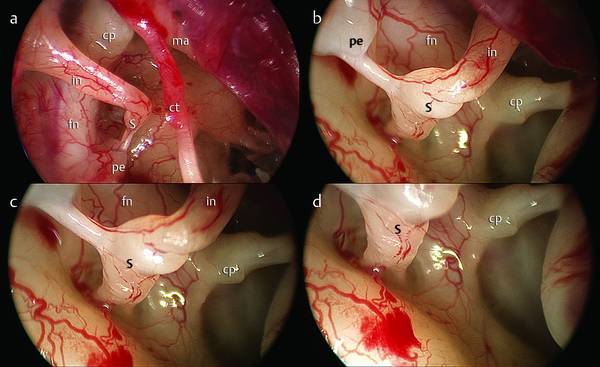
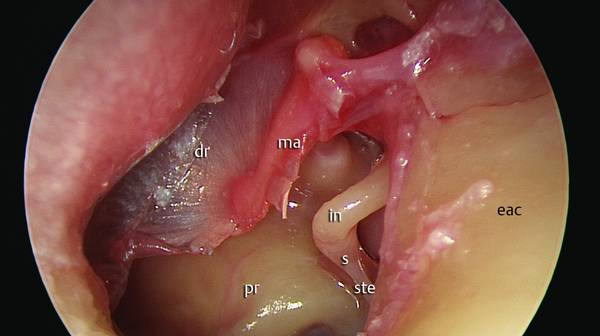
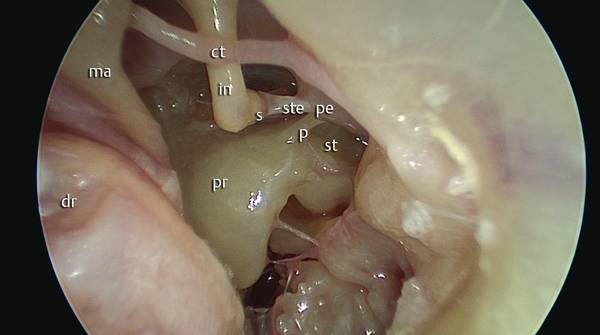
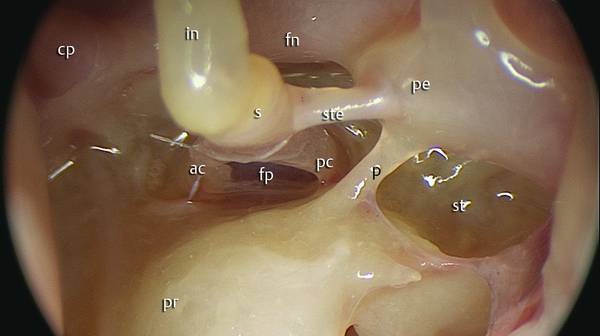
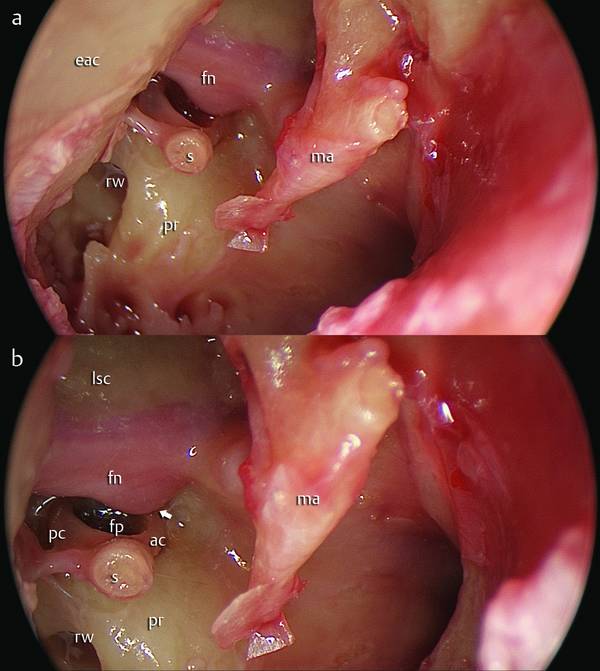
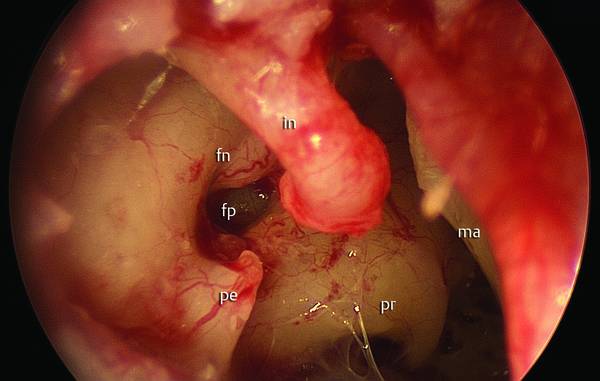
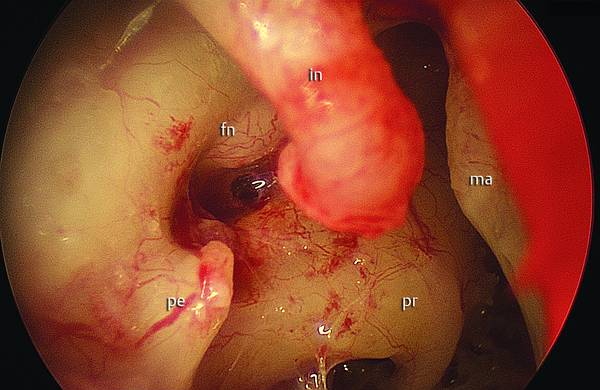
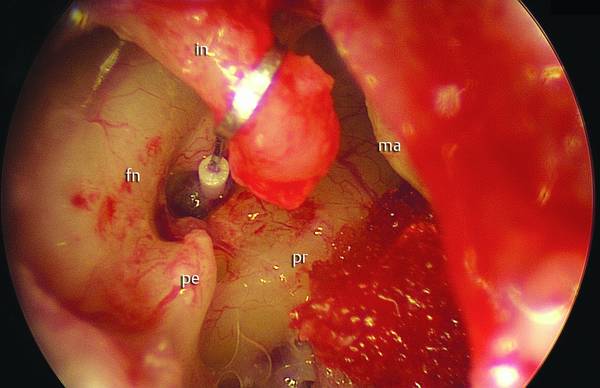
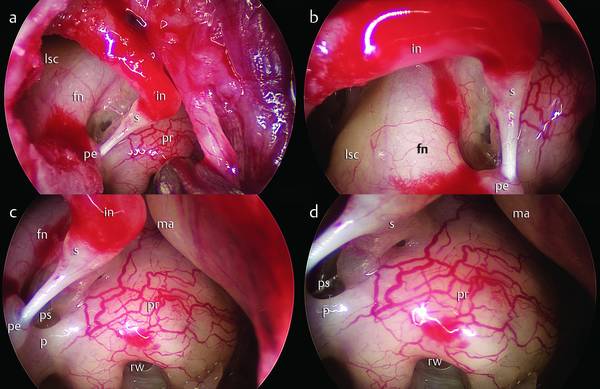
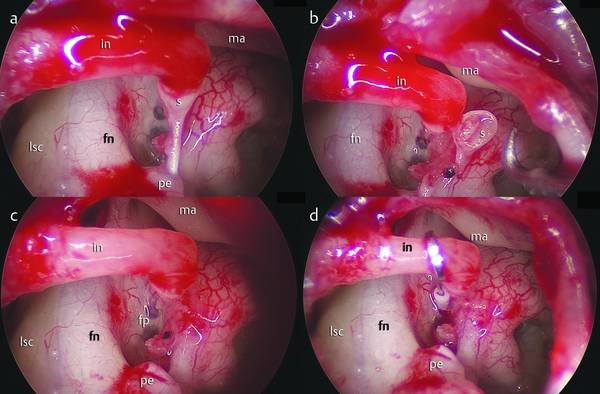
Endoscopic Transcanal Stapes Surgery (Stapedotomy) Since the introduction of the classic stapedectomy technique by Shea,1 many different procedures have been described in the literature from the microscopic point of view.6 Although it has been more than 15 years since the introduction of operative endoscopy to middle ear surgery there is still a very limited role for endoscopes in the surgical management of middle ear diseases and otosclerosis.2–6 There are several possible reasons for this, including a prevalent perception of a limited and marginal role for endoscopes in middle ear surgery, and a potentially long learning period due to the difficulties and tribulations of adapting new techniques and new instrumentation to one-hand work practices.3,4 The operating microscope provides a very good-quality magnified image in a straight line, but the surgeon’s field of view is limited to the narrowest segment of the ear canal.3,4 As is well known, traditional microscopic stapedotomy requires removal of the posterior bony wall of the external auditory canal (EAC) and manipulation of the chorda tympani to obtain an optimal exposition of the oval window niche.2,7 During the microscopic approach to the oval window niche, the chorda tympani is in the middle of the surgical field, impeding optimal access to the window or making the resection of the bony wall of the EAC more difficult. In these cases, injury to the nerve is a possibility and loss, impairment, or alteration of the sense of taste are recognized possible sequelae of microscopic stapedotomy.2 Another consideration with the microscopic approach is the visibility of the superstructure of the stapes. When using the microscope the surgeon cannot directly see the anterior crus of the stapes, so that the removal of the superstructures of the stapes will be a blind maneuver. The objective of this chapter is to demonstrate the use of the endoscope during stapes surgery