(1)
Department of Ophthalmology, St. Thomas’ Hospital, London, UK
16.1 Introduction
16.2.1 Vitreous Opacification
16.2.2 Retinal Detachment
16.2.3 Cystoid Macular Oedema
16.2.4 Hypotony
16.2.5 The Vitreous Biopsy
16.3.1 Clinical Features
16.3.2 Surgery
16.3.3 Visual Outcome
16.4.1 Clinical Features
16.4.2 Surgery
16.4.3 Visual Outcome
16.5.1 Clinical Features
16.5.2 Surgery
16.5.3 Visual Outcome
16.6 Other Infections
16.6.1 Clinical Features
16.6.2 Surgery
16.6.3 Visual Outcome and Survival
16.8 Summary
Abstract
This is a broad and varied group of conditions which have commonality in clinical presentation and features. They often provide a diagnositic challenge with shared investigative methods.
Electronic supplementary material
The online version of this chapter (doi:10.1007/978-3-642-31872-6_16) contains supplementary material, which is available to authorized users.
16.1 Introduction
This is a broad and varied group of conditions which have commonality in clinical presentation and features. They often provide a diagnositic challenge with shared investigative methods.
16.2 Non-infectious Uveitis of the Posterior Segment

Fig. 16.1
Use the slit lamp beam to detect cells in the vitreous in inflammatory conditions. Check for cells in any odd presentation of macular ERM or retinal detachment in case there is an underlying inflammatory cause
The variety of possible presentations of uveitis of the posterior segment makes it difficult to generalise on the surgical approach (Mieler et al. 1988; Eckardt and Bacskulin 1992; Nolle and Eckardt 1993). The conditions that the surgeon may encounter, depending on the racial mix and geographical location, include:


Intermediate uveitis
Sarcoidosis
Uveitis of juvenile chronic arthritis
Behcet’s disease
Idiopathic vasculitis including Eales’ disease
Birdshot chorioretinopathy
Vogt–Koyanagi–Harada syndrome
Sympathetic uveitis
Takayasu’s arteritis
Fig. 16.2
Indentation reveals snow banking in this patient with intermediate uveitis
Fig. 16.3
Sarcoidosis is a very common cause of posterior uveitis
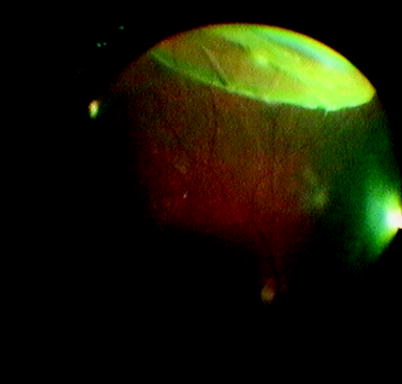
Fig. 16.4
This composite picture shows a pattern of Eales’ disease. These patients can produce neovascularisation and vitreous haemorrhage
Fig. 16.5
This patient with idiopathic uveitis has subretinal exudation and epiretinal membranes
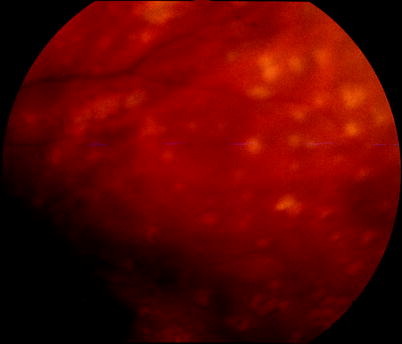
Fig. 16.6
Sympathetic uveitis is a rare cause characterised by white retinal spots, sometimes attributed to the pathological feature of Dalen–Fuch’s nodules
In the Western population, the commonest presentations are likely to be intermediate uveitis, sarcoidosis and juvenile chronic arthritis. Although often relatively controllable with systemic therapy, those patients with more severe disease may require vitreoretinal intervention for the following reasons:

Fig. 16.7
A patient with exudative RD from Vogt–Koyanagi–Harada syndrome
Diagnostic confirmation
Vitreous opacification
Rhegmatogenous retinal detachment (RRD)
Tractional retinal detachment (TRD)
Exudative retinal detachment
Cystoid macular oedema (CMO)
Epiretinal membrane
Hypotony
Fig. 16.8
(a, b) In patients with uveitis, vitreous with debris and cells can be adherent to the posterior lens surface obscuring the view for the surgery. With careful aspiration with the vitreous cutter, the vitreous can be teased off of the posterior lens without damaging the posterior capsule
The vitreous may become opaque because of the presence of cellular deposits, proteinaceous infiltration and degeneration of the gel structure. The inflammatory process can cause shrinkage of the gel which in the presence of vitreoretinal adhesion may produce either TRD or RRD (Mieler et al. 1988; Bovey and Herbort 2000; Heiligenhaus et al. 1994). In patients with intermediate uveitis, cystoid macular oedema may account for between 40 and 60 % of eyes with poor vision (Scott et al. 2003; Dugel et al. 1992). Ultimately phthisis bulbi from hypotony is the most severe end point from these inflammatory conditions (Kokame et al. 2001). It causes a catastrophic visual loss and even a cosmetically unacceptable eye, often in young patients.
16.2.1 Vitreous Opacification
Removal of the vitreous cells and debris in the vitreous gel may restore vision in patients with uveitis of the posterior segment (Eckardt and Bacskulin 1992; Mieler and Aaberg 1992; Heimann et al. 1992; Kaplan 1992; Diamond and Kaplan 1979). Intermediate uveitis may be complicated by vitreous haemorrhage that can be treated successfully by vitrectomy (Potter et al. 2001). Many of these patients are young and have attached PHM, which will require removal, but the PHM may be difficult to detach because of vitreoretinal adhesions. Postoperatively the eye may produce inflammation requiring systemic immunosuppressive cover over the peroperative period. Visual recovery is often limited because of the presence of optic atrophy or retinal damage particularly from CMO (Verbraeken 1996; Waters et al. 2000). Some surgeons claim that removal of the gel reduces the ability of the eye to hold inflammatory mediators and thereby reduces recurrence of inflammation in the long term. Evidence for this remains uncertain (Bovey and Herbort 2000). Others argue that improvement following surgery is a result of the removal of vitreous opacity rather than any influence on the inflammatory process (Mieler et al. 1988). Also reduction in medical treatment after surgery has been blamed for a rebound of inflammation 3–6 months later. Therefore, PPV is not recommended routinely in these patients but is reserved for the treatment of the vitreoretinal complications.
Retinal vasculitis can produce ischaemia and a neovascular response associated with vitreous haemorrhage. PPV can be used to relieve traction to prevent recurrent haemorrhage and clear the visual axis. Unlike diabetic retinopathy, panretinal photocoagulation is not universally required.

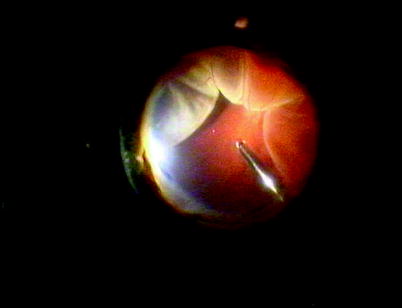
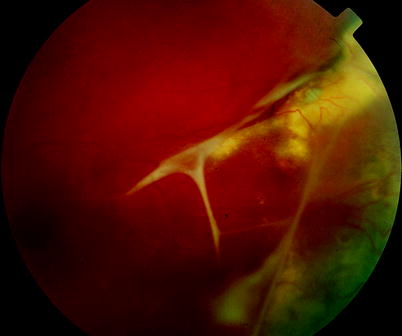
Fig. 16.9
In this patient with uveitis, a secondary epiretinal membrane has formed and has been removed during vitrectomy
Fig. 16.10
In a patient with suspected exudative retinal detachment, heavy liquids can be inserted onto the posterior pole and gradually expanded. If there are no retinal breaks, there is route for escape of subretinal fluid, and the retina will bulge forwards anteriorly in bullae around the top of the heavy liquids. If a retinal break is present, then sclera may be identified and the subretinal fluid will spontaneously leave the subretinal space and the retinal detachment will resolve
16.2.2 Retinal Detachment
When TRD is associated with neovascularisation or fibrosis, delamination and dissection of the membranes are required. A vitreoschisis, as seen in diabetic retinopathy (Chap. 9), may be present and must be recognised to allow appropriate dissection under the plane of the PHM to aid delamination. Unfortunately TRDs are often associated with severe subretinal exudation in uveitic eyes, and visual recovery is often poor.
Rarely patients present with TRD without neovascularisation or preretinal fibrosis; a smooth elevation of the retina is seen. PPV and peeling of the PHM will suffice, allowing the retina to settle without need to drain SRF.
RRD may occur from PVD formation and can be dealt with by routine means (see Chap. 6) whilst being aware of the possibility of exacerbation of the uveitis.
Exudative RD may be encountered and diagnosed by shifting fluid and the absence of retinal tears, traction and epiretinal fibrosis (despite a long-standing duration of retinal detachment) (Gaun et al. 2002). Beware that the patient does not have uveal effusion syndrome. If immunosuppressive therapy does not reattach the retina, PPV a retinotomy to drain the SRF or an external drainage may help. During the surgery, the exudative nature of the retinal detachment can be confirmed by inserting heavy liquids onto the posterior retina. This will displace SRF anteriorly where it is trapped (because there is no retinal hole to allow drainage) and forms a tight ring bulla which overhangs the heavy liquid. Removal of the heavy liquid reveals a return of the retinal detachment to its previous configuration, confirming no loss of SRF. Perform a small and peripheral retinotomy to drain SRF and laser the retinotomy. Alternatively bend a needle as for an external drain (see DACE procedure, Chap. 6) whilst viewing the retina internally via PPV and indent the sclera gently with the ‘heel’ of the bend in the needle to locate its position. Locate the needle into an area of high SRF (fill the posterior pole with heavy liquid to create a ring bulla), then rotate the needle to insert the point through the scleral and choroid to commence drainage. With small-gauge surgery, the needle can be inserted through the conjunctiva. Fill with long-acting gas or silicone oil. If the uveitis is then controlled, return of the retinal detachment is unlikely.
16.2.3 Cystoid Macular Oedema
Steroid injections into the vitreous cavity can reverse CMO in uveitis. However, the chronic nature of these conditions causes a return of the CMO after the steroid has been cleared from the eye (Antcliffe et al. 2001). Slow-release steroid implants or injections may overcome this difficulty and are now available. For example, slow-release dexamethasone pellets can be injected as an outpatient procedure; they have an effect for 3–6 months similar to intravitreal triamcinolone but appear to have less chance of an IOP rise (Haller et al. 2010a, b). PPV has been performed to try to relieve traction on the macula to resolve cystoid macular oedema (Dugel et al. 1992; Verbraeken 1996; Aylward 1999) because the vitreous is more often attached than not in patients with CMO (Davis et al. 1992). Others have examined the severity of cystoid macular oedema and found both improvement (Heiligenhaus et al. 1994; Tranos et al. 2006) and persistence of the complication following vitrectomy (Diamond and Kaplan 1978; Priem et al. 1993). Separating the response to vitrectomy from the natural history of the condition and from the effects of concomitant therapies is difficult because randomised studies have not been done.
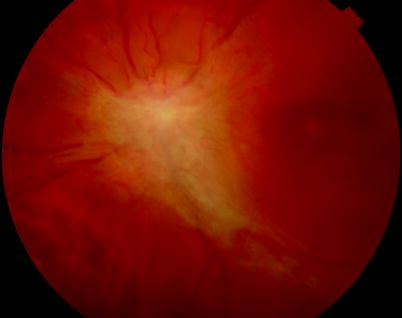
Fig. 16.11
A papillitis has stimulated an ERM which is wrinkling the fovea
16.2.4 Hypotony
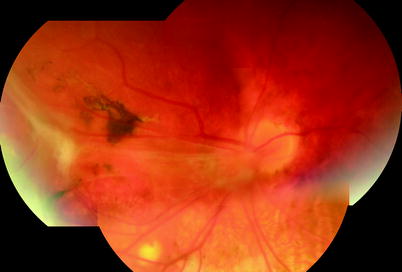
Fig. 16.12
A fold through the macula in a patient with severe panuveitis. The risk of putting the eye into hypotony must be considered before operating on any eye with panuveitis
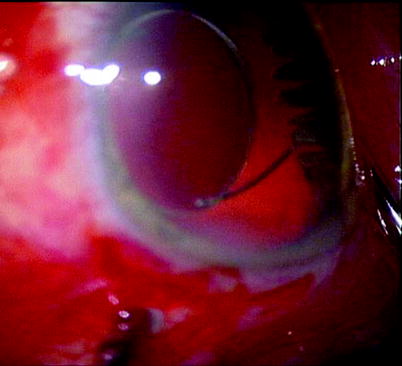
Fig. 16.13
A normal ciliary body
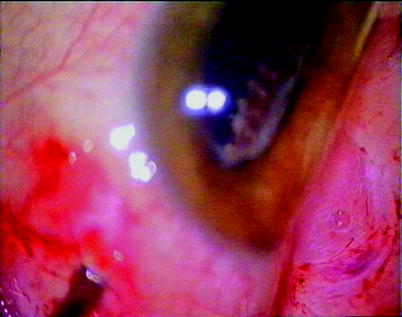
Fig. 16.14
White caps on the ciliary processes from uveitis
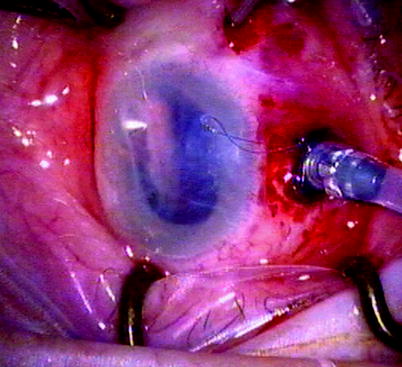
Fig. 16.15
Complete absence of ciliary processes in hypotony from uveitis
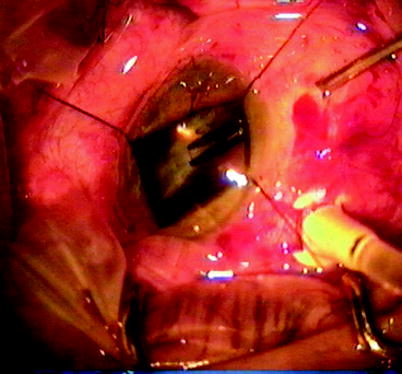
Fig. 16.16
Ciliary body membrane formation
Hypotony occurs in these eyes because the ciliary body becomes involved in the uveitic process.
Causes of ciliary body failure:
Traction
Atrophy
Detachment
Fig. 16.17
The folds in the posterior layers of the eye are a precursor to phthisis in this patient with panuveitis. The surgeon may choose to fill the eye with silicone oil to retain a cosmetically acceptable globe size and shape and vision of low grade
Vitrectomy has been used to try and relieve traction on the ciliary body in hypotony (Kaplan 1992). Inspection of the ciliary body with dissection of any tractional membranes has been performed only in a few patients and is as yet of uncertain worth especially as often the ciliary processes are atrophic and may be non-functional. Insertion of hyaluronic to provide a temporary IOP rise has been employed. Silicone oil can be used for a more prolonged effect and to prevent severe shrinkage of the size of the eye if hypotony persists (Morse and McCuen 1991). Long-term results of these interventions are unknown.
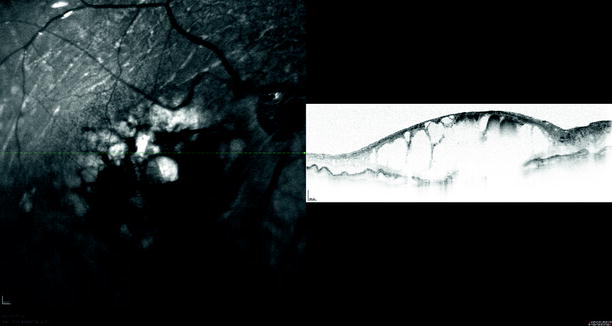
Fig. 16.18
A hypotonous eye is likely to have CMO
Drug | Mode of action | Typical adult maintenance dosage | Severe systemic complications |
|---|---|---|---|
Prednisolone | Corticosteroid | 1–15 mg | Peptic ulceration |
Myopathy | |||
Osteoporosis | |||
Adrenal | |||
suppression | |||
Cushing’s syndrome | |||
Azathioprine | Antiproliferative | 1–3 mg/kg daily | Myelosuppression |
Especially those with low thiopurine methyltransferase activity | |||
Mycophenolate mofetil | Antiproliferative | 1 g twice daily | Leucopenia |
Opportunistic infections | |||
Methotrexate | Antimetabolite (inhibits dihydrofolate reductase) | 7.5 mg weekly | Myelosuppression |
Mucositis | |||
Pneumonitis 7.5 | |||
Ciclosporin | Calcineurin inhibitor | 5 mg/kg daily | Nephrotoxicity |
Tacrolimus | Calcineurin inhibitor | Neurotoxicity | |
Cardiomyopathy | |||
Infliximab | Tumour necrosis factor activity inhibition | 3 mg/kg every 2 months by IV infusion | Infections |
Heart failure | |||
Hypersensitivity | |||
Blood disorders | |||
Rituximab | Tumour necrosis factor activity inhibition | 1 g every 2 weeks by IV infusion | Infections |
Heart failure | |||
Hypersensitivity | |||
Blood disorders | |||
Etanercept | Tumour necrosis factor activity inhibition | 25 mg twice weekly by subcutaneous injection | Infections |
Heart failure | |||
Hypersensitivity | |||
Blood disorders |
Diagnostic Confirmation
Uveitic syndromes may occasionally be difficult to discriminate from other causes of posterior infiltration such as infection and neoplasm. Polyclonal white cells are seen on cytology with a CD4/CD8 ratio of at least 4 (Davis et al. 2005). A significant number of patients with uveitis do not have a definitive diagnosis. Only 66 % of cases of anterior uveitis are associated with clinical and laboratory abnormalities which lead to a definitive diagnosis increasing to 85 % in posterior uveitis (Priem et al. 1993). Laboratory examination of the vitreous is particularly indicated when unusual or non-characteristic presentations occur.
Biopsy of the vitreous by needle aspiration may be effective in postoperative endophthalmitis (Han et al. 1999) where the vitreous is liquefied by the infection but may not be appropriate in non-infectious uveitis. Use of a vitreous cutter is recommended because of the greater incidence of vitreoretinal adhesion in uveitic patients increasing the risk of retinal detachment or tear (Verbraeken 1996). Many of these patients are young and likely to have non-syneretic vitreous gel increasing the likelihood of a ‘dry tap’ with a needle. In some cases, vitrectomy is the ideal; in addition to providing a vitreous sample, vitrectomy may allow visualisation of the fundus, allowing characteristic features of the disease process to be recognised and hence revealing a supplementary diagnosis.
16.2.5 The Vitreous Biopsy
Use transconjunctival 23 or 25 gauge if possible inserted at 4 mm from the corneal scleral limbus; if not available, create the usual 20-gauge sclerotomy opening inferotemporally (see Chap. 2).
A table of immunosuppressive agents that can be used in the treatment of uveitis.
Insert the cutter and visualise in the eye.
Maintain the IOP with a squint hook providing scleral indentation whilst employing the cutter to extract the vitreous to beyond the three-way tap (inserted on the first junction of the aspiration tubing), providing approximately 0.5 ml of vitreous.
Remove the cutter and reinflate the eye with any intravitreal drug administration, for example, antibiotics, whilst relieving the pressure on the squint hook.
Sew up the sclerotomy and conjunctiva if 20 gauge.
Remove the sample from the tubing to send to the laboratory. Take an anterior chamber sample via a paracentesis as required.
16.2.6 Sampling at the Beginning of a PPV
If a small sample is required at the beginning of a PPV, the sample needs to be ‘dry’, that is, not diluted with the infusion fluid; therefore,
Insert the infusion cannula, but do not switch it on.
Create a superior sclerotomy and remove the vitreous whilst applying pressure with the squint hook.
Remove the cutter and extract the sample.
Switch on the infusion and release the pressure with the squint hook.
Continue the PPV.
At the end of the PPV after closing one sclerotomy and with the infusion switched off, insert any intravitreal injections, close the other sclerotomy and then remove the infusion cannula.
Special Situations
If a large sample (2 ml) is required, infuse the eye with heavy liquids which will fall to the back of the eye maintaining its IOP whilst allowing removal of the vitreous and a dry tap (Quiroz-Mercado et al. 2005).
For some conditions (e.g. Candida and bacterial endophthalmitis for culturing or lymphoma for cytometry), it is worth sending the ‘washings’, vitreous diluted with infusion fluid in the vitrectomy equipment aspiration cassette, to the laboratory.
Note: If you are inserting gas or silicone oil and you want to use intravitreal drugs, insert the drugs into the vitreous cavity just before inserting the tamponade agent. This ensures that the drugs are of the correct dosage (diluted in 4 ml of fluid in the vitreous cavity). The concentration will remain the same in the thin layer of remaining fluid after fluid/oil or fluid/gas exchange.
Table 16.1
Adult drug dosages (these are guidelines only, the administration of the medications can vary in different institutions)
Disorder | Drug | Dosage | Route of administration |
|---|---|---|---|
Candida endophthalmitis | Amphotericin B | 0.005 mg in 0.1 ml | Intravitreal |
Fluconazole | 200–400 mg/day for 3 weeks | Oral | |
Flucytosine (often combined with Fluconazole to avoid resistance) | 50–150 mg/kg/day divided doses (reduce in renal impairment) | Intravenous infusion | |
Voriconazole | 400 mg b.d. loading dose, 200 mg b.d. | Oral | |
CMV retinitis | Gancyclovir | 1.5–2.0 mg/0.1 ml | Intravitreal |
HSV and VZV acute retinal necrosis (treatment in the acute phase) | Foscarnet | 2.4 mg/0.1 ml | Intravitreal |
Aciclovir | 10 mg/kg t.d.s for 10 days, monitor renal function | Intravenous infusion | |
Valaciclovir | 1 g t.d.s. for 10 days | Oral | |
HSV and VZV acute retinal necrosis (prevention of infection in the fellow eye) | Valaciclovir | 300 mg t.d.s. for 3 months | Oral |
Bacterial endophthalmitis | Vancomycin | 2 mg/0.2 ml | Intravitreal |
Ceftazidime (used in combination) | 2 mg/0.2 ml | ||
Intraocular inflammation or cystoid macular oedema | Triamcinolone | 2 mg/0.05 ml | Intravitreal |
Triamcinolone | 40 mg | Subtenons | |
Lymphoma | Methotrexate | 0.4 mg/0.16 ml | Intravitreal |
Toxoplasmosis chorioretinitis | Pyrimethamine | 100 mg stat., then 25 mg b.d. for 3 weeks | Oral |
Sulfadiazine | 1 g b.d. for 3 weeks | ||
Folinic acid | 15 mg 2× weekly | ||
Prednisolone (used in combination) | 60 mg tapering,10 mg every 5 days | ||
Clindamycin | 300 mg q.d.s. for 3 weeks | Oral | |
Peroperative prophylaxis | Vancomycin | 10 mg/2 ml (1 g in 20 ml water = 50 mg in ml, take 1 ml dilute in 9-ml water) | Infusion bottle |
Inject 2 ml |
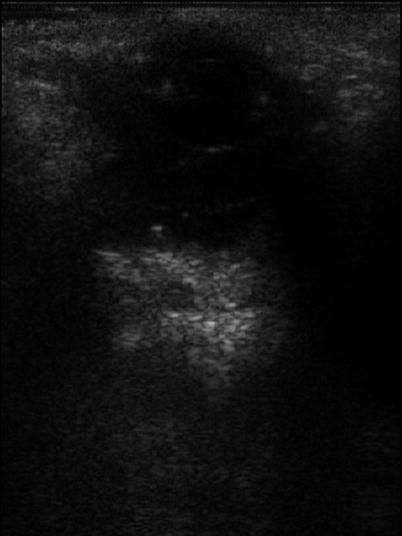
Fig. 16.19
An ultrasound of a patient with panuveitis with an intraocular pellet of slow-release steroid
16.3 Acute Retinal Necrosis
16.3.1 Clinical Features
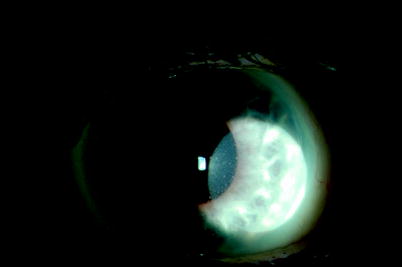
Fig. 16.20
Small ‘spidery’ keratotic precipitates are often associated with virus-associated uveitis. In this patient, cytomegalovirus was detected on PCR analysis of an aqueous sample

Fig. 16.21
The advancing edge of acute retinal necrosis is visible in this patient. Retinal detachments are extremely common in this condition
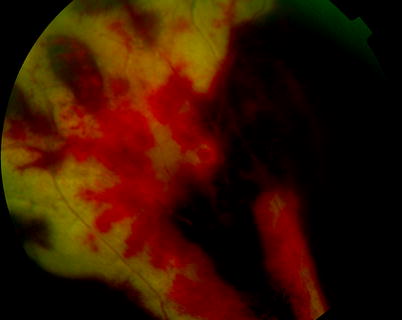
Fig. 16.22
Acute retinal necrosis is characterised by peripheral white lesions with a crenated edge advancing centrally sometimes with retinal haemorrhaging
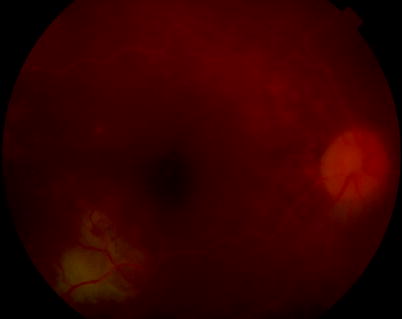
Fig. 16.23
When the infection reaches the optic nerve, the vision drops severely
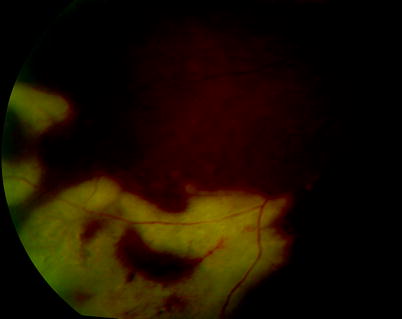
Fig. 16.24
ARN after commencement of steroid therapy
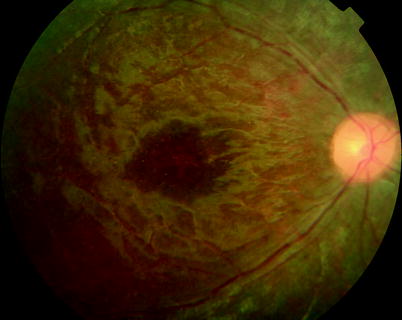
Fig. 16.25
A 5-year-old boy developed an atypical acute retinal necrosis without retinal infiltration but with retinal vasculitis in both eyes a few months after chicken pox. Vision was perception of light in both eyes
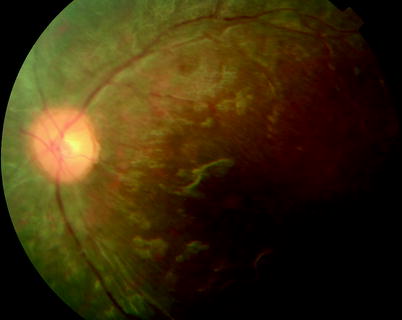
Fig. 16.26
See previous figure
Viral infections of the retina cause a mixed arteritic and infiltrative retinitis. The causative viruses are commonly of the herpes simplex family (Akpek et al. 1999a).
These patients may have a history of cold sores.
Herpes zoster is commoner in the elderly (Freeman et al. 1986; Bali et al. 2003; Zambarakji et al. 2002) and can be associated with herpes zoster ophthalmicus (Nakanishi et al. 2000) and chicken pox (Culbertson et al. 1991).
Herpes simplex 2 infections can also occur especially in children (Rahhal et al. 1996; Markomichelakis et al. 2001; Rappaport and Tang 2000).
Epstein–Barr virus can rarely be detected but is often considered to be a coincidental finding (Hershberger et al. 2003).
Patients are generally not immunocompromised, but herpes zoster is implicated in both ARN (Hershberger et al. 2003; Weinberg and Lyon 1997) and progressive outer retinal necrosis in AIDS patients (Purdy et al. 2003; Austin 2000; Moorthy et al. 1997; Perez-Blazquez et al. 1997; Pavesio et al. 1995; Margolis et al. 1991) and the immunocompromised.
There is a significant risk of bilateral disease (Ezra et al. 1995; Martinez et al. 1992) with fellow eye involvement even years later (Matsuo et al. 1987) and a long-term risk of encephalitis (Ahmadieh et al. 1991; Bloom et al. 1977).
The retina has the appearance of peripheral haemorrhage and infiltration, which spread posteriorly to involve the macula, but the presentation has variable severity (Bloom et al. 1977). The retina may become moth eaten, and retinal detachment is common up to 50 % (Carney et al. 1986). In severe presentations, exudative retinal detachment can occur (Duker et al. 1990). Patients have been described with giant retinal tears (Topilow et al. 1982), retinal neovascularisation (Wang et al. 1983) and peripheral retinal pigment epithelial tears (Fox and Blumenkranz 1993). Proliferative vitreoretinopathy is common.
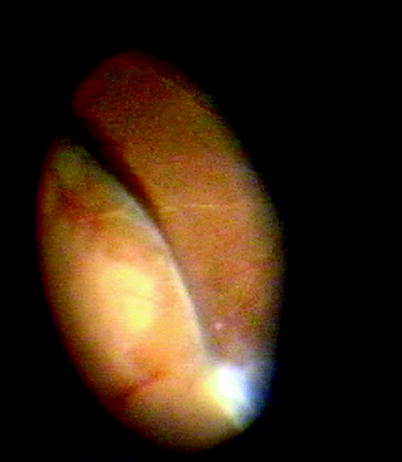

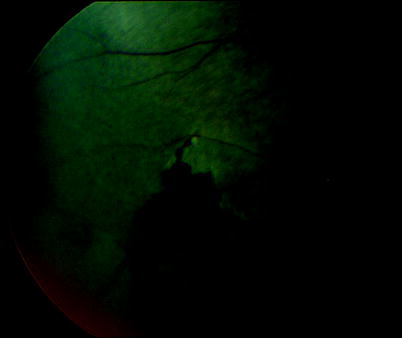
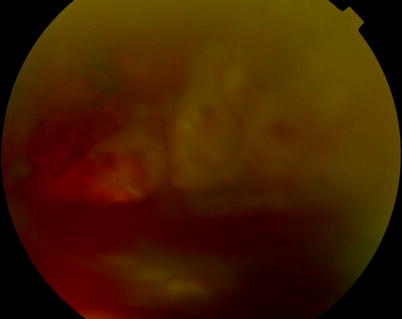
Fig. 16.27
A discrete-edged large retinal break is seen on indentation in this patient with acute retinal necrosis
Fig. 16.28
In this patient, a retinal detachment has followed after acute retinal necrosis. Sometimes discrete tears are identifiable, but often the retina is ‘moth eaten’, and the exact location of breaks is difficult
Fig. 16.29
Progressive outer retinal necrosis occurs in the immunocompromised individuals with herpes simplex or zoster infection of the retina. Retinal tears and detachment are common
16.3.2 Surgery
Table 16.2
Difficulty rating for surgery for ARN
Difficulty rating | High |
Success rates | Low |
Complication rates | Moderate |
When to use in training | Late |
For Diagnosis
The clinical pattern can be useful in diagnosis, but vitreous biopsy is mandatory. A vitreous sample of 0.2 ml is usually sufficient to allow the detection of the virus on polymerase chain reaction (PCR) with a high yield of positive results of 60–80 % (Gerling et al. 1992; Verbraeken and Libert 1995).
For Treatment
Systemic antiviral therapy is given over a period of months to try to prevent involvement of the second eye and encephalitis. Intravitreal antiviral, for example, foscarnet, can be inserted during biopsy (Perez-Blazquez et al. 1997; Immonen et al. 1989).
Management of retinal detachment requires PPV, gas, laser and buckle depending on the situation (Immonen et al. 1989; McDonald et al. 1991; Blumenkranz et al. 1988, 1989). Insertion of silicone oil is often necessary because a causative single break is frequently difficult to identify; large areas of the retina are thinned and damaged, and proliferative retinopathy is common (Ahmadieh et al. 2003). Retinal attachment after multiple procedures is common (90 %) and visual recovery is poor (McDonald et al. 1991).
16.3.3 Visual Outcome
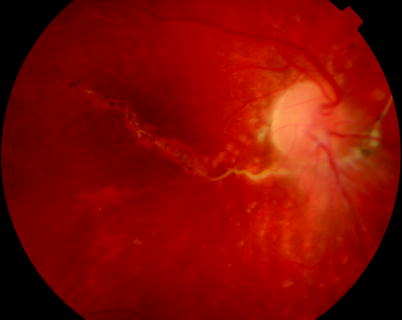
Fig. 16.30
This teenager suffered RRD after ARN; his retina is shown 4 years after the surgical repair reattached without silicone oil in situ with evidence of damage and a subretinal fibrous band
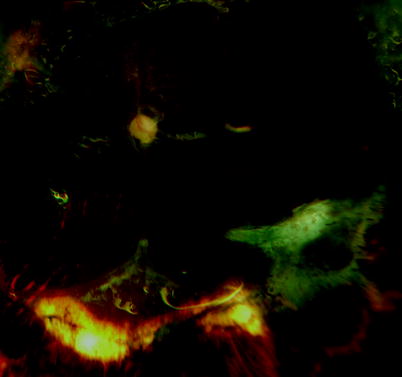
Fig. 16.31
Progressive outer retinal necrosis is shown postoperatively with oil in situ to retain a reattached retina with hand movement vision
The prognosis for vision is poor in the affected eye; therefore, systemic therapy is essential to prevent involvement of the other eye.

Fig. 16.32
Despite reattachment of the retina in this patient with ARN, there is CMO of the macula
16.4 Cytomegalovirus Retinitis
16.4.1 Clinical Features
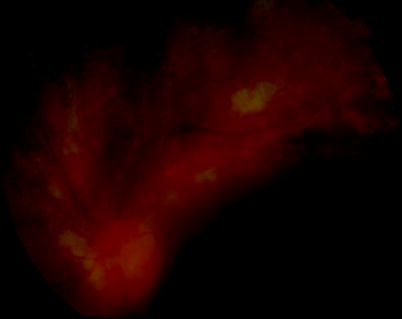
Fig. 16.33
CMV retinitis has become less common since the commencement of HAART therapy but may still be seen in immunocompromised individuals
Cytomegalovirus (CMV) infects the retina in immunocompromised patients. Overwhelmingly these patients suffer from AIDS. Prior to highly active antiretroviral therapy (HAART) (Jabs 1995), 40 % of AIDS patients developed CMV retinitis. Others requiring systemic immunosuppression such as Wegener’s granulomatosis or rheumatoid arthritis are occasionally present (Akpek et al. 1999a; Fraenkel et al. 1995). Classically in AIDS, the patient has a severe reduction in CD4 white blood cells to less than 50 cells/μl. With the introduction of HAART, control of viral load is much improved, and consequently CD4 counts are more often preserved. This has led to a massive reduction in the numbers of new cases of retinitis which may only occur when there is failure of or resistance to HAART (Uphold et al. 1998; Mitchell et al. 1999; Mocroft et al. 2000; Jalali et al. 2000). Retinal detachment was a common complication of the retinitis before HAART (50 % at 1 year after development of retinitis (Jabs 1995; Jabs et al. 1991)), usually slow in onset because of the presence of a formed and attached vitreous gel in these young patients, and bilateral in 70 % (Sidikaro et al. 1991). Prior to HAART, this was linked to early mortality at approximately 6 months (Dugel et al. 1991; Irvine et al. 1997). Since HAART, patients with CMV retinitis have shown 81 % reduction in mortality (Kempen et al. 2003) and 60 % reduction in retinal detachment (Kempen et al. 2001), but most with CMV retinitis will develop a condition called immune recovery uveitis which can reduce vision (Holbrook et al. 2003; Arevalo et al. 2003; Song et al. 2003). This is characterised by posterior segment inflammation which causes secondary complications such as cystoid macular oedema (Irvine et al. 1997), vitreomacular traction (Canzano et al. 1998), vitreous haemorrhage from retinal neovascularisation (Wright et al. 2003), and even activation of previously quiescent infections of the retina such as mycobacteria (Zamir et al. 2002).
Note: Immune recovery uveitis is usually self-limiting causing only mild visual loss.
Increasingly, the control of the viral load is most important to the control of the retinitis by allowing cessation of anti-CMV therapy as the CD4 count recovers (Wright et al. 2003).
16.4.2 Surgery
Table 16.3
Difficulty rating for surgery for CMV retinitis
Difficulty rating | Moderate |
Success rates | Moderate |
Complication rates
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|