 Vascular Tumors and Malformations of the Uvea
Vascular Tumors and Malformations of the UveaCircumscribed Choroidal Hemangioma
General Considerations
Several vascular tumors and malformations can affect the uveal tract. The most important is choroidal hemangioma, which can occur as a circumscribed tumor or as a diffuse lesion in patients with variations of the Sturge-Weber syndrome. This section covers the subject of circumscribed choroidal hemangioma, a benign vascular tumor that has been the subject of considerable attention in the literature (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45). Its etiology in unknown, but it is usually diagnosed in adulthood when it becomes symptomatic. It is speculated that some cases may be congenital or develop in early childhood. Circumscribed choroidal hemangioma usually has typical clinical features.
Clinical Features
Circumscribed choroidal hemangioma is almost always unilateral. It appears as a subtle, red-orange mass in the posterior choroid. It can produce visual loss because of a subfoveal location or a secondary retinal detachment that involves the fovea (1, 2, 3, 4, 5, 6). It can induce hyperplasia and fibrous metaplasia of the overlying pigment epithelium, which can sometimes lead to diagnostic confusion with melanoma. In addition to retinal detachment, secondary retinoschisis commonly occurs over or adjacent to the tumor. Occasionally, neovascular glaucoma can develop, and the subsequent pain may necessitate enucleation (8,45).
Diagnostic Approaches
Fluorescein angiography typically shows hyperfluorescence of the tumor blood vessels in the pre-arterial phase and diffuse late staining of the mass (1,2,6,11). Indocyanine green angiography reveals early filling of the lesion and a characteristic “wash out” of the hyperfluorescence in the later frames (12,22,27). A-scan ultrasonography shows high internal reflectivity within the tumor, and B-scan ultras onography shows a placoid or ovoid choroidal mass pattern with acoustic solidity. Ultrasonography occasionally demonstrats a highly reflective plaque over the tumor surface, which corresponds to fibrous or osseous metaplasia of the overlying RPE (2). Computed tomography and magnetic resonance can also demonstrate choroidal hemangioma, but the results are not necessarily diagnostic. With MRI, choroidal hemangioma generally differs from other intraocular tumors in that it is hyperintense to vitreous on T1-weighted images and isointense on T2-weighted images. Most other intraocular tumors are hypointense on T2 images (2).
Pathology
Grossly, a circumscribed choroidal hemangioma is a red placoid or ovoid choroidal tumor. Microscopically, it is usually composed of large congested blood vessels separated by rather thin intervascular septae. Overlying cystoid retinal edema and retinoschisis are consistent features over choroidal hemangiomas that come to histopathologic examination (2,3).
Management
There have been a number of recent publications on the management of circumscribed choroidal hemangioma. If the affected patient is asymptomatic, no treatment is necessary. When there is visual loss because of a serous detachment of the fovea, the traditional treatment has been laser photocoagulation to the tumor surface to induce resolution of the subretinal fluid (1,2,4,13,15). Plaque or external beam radiotherapy can be employed in cases with more advanced detachment (16, 17, 18, 19, 20,37,38). Plaque radiotherapy has been effective in treating choroidal hemangioma with total retinal detachment resulting in reattachment of the retina (17). External beam irradiation, delivering about 2000 cGy to the whole eye, has been effective in bringing about a decrease in tumor thickness and resolution of the retinal detachment for both circumscribed and diffuse choroidal hemangioma.
There has been recent enthusiasm for other methods of treatment. Transpupillary thermotherapy has met with some success (23, 24, 25, 26,33,41). In recent years, a number of authors have reported good results with photodynamic therapy (PDT), using a method similar to that used for age-related macular degeneration (28,29,31, 32, 33, 34). Optical coherence tomography has been used to document the presence of cystoid retinal edema and subretinal fluid before and after PDT. We have seen a dramatic resolution of these findings and a significant return of vision in a number of patients treated with PDT. In rare instances, neovascular glaucoma may necessitate enucleation (7).
Selected References
1. Gass JDM. Stereoscopic Atlas of Macular Diseases, 4th ed. St. Louis: CV Mosby; 1997:208-212.
2. Shields JA, Shields CL. Vascular tumors of the uvea. In: Shields JA, Shields CL, eds. Intraocular Tumors. A Text and Atlas. Philadelphia: WB Saunders; 1992:252-255.
3. Witschel H, Font RL. Hemangioma of the choroid. A clinicopathologic study of 71 cases and a review of the literature. Surv Ophthalmol 1976;20: 415-431.
4. Anand R, Augsburger JJ, Shields JA. Circumscribed choroidal hemangiomas. Arch Ophthalmol 1989;107:1338-1342.
5. Mashayekhi A, Shields CL. Circumscribed choroidal hemangioma. Curr Opin Ophthalmol 2003;14:142-149.
6. Shields CL, Honavar SG, Shields JA, et al. Circumscribed choroidal hemangioma: clinical manifestations and factors predictive of visual outcome in 200 consecutive cases. Ophthalmology 2001;108:2237-2248.
7. Shields JA, Mashayekhi A, Ra S, et al. Pseudomelanomas of the posterior uveal tract. The 2006 Taylor Smith Lecture. Retina 2005;25:767-771.
8. Shields JA, Stephens RF, Eagle RC Jr, et al. Progressive enlargement of a circumscribed choroidal hemangioma. A clinicopathologic correlation. Arch Ophthalmol 1992;110:1276-1278.
9. Cohen VM, Rundle PA, Rennie IG. Choroidal hemangiomas with exudative retinal detachments during pregnancy. Arch Ophthalmol 2002;120: 862-864.
10. Amirikia A, Scott IU, Capo H, et al. Increasing hyperopia and esotropia as the presenting signs of bilateral diffuse choroidal hemangiomas in a patient with Sturge-Weber syndrome. J Pediatr Ophthalmol Strabismus 2002;39: 121-122.
11. Norton EWD, Gutman F. Fluorescein angiography of hemangiomas of the choroid. Arch Ophthalmol 1967;78:121-125.
12. Shields CL, Shields JA, De Potter P. Patterns of indocyanine green angiography of choroidal tumors. Br J Ophthalmol 1995;79:237-245.
13. Sanborn GE, Augsburger JJ, Shields JA. Treatment of circumscribed choroidal hemangiomas. Ophthalmology 1982;89:1374-1380.
14. Shields JA, Shields CL, Materin MA, et al. Changing concepts in management of circumscribed choroidal hemangioma. The 2003 J. Howard Stokes Lecture, part 1. Ophthalmic Surg Lasers 2004;35:383-393.
15. Shields JA. The expanding role of laser photocoagulation for intraocular tumors. The 1993 H. Christian Zweng Memorial Lecture. Retina 1994;14: 310-322.
16. Zografos L, Bercher L, Chamot L, et al. Cobalt-60 treatment of choroidal hemangiomas. Am J Ophthalmol 1996;121:190-199.
17. Chao AN, Shields CL, Shields JA, et al. Plaque radiotherapy for choroidal hemangioma with total retinal detachment and iris neovascularization. Retina 2001;21:682-684.
18. Shields JA. Radiotherapy of circumscribed choroidal hemangiomas. Ophthalmology 1997;104:1784.
19. Hannouche D, Frau E, Desjardins L, et al. Efficacy of proton therapy in circumscribed choroidal hemangiomas associated with serous retinal detachment. Ophthalmology 1997;104:100-103.
20. Kivela T, Tenhunen M, Joensuu T, et al. Stereotactic radiotherapy of symptomatic circumscribed choroidal hemangiomas. Ophthalmology 2003;110: 1977-1982.
21. Shields CL, Materin MA, Marr BP, et al. Resolution of advanced cystoid macular edema following photodynamic therapy of choroidal hemangioma. Ophthalmic Surg Lasers Imaging 2005;36:237-239.
22. Arevalo JF, Shields CL, Shields JA, et al. Circumscribed choroidal hemangioma: characteristic features with indocyanine green videoangiography. Ophthalmology 2000;107:344-350.
23. Vianna RN, Fernandes L, Muralha A, et al. Transpupillary thermotherapy in the treatment of circumscribed choroidal hemangiomas. Int Ophthalmol 2004;25:117-121.
24. Garcia-Arumi J, Ramsay LS, Guraya BC. Transpupillary thermotherapy for circumscribed choroidal hemangiomas. Ophthalmology 2000;107:351-356.
25. Shields CL. Discussion: transpupillary thermotherapy for circumscribed choroidal hemangiomas. Ophthalmology 2000;107:357.
26. Othmane IS, Shields CL, Shields JA, et al. Circumscribed choroidal hemangioma managed by transpupillary thermotherapy. Arch Ophthalmol 1999;117:136-137.
27. Kamal A, Watts, AR, Rennie IG. Indocyanine green enhanced transpupillary of circumscribed choroidal haemangioma. Eye 2000;14:701-705.
28. Verbraak FD, Schlingemann RO, Keunen JE, et al. Longstanding symptomatic choroidal hemangioma managed with limited PDT as initial or salvage therapy. Graefes Arch Clin Exp Ophthalmol 2003;241:891-898.
29. Porrini G, Giovannini A, Amato G, et al. Photodynamic therapy of circumscribed choroidal hemangioma. Ophthalmology 2003;110:674-680.
30. Augsburger JJ, Shields JA, Moffat KP. Circumscribed choroidal hemangiomas: long-term visual prognosis. Retina 1981;1:56-61.
31. Madreperla SA. Choroidal hemangioma treated with photodynamic therapy using verteporfin. Arch Ophthalmol 2001;119:1606-1610.
32. Schmidt-Erfurth UM, Michels S, Kusserow C, et al. Photodynamic therapy for symptomatic choroidal hemangioma: visual and anatomic results. Ophthalmology 2002;109:2284-2294.
33. Bains H, Gunduz K. Transpupillary thermotherapy in the management of circumscribed choroidal hemangioma. Surv Ophthalmol 2004;49:316-327.
34. Kiratli H. Ipsilateral orbital cavernous hemangioma and choroidal hemangioma. Eur J Ophthalmol 2002;12:547-549.
35. Lanning R, Shields JA. Comparison of radioactive phosphorus (32P) uptake test in comparable sized choroidal melanomas and hemangiomas. Am J Ophthalmol 1979;87:769-772.
36. Jarrett WH 2nd, Hagler WS, Larose JH, et al. Clinical experience with presumed hemangioma of the choroid: radioactive phosphorus uptake studies as an aid in differential diagnosis. Trans Sect Ophthalmol Am Acad Ophthalmol Otolaryngol 1976;81:862-870.
37. Aizman A, Finger PT, Shabto U, et al. Palladium 103 (103Pd) plaque radiation therapy for circumscribed choroidal hemangioma with retinal detachment. Arch Ophthalmol 2004;122:1652-1656.
38. Frau E, Rumen F, Noel G, et al. Low-dose proton beam therapy for circumscribed choroidal hemangiomas. Arch Ophthalmol 2004;122:1471-1475.
39. Scott IU, Gorscak J, Gass JD, et al. Anatomic and visual acuity outcomes following thermal laser photocoagulation or photodynamic therapy for symptomatic circumscribed choroidal hemangioma with associated serous retinal detachment. Ophthalmic Surg Lasers Imaging 2004;35:281-291.
40. Li H, Wen F, Wu D. Polypoidal choroidal vasculopathy in a patient with circumscribed choroidal hemangioma. Retina 2004;24:629-631.
41. Gunduz K. Transpupillary thermotherapy in the management of circumscribed choroidal hemangioma. Surv Ophthalmol 2004;49:316-327.
42. Kivela T, Tenhunen M, Joensuu T, et al. Stereotactic radiotherapy of symptomatic circumscribed choroidal hemangiomas. Ophthalmology 2003;110: 1977-1982.
43. Chao AN, Shields CL, Shields JA, et al. Plaque radiotherapy for choroidal hemangioma with total retinal detachment and iris neovascularization. Retina 2001;21:682-684.
44. Shields CL, Materin MA, Marr BP, et al. Resolution of advanced cystoid macular edema following photodynamic therapy of choroidal hemangioma. Ophthalmic Surg Lasers Imaging 2005;36:237-239.
45. Shields JA, Eagle RC Jr, Shields CL, et al. Total blindness from circumscribed choroidal hemangioma in a child. Am J Ophthalmol 2005;139: 1113-1114.
▪ Circumscribed Choroidal Hemangioma: Clinical Features
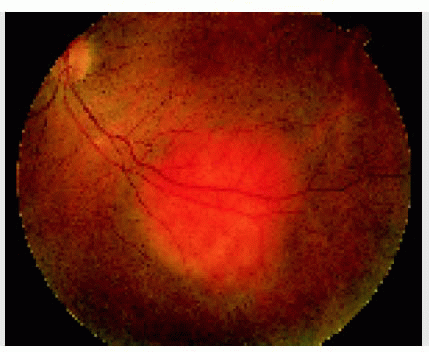
In most instances, the characteristic orange color of a circumscribed choroidal hemangioma strongly suggests the diagnosis.
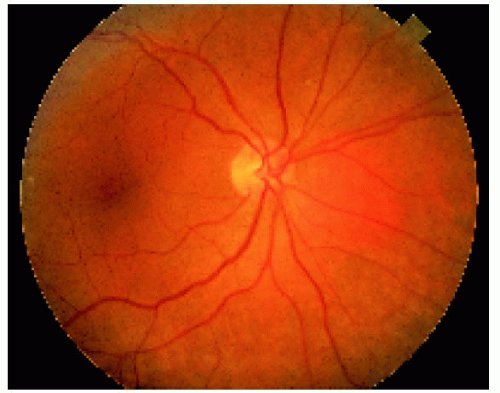 Figure 13.1. Subtle, asymptomatic choroidal hemangioma located nasal to the optic disc in a 69-year-old woman. Because it is the same color as the background fundus, it is often difficult to visualize in photographs, but it would appear elevated with binocular indirect ophthalmoscopy. |
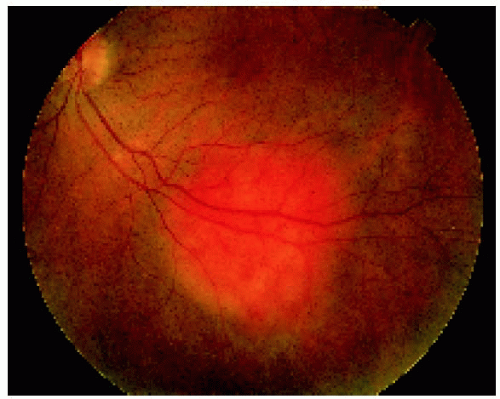 Figure 13.2. Choroidal hemangioma inferior to the fovea in a 47-year-old woman. |
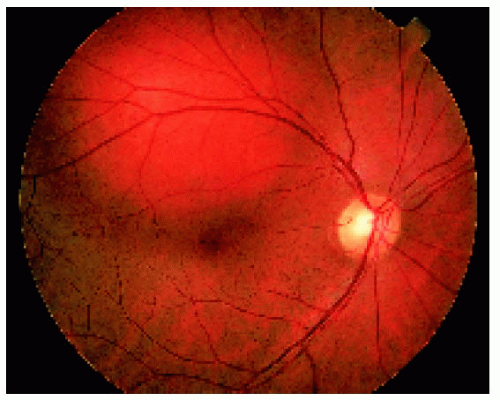 Figure 13.3. Choroidal hemangioma superior to the fovea in a 46-year-old man. |
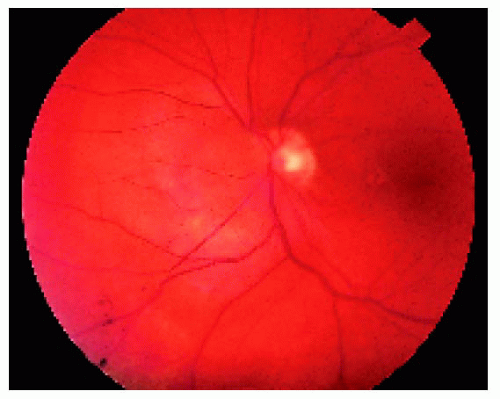 Figure 13.4. Choroidal hemangioma nasal to the optic disc and slightly overhanging the disc in a 39-year-old woman. |
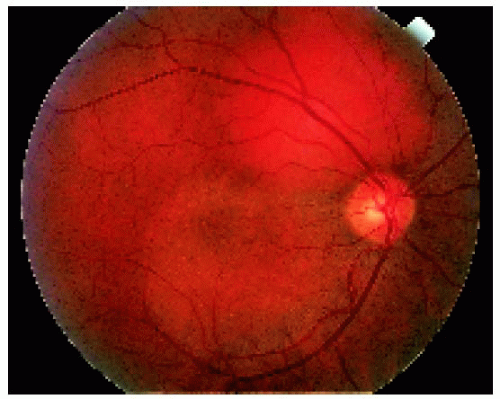 Figure 13.5. Choroidal hemangioma superior to the optic disc causing visual loss due to a secondary serous detachment of the retina extending into the foveal area. |
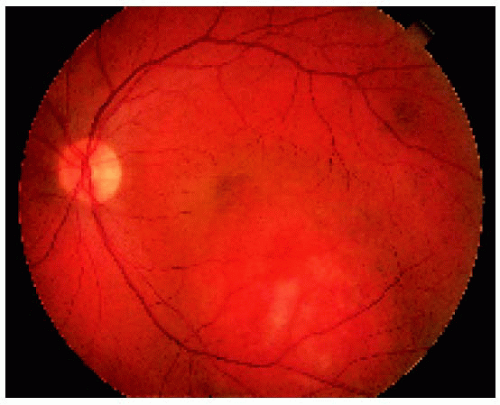 Figure 13.6. Choroidal hemangioma inferior to the fovea causing visual loss due to foveal elevation by the tumor. |
▪ Circumscribed Choroidal Hemangioma: Wide-Angle Imaging
 Figure 13.7. Choroidal hemangioma with shallow subretinal fluid superior to the optic disc in a 54-year-old woman. |
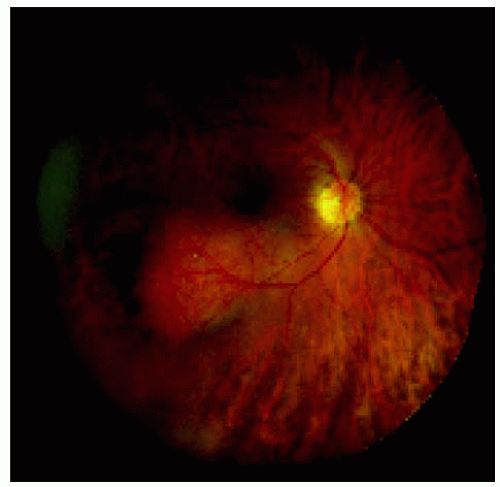 Figure 13.8. Choroidal hemangioma with shallow subretinal fluid inferotemporal to the fovea in a 71-year-old man. |
 Figure 13.9. Choroidal hemangioma superior to the optic disc in a 54-year-old woman. |
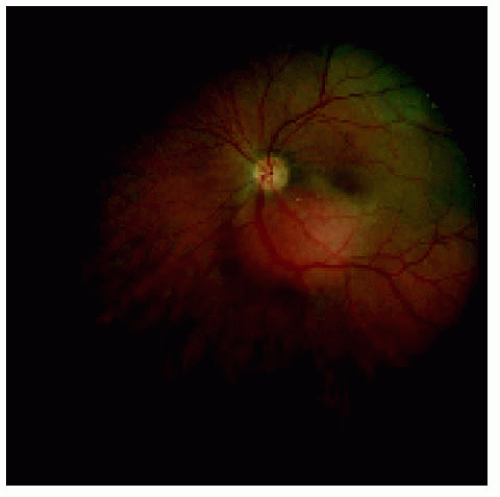 Figure 13.10. Choroidal hemangioma inferior to the disc and fovea in a 63-year-old woman. |
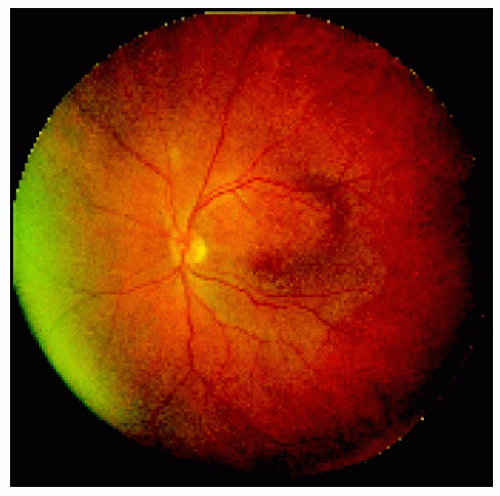 Figure 13.11. Choroidal hemangioma in the superior half of the macular area with evident secondary retinal detachment. |
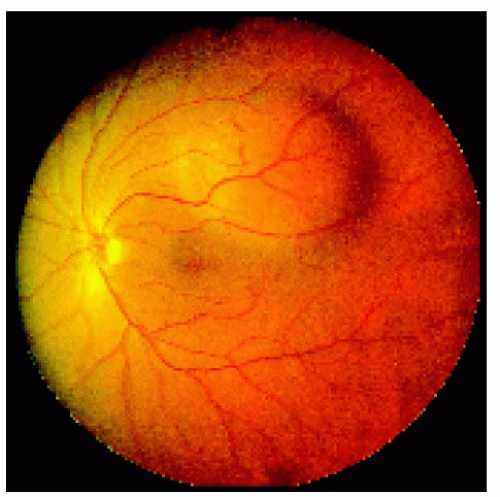 Figure 13.12. Slightly larger choroidal hemangioma superotemporal to the macular region in a 61-year-old man. |
▪ Circumscribed Choroidal Hemangioma: Effects on Adjacent Structures
In some instances, circumscribed choroidal hemangioma can cause secondary hyperplasia, fibrous metaplasia, or osseous metaplasia of the retinal pigment epithelium, as well as secondary retinal detachment and secondary retinoschisis.
