 Eyelid Inflammatory Lesions Simulating Neoplasms
Eyelid Inflammatory Lesions Simulating NeoplasmsEyelid Molluscum Contagiosum Infection
General Considerations
Molluscum contagiosum is an important cause of viral infection that can affect the eyelid (1,2,3,4,5,6,7,8,9,10,11,12,13). Historically seen almost exclusively in young children, it has recently been recognized with greater frequency in adults with acquired immunodeficiency syndrome (AIDS; 3). In children, transmission results from direct contact or fomites (1). In adults, it is generally a sexually transmitted disease. It is a cutaneous pox virus infection that can produce lesions on face, trunk, and proximal extremities (1).
Clinical Features
Molluscum contagiosum infection typically occurs as one or more discrete, flesh-colored lesions that range from 1 to 5 mm in diameter. Each lesion typically has an umbilicated center, sometimes simulating basal cell carcinoma. A cheesy detritus can usually be expressed from this central pore. A chronic follicular conjunctivitis can also occur as a result of shedding of virus particles into the conjunctival fornix. If untreated, this can lead to a corneal pannus and can simulate trachoma. Eyelid molluscum contagiosum can also cause an eczematous-appearing periorbital dermatitis (1,4,5,6,7). In patients with human immunodeficiency virus infection, the lesions tend to be larger and more aggressive (4,5,6,7). Severe bilateral eyelid involvement can occur in immunosuppressed children (8). Eyelid molluscum contagiosum infection can occasionally be the first signs of AIDS (7).
Pathology
Histopathologically, the typical lesion shows invasive acanthosis and degeneration of epithelial cells that fill the central cavity. Numerous intracytoplasmic inclusion bodies (Henderson-Patterson bodies) are present within the cavity (10).
Management
The most commonly employed treatment is incision and expression or curettage of the central core (13). When the lesion is located on the eyelid margin, it can be excised by shaving. Cryotherapy and laser treatment have been employed mostly for extraocular lesions. Hyperfocal cryotherapy with local anesthesia is reported to be a safer method for multiple eyelid lesions in AIDS patients (12). Topical trichloroacetic acid tretinoin (Retin-A), salicylic acid, and cantharidin have been used (13). Once the lesion is completely eliminated, recurrence is rare.
Selected References
1. Plotik RD, Brown M. Molluscum contagiosum and papillomas. In: Mannis MJ, Macsai MS, Huntley AC, eds. Eye and Skin Disease. Philadelphia: Lippincott Raven; 1996:489-494.
2. Vannas S, Lapinleimn K. Molluscum contagiosum in the skin caruncle, and conjunctiva. Acta Ophthalmol 1967;45:314-319.
3. Perez-Blazquez E, Villafruela I, Madero S. Eyelid molluscum contagiosum in patients with human immunodeficiency virus infection. Orbit 1999;18: 75-81.
4. Pelaez CA, Gurbindo MD, Cortes C, et al. Molluscum contagiosum, involving the upper eyelids, in a child infected with HIV-1. Pediatr AIDS HIV Infect 1996;7:43-46.
5. Biswas J, Therese L, Kumarasamy N, et al. Lid abscess with extensive molluscum contagiosum in a patient with acquired immunodeficiency syndrome. Indian J Ophthalmol 1997;45:234-236.
6. Chattopadhyay DN, Basak SK, Ghose S. HIV-positive patient presented with giant molluscum contagiosum of the eyelid. J Indian Med Assoc 1997;95: 202.
7. Leahey AB, Shane JJ, Listhaus A, et al. Molluscum contagiosum eyelid lesions as the initial manifestation of acquired immunodeficiency syndrome. Am J Ophthalmol 1997;124:240-241.
8. Katzman M, Emmets CA, Lederman MM. Molluscum contagiosum and the acquired immunodeficiency syndrome. Ann Intern Med 1985;102:413-414.
9. Charles NC, Friedberg DN. Epibulbar molluscum contagiosum in acquired immunodeficiency syndrome. Ophthalmology 1992;99:1123-1126.
10. Font RL. Eyelids and lacrimal drainage system. In: Spencer WH, ed. Ophthalmic Pathology. An Atlas and Textbook. 4th ed. Philadelphia: WB Saunders; 1996:2347.
11. Gonnering RS, Kronish JW. Treatment of periorbital molluscum contagiosum by incision and curettage. Ophthalmic Surg 1988;19:325-327.
12. Bardenstein DS, Elmets C. Hyperfocal cryotherapy of multiple molluscum contagiosum lesions in patients with the acquired immune deficiency syndrome. Ophthalmology 1995;102:1031-1034.
13. Habif TP. Warts, herpes simplex and other viral infections. In: Habif TP, ed. Clinical Dermatology. 2nd ed. St. Louis: CV Mosby; 1990:277-278.