in patients with otosclerosis, illustrating the relevant surgical anatomy,8–11 surgical steps, and possible complications and results, and discussing the advantages and disadvantages of this instrument in this type of surgery. The main advantages of this procedure are that there is virtually no trauma to the chorda tympani in the cases where there is no curetting or drilling, and that one has excellent visualization of the anterior crus of the stapes, its superstructure, and the oval window niche (▶ Fig. 16.1, ▶ Fig. 16.2, ▶ Fig. 16.3). When using an endoscope of 4 mm or 3 mm diameter and 18 cm or 14 cm long, the surgeon also gets a magnified view and the ability to change rapidly from a close-up to a wide-angle view simply by moving closer or withdrawing the instrument,2 as well as all-round vision. In cases of facial prolapse or dehiscence the use of an endoscope may give some advantages in correctly visualizing the footplate of the stapes (platina) and performing stapedotomy in the right position, avoiding any risk of facial nerve lesion (▶ Fig. 16.4, ▶ Fig. 16.5, ▶ Fig. 16.6, ▶ Fig. 16.7). Moreover, with the endoscope the anatomy can be studied very closely and very precisely8–10 (▶ Fig. 16.8, ▶ Fig. 16.9), and this can be useful, for example, in cases of stapes malformation (▶ Fig. 16.10, ▶ Fig. 16.11) or in revision cases (▶ Fig. 16.12). In cases of stapes malformation it may be difficult to understand the real relationship between the surrounding anatomical structures with the microscope. Endoscopic magnification and the use of endoscopes with different angles of view allows us to verify the type of stapes malformation, and so perform a safe stapedectomy avoiding injury to the facial nerve and other important structures (▶ Fig. 16.13, ▶ Fig. 16.14). Disadvantages of the procedure include the lack of a stereoscopic view, the inability to work bimanually, and a significant burden of learning. Fig. 16.1 Left ear. Endoscopic surgical anatomy. Image with a 0°, 4-mm endoscope. dr, eardrum; ma, malleus; in, incus; ste, stapes tendon; s, stapes; pr, promontory; eac, external auditory canal. Fig. 16.2 Left ear. Endoscopic surgical anatomy of the oval window niche. Image with a 30°, 4-mm endoscope. dr, eardrum; ma, malleus; in, incus; ste, stapes tendon; s, stapes; pr, promontory; ct, chorda tympani; st, sinus