 Figure 13.13. Focus of proliferation of the retinal pigment epithelium on the surface of a choroidal hemangioma superior to the optic disc in a 30-year-old woman. |
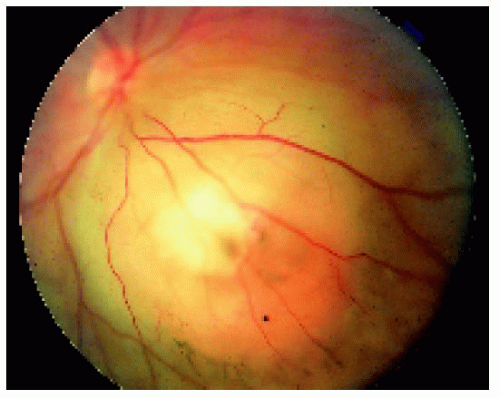 Figure 13.14. Subtle retinal pigment epithelium hyperplasia and fibrous metaplasia over a choroidal hemangioma in a 30-year-old woman. |
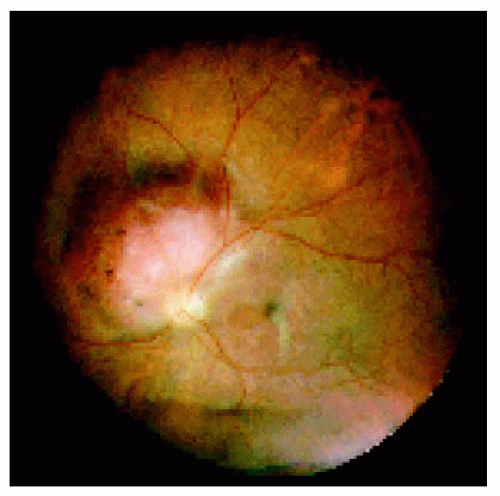 Figure 13.15. Extensive fibrous metaplasia and retinal pigment epithelium proliferation over and around a choroidal hemangioma in a 30-year-old man. There is retinoschisis over the dome of the tumor that is not well appreciated in a photograph without stereopsis. |
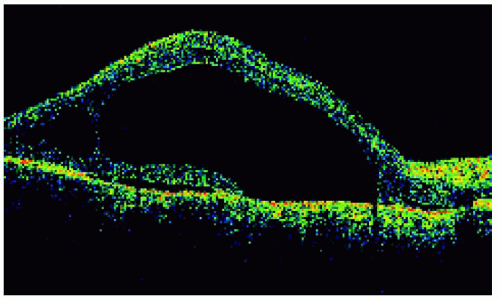 Figure 13.16. Optical coherence tomography of the lesion in Figure 13.15, showing the extensive retinoschisis and a shallow retinal detachment that was not appreciated clinically. |
 Figure 13.17. Retinal pigment epithelium (RPE) proliferation around and inferior to a choroidal hemangioma in a 71-year-old man. The RPE changes are typical of prior chronic localized retinal detachment. This tumor is somewhat larger and more anteriorly located than most choroidal hemangiomas. |
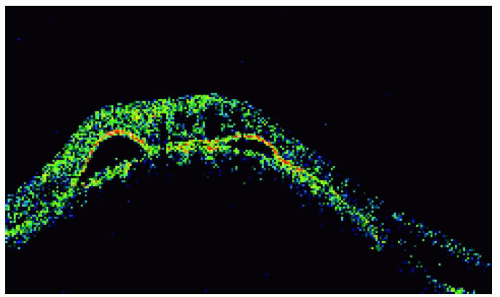 Figure 13.18. Optical coherence tomography of the lesion shown in Figure 13.17, demonstrating two focal detachments of the retinal pigment epithelium and chronic cystoid degeneration of retina, also attesting to the chronic nature of the lesion. |
▪ Circumscribed Choroidal Hemangioma: Fluorescein and Indocyanine Green Angiography
Although the findings are not pathognomonic, fluorescein angiography and indocyanine green angiography can often be helpful in differentiating a choroidal hemangioma from amelanotic melanoma, choroidal metastasis, and other nonpigmented fundus tumors.
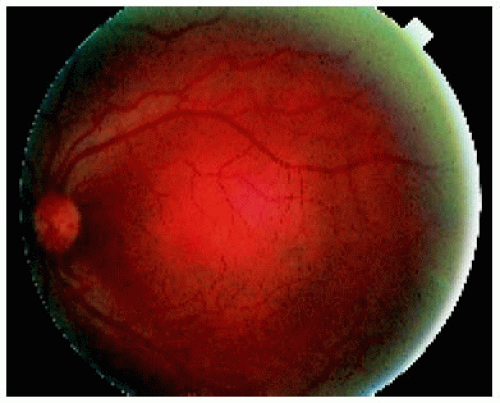 Figure 13.19. Choroidal hemangioma located in the central macular area. |
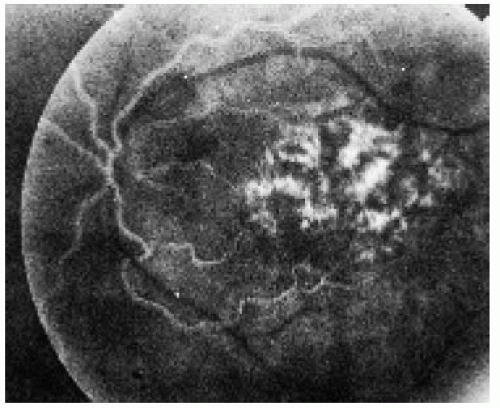 Figure 13.20. Standard fluorescein angiogram of lesion depicted in Figure 13.19 in the early arterial phase, showing reticular hyperfluorescence corresponding to the filling of choroidal vessels in the tumor. |
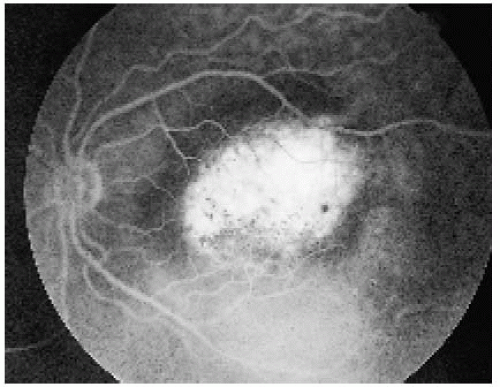 Figure 13.21. Recirculation phase of lesion shown in Figure 13.19 demonstrating marked hyperfluorescence of the lesion. |
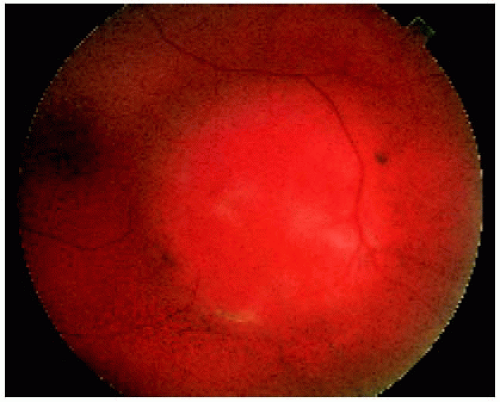 Figure 13.22. Choroidal hemangioma temporal to the foveal region in the left eye of a 39-year-old man. |
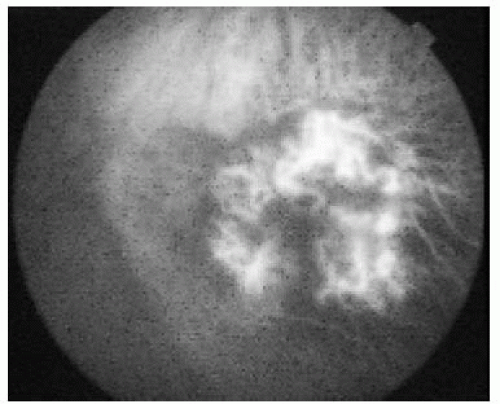 Figure 13.23. Early indocyanine green angiography of lesion shown in Figure 13.22 revealing reticular hyperfluorescence of the lesion. |
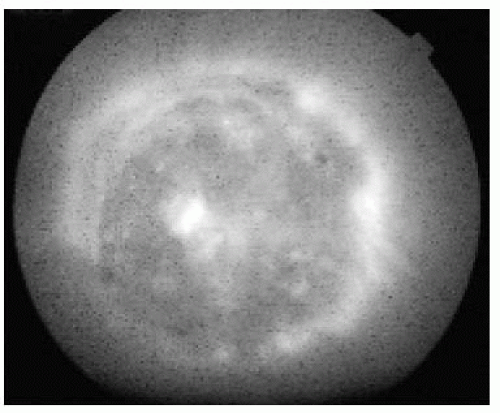 Figure 13.24. Late indocyanine green angiography of lesion shown in Figure 13.22 demonstrating the halo of hyperfluorescence and the central “wash out” phenomenon. |