Eyelid Molluscum Contagiosum Infection
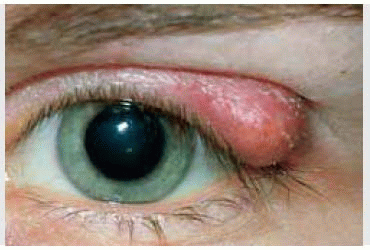
 Figure 12.1. Molluscum contagiosum infection with lesions involving upper and lower eyelids and the cheek. (Courtesy of Sprague Eustis, MD.) |
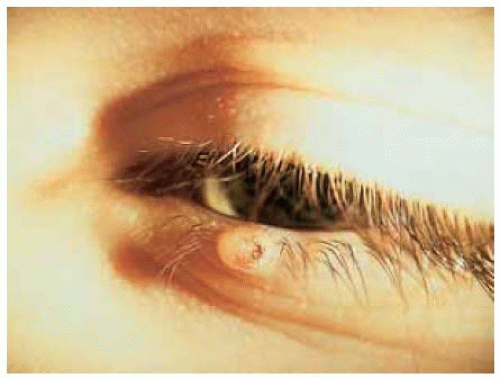 Figure 12.2. Closer view of left lower eyelid of the patient shown in Figure 12.1, revealing circumscribed papule with umbilicated center. (Courtesy of Sprague Eustis, MD.) |
 Figure 12.3. Multiple eyelid lesions of molluscum contagiosum in a 30-year-old man with AIDS. (Courtesy of Narsing Rao, MD.) |
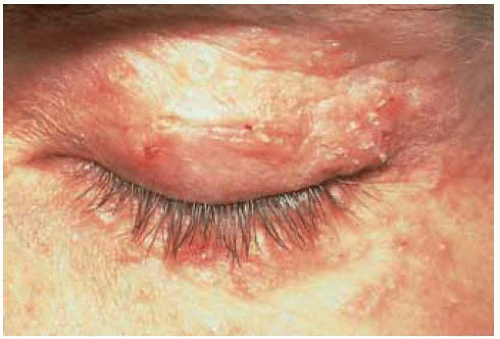 Figure 12.4 Eyelid involvement with molluscum contagiosum in a 34-year-old man with AIDS showing multifocal lesions. (Courtesy of Norman Charles, MD.) |
 Figure 12.5 Histopathology of molluscum contagiosum lesion showing acanthosis and central core containing necrotic epithelial cells and inclusion bodies. (Hematoxylin-eosin 5.) |
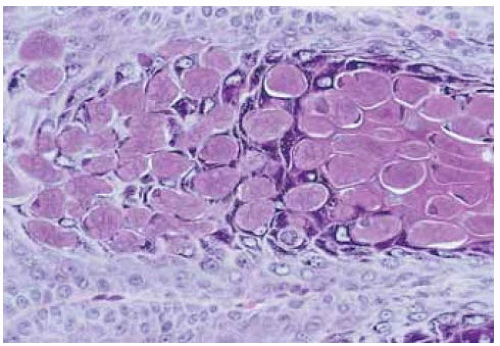 Figure 12.6. Higher magnification photomicrograph of the central core of the lesion shown in Figure 12.5, demonstrating typical intranuclear inclusion bodies (Henderson-Patterson bodies). (Hematoxylin-eosin 100.) |
Eyelid Chalazion
General Considerations
Clinical Features
Chalazion usually occurs secondary to noninfectious obstruction of the ducts of the aforementioned sebaceous glands (1,2). It usually first appears as a firm, tender, erythematous lump in the tarsal plate. As it progresses, it may break through posteriorly and appear on the palpebral conjunctiva or it may drain anteriorly through the skin. A ruptured chalazion can sometimes incite production of granulation tissue in the form of a pyogenic granuloma. In some instances, pressure on the globe by a chalazion can induce significant refractive errors (3,4,22). More aggressive chalazions have been observed in patients with hyperimmunoglobulinemia E (Job’s syndrome; 23,25), and tend to be more difficult to manage.
Chalazion generally has typical clinical features and the diagnosis can be made easily. It is reported that in 94% of cases the diagnosis is correctly made by the clinician. However, about 6% prove histopathologically to be other benign or malignant lesions (5); the most important is sebaceous carcinoma, but other malignant and benign eyelid conditions can closely mimic chalazion (5,6,7,8,9).
Pathology
Histopathologically, chalazion is characterized by a lipogranulomatous reaction to liberated lipid material. A connective tissue pseudocapsule is often present around the lesion. Round clear spaces in the lesion represent fat deposition. The granulomatous reaction with giant cells may be intermixed with acute and chronic inflammatory cells. Causative organisms are not usually identified, but secondary infection can occur, particularly in patients with Job’s syndrome. The granulomas may resemble those seen with sarcoidosis, cat scratch disease, or tuberculosis (2).
Management
Management is generally hot compresses and good eyelid hygiene. Symptomatic lesions that do not resolve can be managed by incision and curettage, with special effort to remove the pseudocapsule. A conjunctival approach using a chalazion clamp with the lid everted is generally preferred. An eyelid incision can be used for anterior lesions that are eroding through the skin (10,11). Several techniques for local anesthesia for chalazion treatment have been reported (12,13,14,15,16,17,18,19). If the lesion is typical of chalazion, intralesional injection of corticosteroids can be effective in bringing about resolution (10,15). However, such injections should be done with great care, because inadvertent corneal penetration and traumatic cataract have been rarely recognized as complications of corticosteroid injection (16).
As mentioned, some malignant neoplasms, particularly sebaceous carcinoma, can simulate a chalazion. Hence, any tissue should be sent for histopathologic studies to exclude the possibility of malignancy. The prognosis for chalazion is excellent.
Selected References
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