tympani; p, ponticulus. Fig. 16.3 Left ear. A close-up view of the oval window niche and stapes. Image with a 30° endoscope. in, incus; ste, stapes tendon; s, stapes; pr, promontory; st, sinus tympani; p, ponticulus fn, facial nerve; ac, anterior crus of stapes; pc, posterior crus of stapes; fp, stapes footplate; pe, pyramidal eminence; cp, cochleariform process. Fig. 16.4 Right ear. a Endoscopic anatomy of the medial aspect of the tympanic cleft. b A closer view. The arrow indicates facial nerve dehiscence. Note the very close relationship between the nerve and the anterior crus (ac), with consequent risk of damage to the nerve. lsc, lateral semicircular canal; fn, facial nerve; ma, malleus; pr, promontory; fp, stapes footplate; rw, round window; pc, posterior crus; ac, anterior crus; s, stapes; eac, external auditory canal. Fig. 16.5 Right ear. A close-up view of the stapedial region. In this case the facial nerve dehiscence and the particular anatomy tend to hide the oval window region, making surgical maneuvers difficult. pe, pyramidal eminence; fp, stapes footplate; fn, facial nerve; pr, promontory; ma, malleus; in, incus. Fig. 16.6 Right ear. A closer view of the same case. The hole in the footplate has been made endoscopically. pe, pyramidal eminence; fn, facial nerve; pr, promontory; ma, malleus; in, incus. Fig. 16.7 Right ear. Endoscopic view after stapedial piston placement. pe, pyramidal eminence; fn, facial nerve; pr, promontory; ma, malleus; in, incus. Fig. 16.8 Right ear. A further case of endoscopic stapes surgery. a Endoscopic anatomy of the medial aspect of the tympanic cleft after elevation of the tympanomeatal flap. b Relationship of the oval window to facial nerve. c, d Relationship of the oval window region with promontory. pe, pyramidal eminence; fn, facial nerve; pr, promontory; ma, malleus; in, incus; lsc, lateral semicircular canal; rw, round window; p, ponticulus; ps, posterior tympanic sinus. Fig. 16.9 Right ear. Surgical steps of stapedoplasty. a Crura section after stapedotomy. b Removal of the stapes superstructure. c Visualization of the oval window. d Placement of the piston. pe, pyramidal eminence; fp, stapes footplate; fn, facial nerve; ma, malleus; in, incus; lsc, lateral semicircular canal; s, stapes.
16.1 History
16.2 Advantages
Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine