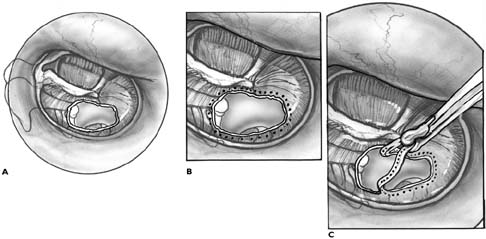
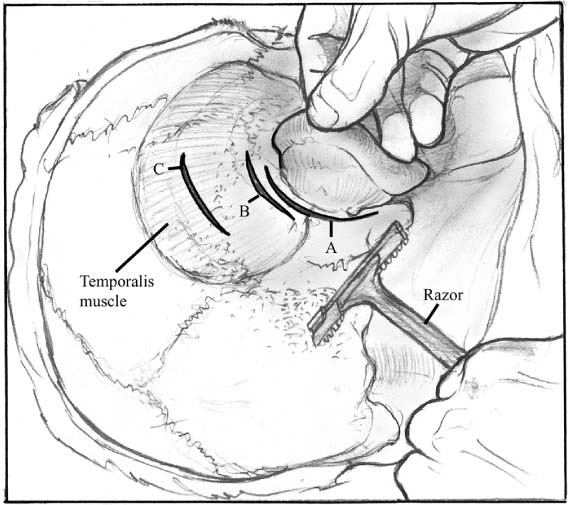
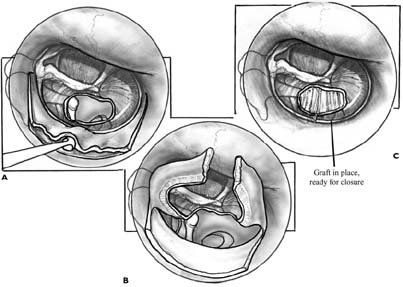
Chapter 3 The current era of tympanoplasty began in 1952 with Wullstein and Zollner.1 Shea,2,3 Hough,4 Storrs,5 Herrmann,6 Austin,2,7,8 Sheehy,9,10 Glasscock,11,12 Tos,13–15 and others have since made important contributions. Today tympanoplasty is a highly developed set of techniques. Most tympanic membrane perforations can be closed with underlay or overlay techniques regardless of location or size.11,16–18 This chapter presents the technique of tympanic membrane repair with underlay grafting. In the underlay technique the graft material is placed medial to the tympanic membrane remnant and medial to the manubrium of the malleus. Other strategies and techniques for grafting are described elsewhere in this book. The overall goals of treatment of chronic otitis media in order of priority are (1) to make the ear safe; (2) to make the ear clean, dry, comfortable, and relatively free of maintenance; and (3) to restore hearing. Otologists pursue these goals with medical and surgical treatment. Tympanoplasty is defined as a procedure to remove disease from the middle ear and to reconstruct with or without tympanic membrane grafting. Tympanic membrane grafting is a component of tympanoplasty when the disease involves the tympanic membrane; for example, in cases of perforation or atelectasis. Tympanoplasty often includes reconstruction of the ossicular chain for hearing. Sometimes mastoidectomy is also performed either to remove disease or to provide exposure through a posterior tympanotomy approach. A careful evaluation of diseased ears is necessary for planning treatment. Important points of history include the patient’s age, history of prior otologic surgery, general health, and the frequency and character of drainage, pain, hearing loss, and vestibular symptoms. It is important to understand what symptoms are most bothersome and most important to the patient. The physical examination should include an examination of the tympanic membranes and the outer ears for incisional scars from previous otologic surgery. The nasopharynx should be examined, if possible, for evidence of potential causes of eustachian tube dysfunction. The size and location of the perforation or retraction of the tympanic membrane, the presence of middle ear polyps, cholesteatoma, tumors, masses, atelectasis, tympanosclerosis, and erosion of the ossicular chain should be noted. In appropriate instances, high-resolution computed tomography of the temporal bones or microbial cultures should be considered.19,20 Audiometric testing is indicated. We have not found routine tests of eustachian tube function to be useful guides to therapy. Patients should be evaluated holistically, with due consideration given to the status of the opposite ear and the ability to maintain middle ear aeration, and to estimate the long-term prospects for helping with the patient’s needs and goals. In some cases, medical treatment and debridement will be needed to control active infection prior to consideration for surgical repair. The assessment guides the treatment recommendations and counseling. The elective nature of most cases of tympanoplasty should be kept in mind. Surgery in the only hearing ear should be reserved for dangerous ear conditions, such as progressive cholesteatoma, and should be carried out by experienced surgeons.15,21 The normal tympanic membrane has a complex layered structure consisting of thin stratified squamous epithelium on the lateral surface, flat respiratory epithelium on the medial surface, and two fibrous layers, one radial and one longitudinal, between the two epithelial layers. The fibrous layers also contain vascular elements. Successful, functional repair of the tympanic membrane requires reconstitution of the epithelial layers and enough of a fibrous middle layer to provide satisfactory mechanical support. When a tympanic membrane heals spontaneously without grafting, the perforation is often closed by the squamous epithelium before fibrous elements develop. The fibrous layer may be attenuated or even lacking. The resultant tympanic membrane has an area that lacks the tensile strength, elasticity, blood supply, and resistance to future perforation of a fully reconstructed tympanic membrane. Such areas are referred to as “dimeric” because the squamous epithelium lies against the mucous membrane without intermediate fibrous elements. The healing process after grafting appears to be initiated by angiogenesis within the tympanic membrane remnant, especially at the margin of the perforation. During healing the fascia is a scaffold for epithelialization. The margins of the freshened edges of the perforation (see below) are the sources for the migrating epithelia. Fascia is composed of fibroblasts in a collagen matrix. Its low metabolic rate and its extracellular matrix permit it to persist until it becomes vascularized. A critical problem early in the development of tympanoplasty was finding a suitable material for tympanic membrane grafting. Since the 1950s, sev-eral tissues have been proposed for donor graft materials, including split-thickness skin, full-thickness skin, vein, allograft tympanic membranes, and prepared collagen materials. This chapter describes the use of temporalis fascia, which is now the most widely used material.5,6 Temporalis fascia results in rapid, reliable healing of an appropriately thin tympanic membrane. It can be obtained from the same operative field, often from the same incision used for access to the ear (Fig. 3–1). Epidermal growth factors have been used to enhance healing experimentally.22 Medial grafting techniques take advantage of the ability of respiratory epithelium (unlike squamous epithelium) to incorporate the graft material when the graft is placed against it. The squamous and respiratory epithelial layers and the fibrous layer are in contact with the rest of the tympanic membrane after healing.23,24 A graft of temporalis fascia is harvested early in the procedure to allow time for the graft to dry (Fig. 3–1). Any muscle tissue adherent to the fascia is removed. We prefer to use the true temporalis fascia, rather than the areolar fascia. The areolar fascia has more of a trabecular structure, which occasionally results in the formation of small perforations. These small perforations sometimes appear months after primary healing. The transcanal approach is appropriate for small posterior perforations where the entire margin can be seen through the ear canal (Fig. 3–2). Either local anesthesia (adults) or general anesthesia can be used. After sterile preparation and draping of the ear, local anesthetic with epinephrine is injected to supplement the general anesthetic and aid in hemostasis. The graft is harvested and allowed to dry on a smooth, hard surface. The size of the fascial graft depends on the size of the perforation. The trimmed perforation should overlap the graft by at least 1 mm, and preferably by 2 mm or more, in all directions. Once harvested, the fascia is allowed to dry on a block of dense fluoroplastic. Tympanic membrane perforations are fistulas between the ear canal and the middle ear space. They are stable because contact inhibition between the squamous epithelium of the lateral surface of the tympanic membrane and the mucous membrane of the medial surface prevents active growth of either epithelium. Consequently, it is necessary to disrupt the junction between the squamous and respiratory epithelia.23 The authors prefer to accomplish this step by removing a 1-mm rim of the perforation circumferentially (Fig. 3–2). This step is sometimes referred to as “freshening” the edges of the perforation. Plaques of tympanosclerosis are patches of hyalinized (calcified) scar that replace portions of the fibrous layers of the tympanic membrane following periods of inflammation from chronic otitis media. They probably interfere with healing by blocking vascularization of the graft. Tympanosclerosis can be removed from the medial surface of the tympanic membrane with an angled pick. It is also useful to score the medial surface of the tympanic membrane remnant to stimulate the respiratory epithelium to incorporate the graft. FIGURE 3–1 Temporalis fascia may be har-vested from the same postauricular incision used for exposure to the middle ear (incision A). If a transcanal approach is used, a smaller incision over the fascia may be used to obtain the graft (incision B). If fascia has already been harvested during a previous operation, it may be necessary to harvest fascia from a more superior position using a supplemental incision (incision C). Use of incision C requires shaving and sterile preparation of a larger area before starting the operation. It is important to be aware of the location of the temporalis muscle, because the true temporalis fascia makes a more suitable graft material than areolar fascia or the periosteum of the skull. A simple myringoplasty can be accomplished for small perforations without a tympanomeatal flap. In most cases, however, a tympanomeatal flap is raised to provide exposure to remove disease, reconstruct the ossicular chain, or facilitate placement of the graft. The flap should be planned to expose at least the posterior half of the middle ear space. The flap should be folded anteriorly at the manubrium. Thus, incisions are made laterally from the annulus at the 6 and 12 o’clock positions, and directed posteriorly. The inferior incision may be placed more anteriorly if more anterior exposure is needed. Three canal incisions are made to create the medially based flap (Fig. 3–3A). The two radial incisions are made first. Then they are connected by a third incision placed laterally. The flap should be long enough to accommodate curettage of the posterior scutum if needed for exposure. To avoid troublesome bleeding, the flap should not be extended more than necessary into the thicker poster-osuperior canal skin (the “vascular strip”). Also, a large flap can obstruct exposure to the middle ear. In general the flap should extend two thirds of the distance from the annulus to the bony cartilaginous junction of the external auditory canal, or about 7 mm from the annulus (Fig. 3–3A). FIGURE 3–2 The transcanal approach is suitable for repair of a small posterior tympanic membrane perforation (A). A series of full-thickness punctures is made 1 mm from the edge of the perforation circumferentially using a sharp curved needle (B). The margin of the perforation is then stripped off using a cup forceps (C). FIGURE 3–3
UNDERLAY TYMPANOPLASTY
DEFINITIONS
EVALUATION
CONSIDERATIONS IN GRAFT HEALING
TECHNIQUE
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


