 Orbital Fibrous Connective Tissue Tumors
Orbital Fibrous Connective Tissue TumorsOrbital Nodular Fasciitis and Fibroma
Orbital Nodular Fasciitis
General Considerations
Nodular fasciitis is a benign nodular proliferation of connective tissue that usually involves superficial fascia (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20). Konwaler and associates (2) originally called it “subcutaneous pseudosarcomatous fibromatosis.” It is now recognized to be a fairly common condition (1). Its occurrence in the orbital area was elucidated by Font and Zimmerman in 1966 (3) and subsequent reports have expanded on its ophthalmic manifestations (4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20). In the authors’ series of 1,264 orbital lesions, there were 2 cases, accounting for 15% of all fibrocytic lesions and for 1% of all orbital masses. It may be more common than indicated in that report because some cases are probably misdiagnosed histopathologically as other spindle cell lesions.
Clinical Features
Nodular fasciitis usually occurs in children and has a rather rapid onset and progression. It tends to occur in anterior periocular structures where it is visible or palpable and has rarely been observed in the deep orbit. It can simulate a dermoid cyst clinically (7).
Diagnostic Approaches
The diagnosis of nodular fasciitis can be suspected on the basis of clinical findings, but is usually made histopathologically after biopsy or surgical excision. With imaging studies, it shows features typical of other solid masses and has no distinctive findings.
Pathology
The histopathologic diagnosis of nodular fasciitis can be challenging, because it can simulate rhabdomyosarcoma or other soft tissue sarcomas (1,2,3). However, pathologists experienced with soft tissue tumors usually can make the diagnosis based on characteristic light microscopic features. Mitotically active stellate or spindle-shaped fibroblasts are often arranged in parallel bundles and extend in all directions, resembling cells in a tissue culture. Numerous newly formed parallel capillaries often ramify through the lesion, forming slitlike spaces reminiscent of those seen in Kaposi sarcoma. With immunohistochemistry, nodular fasciitis shows positive reactions against smooth muscle actin and vimentin. With electron microscopy, one sees parallel bundles of actinlike filaments with fusiform densities (17).
Management
Because nodular fasciitis usually is well circumscribed and located in the anterior adnexal structures, we recommend complete surgical removal when possible. Local recurrence is rare after complete excision.
Selected References
1. Weiss SW, Goldblum JR. Benign fibrous tissue tumors. Nodular fasciitis. In: Weiss SW, Goldblum JR. Enzinger and Weiss’s Soft Tissue Tumors. 4th ed. St. Louis: CV Mosby; 2001:50-56.
2. Konwaler BE, Keasbey, Kaplan L. Subcutaneous pseudosarcomatous fibromatosis (fasciitis). Am J Clin Pathol 1955;25:241-252.
3. Font RL, Zimmerman LE. Nodular fasciitis of the eye and adnexa. A report of ten cases. Arch Ophthalmol 1966;75;475-481.
4. Shields JA. Fibrous connective tissue tumors. In: Shields JA, ed. Diagnosis and Management of Orbital Tumors. Philadelphia: Saunders; 1989: 192-204.
5. Shields JA, Shields CL, Scartozzi R. Survey of 1264 patients with orbital tumors and simulating lesions: the 2002 Montgomery Lecture, part 1. Ophthalmology 2004;111:997-1008.
6. Perry RH, Ramani PS, McAllister SR, et al. Nodular fasciitis causing unilateral proptosis. Br J Ophthalmol 1975;59:404-408.
7. Shields JA, Shields CL, Christian C, et al. Orbital nodular fasciitis simulating a dermoid cyst in an 8-month-old child. Case report and review of the literature. Ophthal Plast Reconstr Surg 2001;17:144-148.
8. Levitt JM, deVeer A, Oguzhan C. Orbital nodular fasciitis. Arch Ophthalmol 1969;81:235-237.
9. Reccia FM, Buckley EG, Townshend LM, et al. Nodular fasciitis of the orbital rim in a pediatric patient. J Pediatr Ophthalmol Strabismus 1997;34: 316-318.
10. Hymas D , Mamalis N, Pratt DV, et al. Nodular fasciitis of the lower eyelid in a pediatric patient. Ophthal Plast Reconstr Surg 1999;15:139-142.
11. Tolls RE, Mohr S, Spencer WH. Benign nodular fasciitis originating in Tenon’s capsule. Arch Ophthalmol 1966;75:482-483.
12. Levitt JM, deVeer JA, Ogushan C. Orbital nodular fasciitis. Arch Ophthalmol 1969;81:235- 237.
13. Meacham CT. Pseudosarcomatous fasciitis. Am J Ophthalmol 1974;77: 747-749.
14. Ferry AP, Sherman SE. Nodular fasciitis of the conjunctiva apparently originating in the fascia bulbi (Tenon’s capsule). Am J Ophthalmol 1974;78: 514-517.
15. Holds FB, Mamalis N, Anderson RL. Nodular fasciitis presenting as rapidly enlarging episcleral mass in a 3-year-old. J Pediatr Ophthalmol Strabismus 1990;27:157-160.
16. Vestal KP, Bauer TW, Berlin AJ. Nodular fasciitis presenting as an eyelid mass. Ophthalmol Plast Reconstr Surg 1990;6:130-132.
17. Sakamoto T, Ishibashi T, Ohnishi Y, et al. Immunohistologic and electron microscopical study of nodular fasciitis of the orbit. Br J Ophthalmol 1991;75:636-638.
18. Kew YT, Cuesta RA. Nodular fasciitis of the orbit diagnosed by fine needle aspiration cytology. A case report. Acta Cytologica 1993;37:957-960.
19. Meffert JJ, Kennard CD, Davis TL, et al. Intradermal nodular fasciitis presenting as an eyelid mass. Int J Dermatol 1996;35:548-552.
20. Graham BS, Barrett TL, Goltz RW. Nodular fasciitis: response to intralesional corticosteroids. J Am Acad Dermatol 1999;40:490-492.
Orbital Fibroma
General Considerations
Among the benign fibrous proliferations, fibroma is a difficult lesion to categorize (1). It is possible that reported cases of orbital fibroma would be reclassified today as solitary fibrous tumor (SFT), fibrous histiocytoma, or other spindle cell lesions (1,2). Nevertheless, we have retained it in this edition because of prior publications (4,5,6,7). It appears to be a benign neoplasm or reactive process that may arise from Tenon’s fascia or its precursors. It has been reported in the orbital region (3,4,5,6,7,8).
Clinical Features
Fibroma in the orbital area usually appears as a palpable firm mass in the anterior orbit that produces proptosis or globe displacement. It can extend anteriorly into the conjunctiva and appear as an irregular, yellow-white mass.
Diagnostic Approaches
There is little specific information on the diagnosis of orbital fibroma. Clinically and with imaging studies, it probably appears as a solid, anterior, yellow-white mass with irregular borders.
Pathology
Fibroma is composed of a paucicellular population of fibroblasts that are sometimes widely separated by abundant collagen. The long, graceful fascicles typical of fibroma and other pure fibroblastic tumors appear different on light microscopy from the twisting storiform pattern of the cells of fibrous histiocytoma. The absence of foci of inflammation is helpful in differentiating fibroma from sclerosing idiopathic orbital inflammation, in which inflammatory cells can usually be detected despite large areas of fibrosis.
Management
The diagnosis of orbital fibroma is not usually made clinically; as with most primary circumscribed orbital soft tissue tumors, the best management is complete surgical removal. Incomplete surgical removal can lead to recurrence. The approach to surgery is determined by the size and location of the tumor on orbital computed tomography (CT). Orbital fibromas are probably not radiosensitive, although it seems reasonable to attempt radiotherapy in recurrent or unresectable cases that show progression and complications.
Selected References
1. Weiss SW, Goldblum JR. Benign fibrous tissue tumors. Nodular fasciitis. In: Weiss SW, Goldblum JR. Enzinger and Weiss’s Soft Tissue Tumors. 4th ed. St. Louis: CV Mosby; 2001:250-256.
2. Shields JA. Fibrous connective tissue tumors. In: Shields JA, ed. Diagnosis and Management of Orbital Tumors. Philadelphia: Saunders; 1989: 192-204.
3. Mortada AK. Fibroma of the orbit. Br J Ophthalmol 1971;55:350-352.
4. Stokes WH, Bowers WF. Pure fibroma of the orbit. Report of a case and review of the literature. Arch Ophthalmol 1934;11:279-282.
5. Howcroft MJ, Hurwitz JJ. Lacrimal sac fibroma. Can J Ophthalmol 1980;15: 196-197.
6. Herschorn BJ, Jakobiec FA, Hornblass A, et al. Epibulbar subconjunctival fibroma. A tumor possibly arising from Tenon’s capsule. Ophthalmology 1983; 90:1490-1494.
7. Fowler JG, Terplan KL. Fibroma of the orbit. Arch Ophthalmol 1942;28: 263-271.
8. Case TD, La Piana FG. Benign fibrous tumor of the orbit. Ann Ophthalmol 1975;7:813-815.
Orbital Nodular Fasciitis
Orbital nodular fasciitis usually occurs in young children as a subcutaneous mass. It can sometimes simulate a dermoid cyst.
Shields JA, Shields CL, Christian C, et al. Orbital nodular fasciitis simulating a dermoid cyst in an 8-month-old child. Case report and review of the literature. Ophthal Plast Reconstr Surg 2001;17:144-148.
 Figure 32.1. Nodular fasciitis in a young boy presenting as a subcutaneous mass beneath lateral aspect of right upper eyelid, resembling a dermoid cyst. |
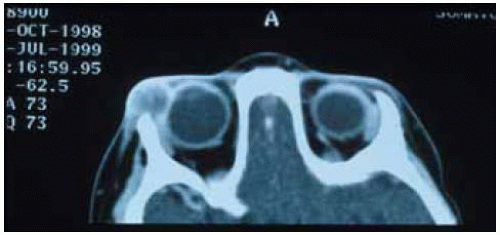 Figure 32.2. Axial computed tomography showing a round mass near superotemporal orbital rim. |
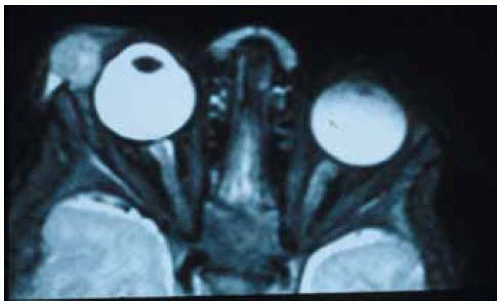 Figure 32.3. Magnetic resonance im aging on T2-weighted im age showing the mass with solid internal appearance. It is slightly hyperintense to vitreous on T2. |
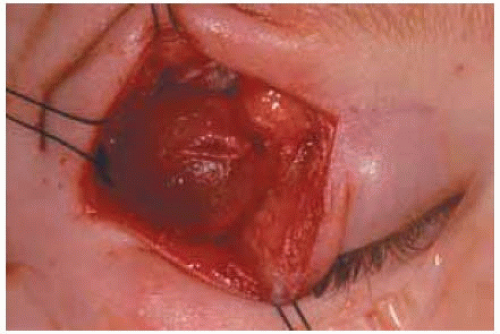 Figure 32.4. Appearance of reddish firm mass exposed at time of surgery by a superotemporal eyelid crease approach. |
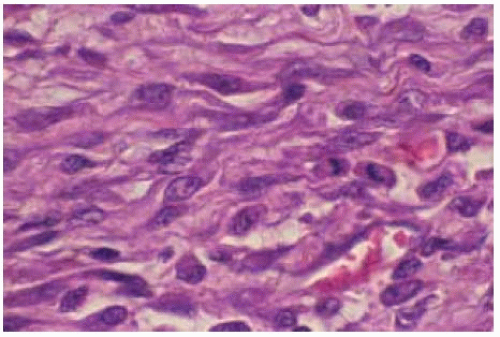 Figure 32.5. Photom icrograph of same lesion showing spindle cells with prominent nucleoli. A mitotic figure is present to the right. On initial diagnostic frozen sections, rhabdomyosarcoma or other malignant spindle cell tumor could not be excluded. However, permanent section were interpreted as nodular fasciitis by expert soft tissue pathologists. (Hematoxylin-eosin 200.) |
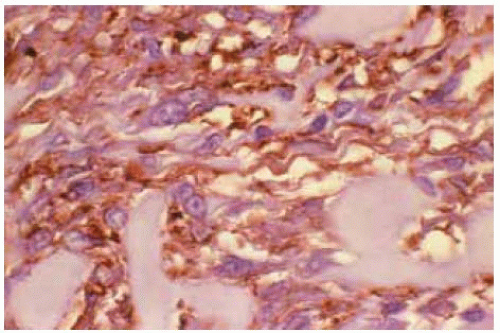 Figure 32.6. Immunohistochem istry shows positive reaction to vim entin. Immunohistochem istry also showed positive reaction for smooth muscle actin. These results supported the diagnosis of nodular fasciitis. ( 200.) |
Orbital Nodular Fasciitis and Fibroma
 Figure 32.7. Orbital nodular fasciitis presenting as a subcutaneous mass behind lower eyelid in a 2-year-old girl. (Courtesy of Mark Ost, M D.) |
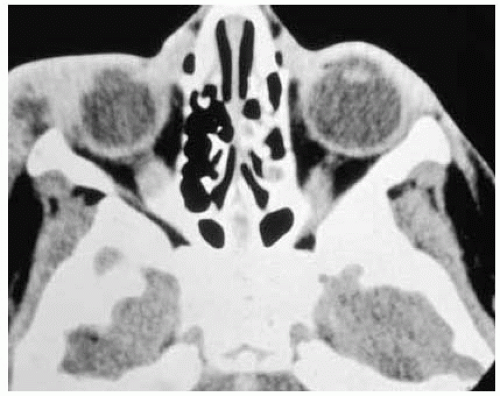 Figure 32.8. Axial computed tomography of the patient shown in Figure 32.7 demonstrating the tumor in the inferotemporal aspect of the orbit and subcutaneous tissue. (Courtesy of Mark Ost, MD.) |
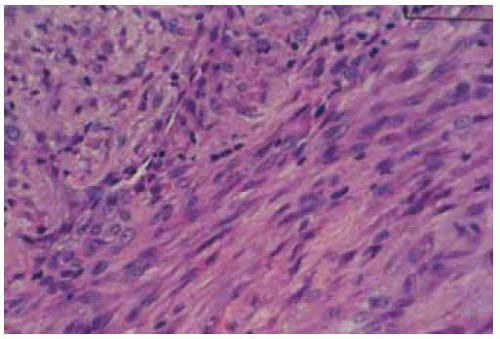 Figure 32.9. Histopathology of nodular fasciitis demonstrating sheets of proliferating fibroblasts and chronic inflammatory cells. (Hematoxylin-eosin 150.) |
 Figure 32.10. Fibroma of superior orbit and subcutaneous tissue in a 49-year-old woman. It was noticed 1 year earlier and had not shown appreciable change. (Courtesy of Mourad Khalil, MD.) |
 Figure 32.11. Same lesion shown in Figure 32.10 with eyelid elevated. Note the smooth, circumscribed appearance of the lesion. (Courtesy of Mourad Khalil, MD.) |
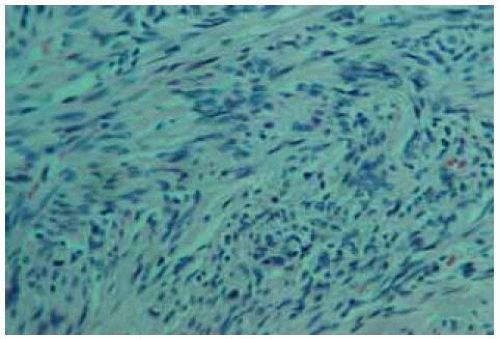 Figure 32.12. Histopathology of lesion shown in Figure 32.11 demonstrating closely packed fibrocytes consistent with fibrom a. (Hematoxylin-eosin 150.) (Courtesy of Mourad Khalil, MD.) |
Orbital Fibromatosis, Myofibromatosis, and Myofibroma
General Considerations
The fibromatoses (myofibromatoses) are nonencapsulated, nonmetastasizing fibrous tumors that have several clinical variations (1,2,3,4,5,6,7,8,9,10,11,12,13,14). The terminology regarding these entities is confusing because they overlap clinically and histopathologically. Evidence of smooth muscle elements in some lesions is justification for the term “myofibromatosis,” and we use the terms interchangeably herein because they are closely related. The fibromatoses appear to represent intermediate lesions between the localized fibromas and the more malignant fibrosarcomas. They can occur at any age and can be a part of generalized fibromatosis or they can be solitary (myofibroma). Orbital involvement has received increasing attention in the literature (4,5,6,7,8,9,10,11,12,13,14).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