▪ Circumscribed Choroidal Hemangioma: Ultrasonography
Ultrasonography of choroidal hemangioma generally shows high internal reflectivity with A-scan and acoustic solidity with B-scan. Fibrous or osseous metaplasia of the overlying pigment epithelium can produce a highly reflective echo that can sometimes confuse the diagnosis.
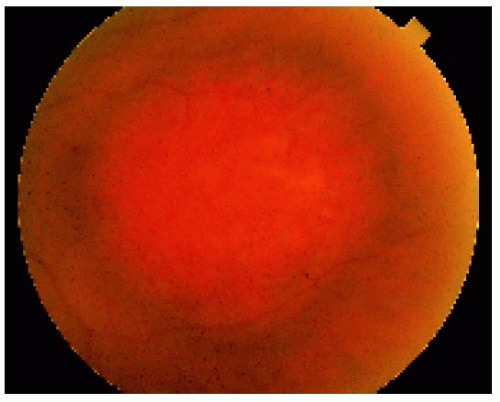 Figure 13.25. Clinical appearance of a tumor in the macular area in a 70-year-old woman. |
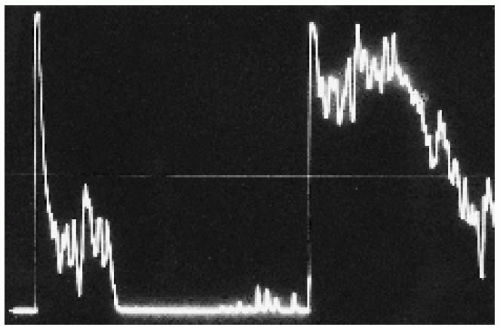 Figure 13.26. A-scan ultrasonogram, showing high initial spike and high internal reflectivity in the tumor. |
 Figure 13.27. B-scan ultrasonogram, showing acoustic solidity and lack of choroidal excavation. |
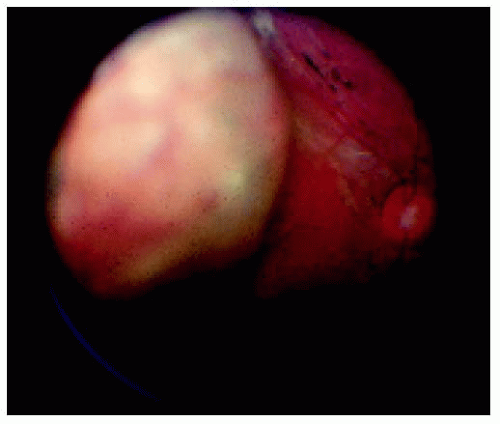 Figure 13.28. Large circumscribed choroidal hemangioma with severe overlying fibrous and/or osseous metaplasia of retinal pigment epithelium in a 9-year-old boy.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|