tympani; su, subiculum; ss, sinus subtympanicus; f, finiculus; sty, styloid complex; pr, promontory; fn, facial nerve; rw, round window; s, stapes.
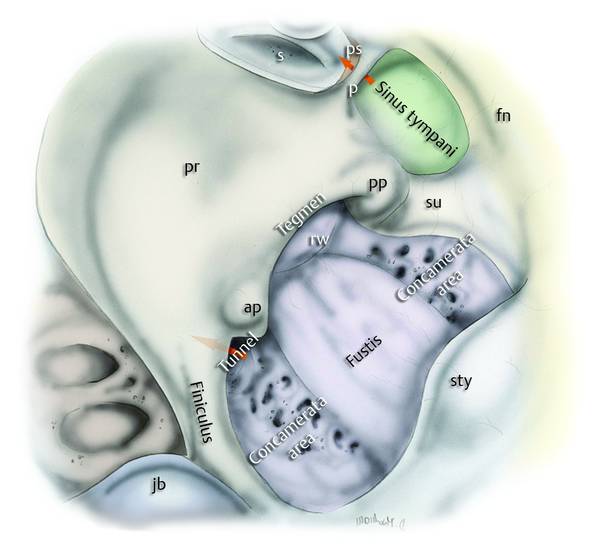
Fig. 13.6 Left ear. Subtympanic sinus and related areas (purple). This sinus is located between the subiculum superiorly and the finiculus inferiorly, and is confluent with the styloid complex posteriorly. Note the presence of a chambered pneumatized area delimiting a particularly bony area (termed the fustis) and the presence of a deep tunnel beneath and close to the junction between the finiculus and the anterior pillar of the round window. In some cases it is possible to find a particularly deep tunnel that can reach the carotid canal. Red arrows: the upper arrow indicates the communicating space under the ponticulus between the sinus tympani and the posterior sinus; the lower arrow indicates the tunnel under the finiculus into the subtympanic sinus. fn, facial nerve; s, stapes; ps, posterior sinus; p, ponticulus; su, subiculum; sty, styloid complex; pr, promontory; rw, round window; jb, jugular bulb; ap, anterior pillar; pp, posterior pillar.
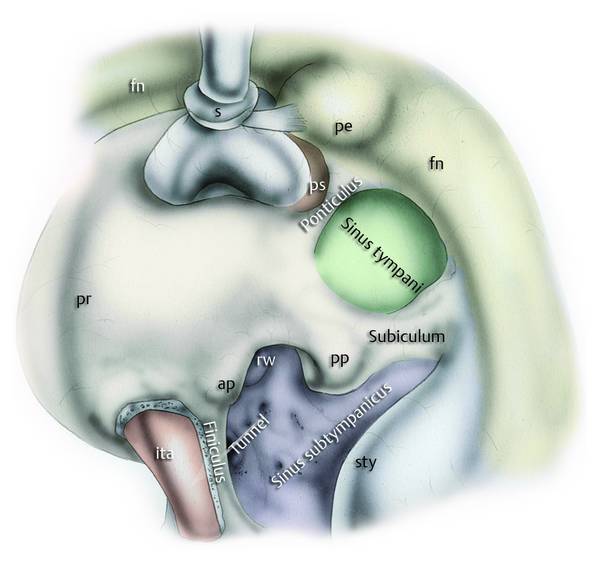
Fig. 13.7 Left ear. Subtympanic sinus and finiculus region after partial removal of the finiculus. In some cases it is possible to find the inferior tympanic artery inside the bony structure of the finiculus with a course parallel to the finiculus. The white arrow indicates the position of the tunnel under the finiculus; fn, facial nerve; s, stapes; ps, posterior sinus; sty, styloid complex; pr, promontory; rw, round window; ap, anterior pillar; pp, posterior pillar; pe, pyramidal eminence; ita, inferior tympanic artery.
The inferior retrotympanum is the posterior space that houses the sinus subtympanicus (▶ Fig. 13.6, ▶ Fig. 13.7), delimited posteriorly by the styloid complex and the third segment of the seventh cranial nerve, anteriorly by the round window with its anterior and posterior pillar and tegmen and the inferior and posterior portion of the promontory, superiorly by the subiculum, and inferiorly by the jugular bulb and finiculus: a bone ridge of variable shape, arising from the inferior portion of the styloid prominence and connected to the anterior and inferior lip of the round window.
The sinus subtympanicus (previously termed the area concamerata by Proctor) is difficult to identify and moreover its posterior portion is delimited by the styloid segment and the third segment of the facial nerve laterally and the otic capsule medially. In some individuals, posterior pneumatization into the subtympanic sinus is evident medially with respect to the styloid complex, creating a deep space where a residual cholesteatoma could be present.
For a thorough anatomical description, refer to Chapter ▶ 3.
13.2 History
Cholesteatoma involving the retrotympanic space poses two important clinical risks: (1) the potential for residual disease due to incomplete removal of the diseased tissue, and (2) increased risk of ossicular discontinuity, hearing loss, and seventh cranial nerve injuries due to cholesteatoma, which the surgeon cannot control. Maximum exposure of this region is essential for a complete removal of the pathology and to avoid these risks. Various surgical techniques with the microscope to better expose this region have been proposed over the years and consist of (a) changing the position of the surgeon or the patient’s head (though often this does not allow good exposure because of the height of the external ear canal2; (b) the facial recess approach, dissecting the triangular bony area delimited by the seventh cranial nerve anteriorly, the lateral semicircular canal posteriorly, and the posterior semicircular canal medially (however, this technique poses high risk for injuries and is feasible only in the presence of a deep sinus tympani3; (c) classical and radical tympanoplasty requiring a posterior tympanotomy, which cannot always guarantee good exposure of the retrotympanic space (▶ Fig. 13.8, ▶ Fig. 13.9).
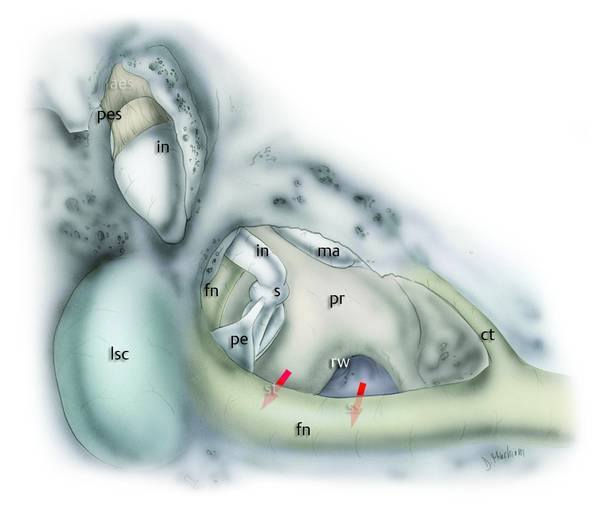
Fig. 13.8 Right ear. Transmastoid microscopic exposure of the retrotympanum after wide posterior tympanotomy. Note how the sinus tympani (st) and subtympanic sinus (ss) positions are completely covered by the second genu and third tract of the seventh cranial nerve. fn, facial nerve; s, stapes; pr, promontory; rw, round window; pe, pyramidal eminence; in, incus; ma, malleus; pes, posterior epitympanic space; lsc, lateral semicircular canal; ct, chorda tympani.
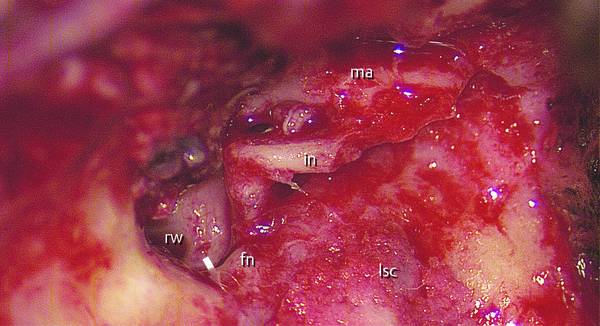
Fig. 13.9 Clinical case. Left ear. After canal wall down technique for a cholesteatoma, we can observe the anatomical relationship between the facial nerve and the medial retrotympanum. The second genu of the facial nerve is covering the medial portions of the retrotympanum. fn, facial nerve; in, incus; ma, malleus; rw, round window; lsc, lateral semicircular canal. The white arrow indicates the medial retrotympanum.
Endoscopic approaches to the retrotympanum (with 0°, 45°, or 70° optics) ensure the complete visualization of the surgical spaces described above and this technique allows surgeons to completely visualize the anatomical variations and pathological tissues (▶ Fig. 13.10, ▶ Fig. 13.11, ▶ Fig. 13.12, ▶ Fig. 13.13).4–7

Fig. 13.10 Endoscopic exposure of the sinus tympani (45° endoscope). a Left ear. Sinus tympani with partitioned shape: a ridge of bone extending from the inferior portion of the pyramidal eminence inferiorly with respect to the ponticulus is noted. This crest of bone divides the sinus tympani into two portions (superior and inferior). b Left ear. Sinus tympani with classic shape: a bridge ponticulus is detected. A communicating space between the sinus tympani and the posterior sinus is present. fn, facial nerve; s, stapes; ps, posterior sinus; ss, sinus subtympanicus; p, ponticulus; rw, round window; in, incus; pe, pyramidal eminence; st, sinus tympani; su, subiculum; sty, styloid complex.
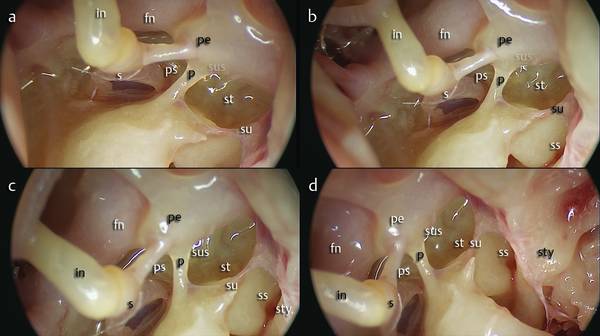
Fig. 13.11 a–d Left ear. View with a 45° endoscope. Sinus tympani type B and a deep subpyramidal space in a patient with a complete pyramidal eminence. There is communication between the sinus tympani and the posterior sinus through the subpyramidal space. fn, facial nerve; ps, posterior sinus; ss, sinus subtympanicus; p, ponticulus; in, incus; s, stapes; pe, pyramidal eminence; sus, subpyramidal space; su, subiculum; st, sinus tympani; sty, styloid complex.
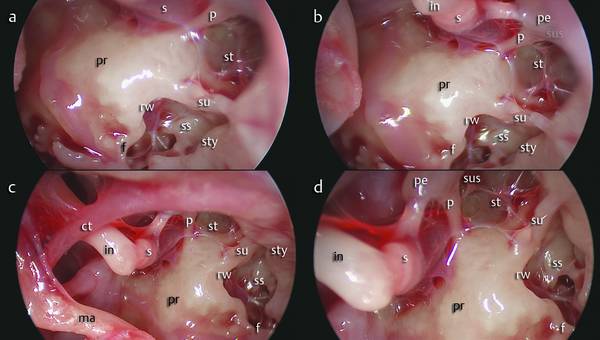
Fig. 13.12 a–d Left ear. View with a 45° endoscope of the entire medial retrotympanum. Note the depth of the sinus tympani (type B) with its extension medially with respect to the seventh cranial nerve and a wide subpyramidal space linked to the sinus tympani. Note also the sinus subtympanicus with a chambered pneumatized area located posteriorly to the fustis with the presence of a tunnel beneath the area of the finiculus and near the anterior pillar of the round window. ss, sinus subtympanicus; p, ponticulus; st, sinus tympani; rw, round window; in, incus; s, stapes; pe, pyramidal eminence; sus, subpyramidal space; su, subiculum; f, finiculus; ma, malleus; pr, promontory; sty, styloid complex.
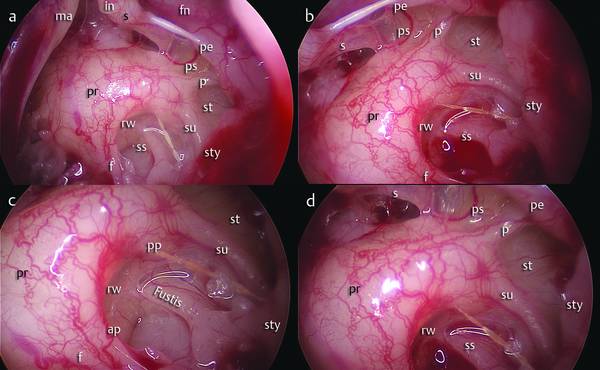
Fig. 13.13 Left ear. Intraoperative view with a 45° endoscope of the retrotympanic spaces. In this patient the sinus tympani exhibits a classic conformation between the ponticulus and the subiculum (a, b); endoscopic magnification of the subtympanic sinus shows the styloid prominence, the fustis, and the round window niche anteriorly (c, d). fn, facial nerve; s, stapes; ps, posterior sinus; ss, subtympanicus sinus; p, ponticulus; su, subiculum; sty, styloid complex; pr, promontory; rw, round window; ap, anterior pillar; pp, posterior pillar; ma, malleus; in, incus; pe, pyramidal eminence; st, sinus tympani; ps, posterior sinus; f, finiculus.
13.3 Advantages
A direct minimally invasive surgical approach to the middle ear avoiding removal of mastoid bone and mucosa
Direct visualization of the retrotympanum and surrounding structures such as ossicular chain, chorda tympani, seventh cranial nerve, and round and oval windows
Wide exposure of the retrotympanic region both medially (sinus tympani, sinus subtympanicus, subpyramidal space) and laterally (facial sinus, lateral sinus).
13.4 Indications and Contraindications
13.4.1 Indications
Cholesteatoma or pars tensa retractions of the middle ear involving the retrotympanic region.
13.4.2 Contraindications
Narrow external ear canal
External ear malformation.
13.5 Complications
Stapes fracture (possible in first surgical approaches and for surgeons with little experience with endoscopes or otoneurological surgery)
Seventh cranial nerve injury (possible in cases of severe bleeding with poor vision of the surgical field)
Key point: Generally the seventh cranial nerve is located in front of the surgeon, specially the second tract and the second genu of the nerve.
Cochlear injury secondary to drilling of the finiculus.
Key point: Avoid drilling in the subtympanic sinus and if possible prefer the use of a curette.
13.6 Surgical Steps
Using a 0° endoscope, the external auditory canal is infiltrated with a mix of mepivacaine 2% with epinephrine about 3 minutes before the surgical approach. The incision of the external auditory canal is made about 0.5 to 1 cm lateral of the fibrous anulus (4 o’clock position to 1 o’clock position) and can be made with a molecular resonance scalpel (Vesalius), a flexible carbon dioxide laser, or a scalpel (▶ Fig. 13.14; see also Clinical case 2).
A tympanomeatal flap is detached from the bone using cottonoids soaked in epinephrine (50% with physiological saline). Flap dissection proceeds medially, pushing the skin anteriorly, encompassing the incision until the fibrous anulus is identified. A curved dissector is used to dissect the flap, paying attention to scraping the dissector on the bone of the external auditory canal.
Key point: There may be massive bleeding after incision of the skin of the external auditory canal; this should be controlled by the use of epinephrine-soaked cottonoids placed on the point of bleeding for about 1 minute.
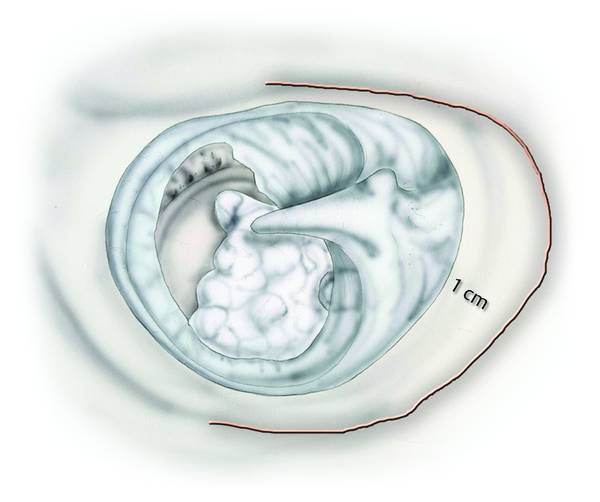
Fig. 13.14 Left ear. Drawing showing the line of incision of the external auditory canal.
The fibrous anulus is raised through the use of microforceps, and hook-up allows good exposure of the middle ear. During the pars flaccida dissection special attention should be paid to avoiding any damage to the membrane. In this phase of dissection, surgical maneuvers to separate the tympanic membrane from the lateral process of the malleus and from the anterior malleolar ligament must be extremely gentle (▶ Fig. 13.15; see also Clinical case 2). The use of microforceps is useful to obtain a good caudal overturning of the tympanic flap, thereby also exposing the protympanic region. The flap is anchored at the umbus and overturned anteriorly-inferiorly, allowing good exposure of the mesotympanic and retrotympanic region.
Key point: In the case of invasion of the subtympanic sinus with partial invasion in the hypotympanum by the cholesteatoma, the tympanic flap can be completely mobilized by cutting the ligament at the umbus. This offers extensive exposure of the whole tympanic cavity with easy access to the entire retrotympanum (▶ Fig. 13.16; see also Clinical case 2; ▶ Fig. 13.30).
Using a 0° endoscope, the tympanic cavity is exposed and the incudostapedial joint (and the anatomical status of the articulation of the ossicular chain), the second genu of the seventh cranial nerve, and the pyramidal eminence are identified so as to correctly evaluate the extension of the cholesteatoma and its relationships with the surrounding structures (▶ Fig. 13.21, ▶ Fig. 13.22).



