Chapter 22 Congenital aural atresia is thought to occur in 1 in 10,000 to 20,000 live births, with unilateral atresia being three times more common than bilateral atresia.1–3 It occurs more often in males, and more often on the right side.1 Although external ear and middle ear malformations often occur in combination, due to their similar embryologic origin from the first and second branchial structures, inner ear malformations are a less common association, owing to its derivation from the auditory placode and otic capsule. Surgery for canal atresia is one of the most complex surgeries performed by otologists, drawing on the techniques of canaloplasty, meatoplasty, tympanoplasty, and ossiculoplasty. A thorough understanding is required of the normal as well as variant surgical anatomy of the facial nerve, oval window, inner ear, temporomandibular joint, mastoid cavity, and tegmen tympani. This chapter discusses the history, embryology, classification, patient selection, surgical technique, postoperative care, risks, complications, and outcomes of surgery for canal atresia. Kiesselbach4 is credited with the first attempt at correction of congenital atresia in 1883. Unfortunately, that surgery resulted in facial nerve paralysis.5 Although Dean and Gittens6 described the first successful case with satisfactory hearing results in 1917, the high complication rates and the lack of middle ear microsurgical techniques limited surgery for atresia throughout the early twentieth century until 1947. In that year, both Ombredanne7 in France and Pattee8 in the United States separately reported a series of successful outcomes. Since that time, the development of tympanoplasty techniques and the introduction of the operating microscope have made surgery for atresia both safer and more successful. Large case series have been reported by Gill,2 Ombredanne,9 Shih and Crabtree,10 Jarhsdoerfer,5,11 Marquet,12 and De la Cruz.13,14 The development of the inner ear, derived from the otic capsule, is greatly independent of the development of the middle ear and outer ear, which take their form from the first and second branchial structures.15 The external ear develops around the primitive meatus by the fusing of the six primitive hillocks, derived from the first and second branchial arches (Table 22–1), the auricle assuming its primitive form by the end of the third month of development. The external auditory meatus develops from the first branchial groove as an ingrowth of epithelium from the primitive pinna that migrates inward toward the expanding first branchial pouch. During the sixth and seventh month of gestation, this solid core of tissue begins to hollow, creating the external meatus. The middle ear cleft is created by an expansion of the first branchial pouch, its lateral wall fusing with the inward migrating tissue of the branchial groove to form the tympanic membrane. Along with the tympanic cavity, the first branchial pouch also expands to form the eustachian tube anteriorly as well as the mastoid cavity posteriorly. Within this expanding cavity, the ossicles develop from Meckel’s cartilage (first branchial arch), which forms the malleus head and neck and incus body, as well as from Reichert’s cartilage (second branchial arch), which forms the long processes of the incus and malleus as well as the stapes superstructure. The stapes footplate has a dual origin, forming from the second branchial arch as well as from the otic capsule. The ossicles assume their final shape by the fourth month of development, and by the end of the eighth month the middle ear cleft has expanded to include all of the ossicles.
CANALOPLASTY FOR ATRESIA
HISTORY
EMBRYOLOGY
| First branchial arch | |
1st hillock | Tragus |
2nd hillock | Helical crus |
3rd hillock | Helical rim |
Second branchial arch |
|
4th hillock | Antihelix |
5th hillock | Antitragus |
6th hillock | Lobule |
The position of the facial nerve, the nerve of the second branchial arch, is dependent on the bony expansion of the middle ear as well as the expanding external auditory canal. The posterior and inferior expansion of the external canal accounts for the vertical course of the facial nerve through its mastoid segment. Failure of development of the external canal often results in an aberrant anterior displacement of the facial nerve through its descending portion, placing it at risk during drilling for canal atresia repair (Figs. 22–1 and 22–2).
The final form of the outer and middle ear structures, therefore, is dependent on the primitive structures involved as well as the time course of developmental arrest. Congenital aural atresia can range from a thin membranous canal thickening to complete absence of the tympanic bone, and from fused malleus incus formations to near absence of the malleus, incus, and stapes superstructure. Nevertheless, only 4% of congenital malformations of the external and middle ear have associated inner ear deformities, owing to their separate embryologic origins.
CLASSIFICATION
Several classification schemes have been described to define the severity of canal atresia as well as to predict the likelihood of successful hearing restoration surgery. Classification systems can be helpful in choosing appropriate surgical candidates, in counseling patients, and in analyzing and comparing results. The first widely used classification system, descriptive in nature, was proposed in 1955 by Altmann16 (Table 22–2). In 1985 De la Cruz13 proposed a further classification of Altmann groups II and III into major and minor categories (Table 22–3), proposing that patients with only minor malformations stood a reasonable chance at hearing restorative surgery, whereas patients with major malformations had a low chance of success from surgery, and were better managed by bone-anchored hearing aids to overcome their conductive hearing loss. Perhaps the most widely used classification system used to qualify patients for potential hearing restorative surgery is one proposed by Jahrsdoerfer et al11 in 1992 (Table 22–4). A 10-point grading system evaluating a variety of middle and external ear structures as seen on high-resolution computed tomography (HRCT) scanning is used to predict the likelihood of success of hearing restoration surgery. Patients receiving total scores of 5 or below are not candidates for surgery, whereas patients scoring 6 or higher are considered for surgery.
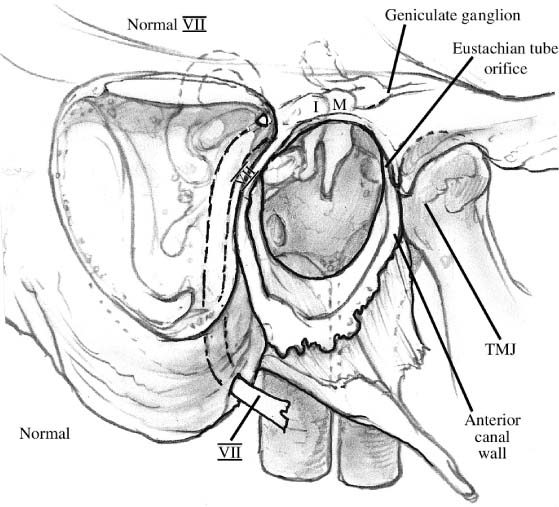
FIGURE 22–1 Normally developed ear, showing usual course of the facial nerve. I, incus; M, malleus; TMJ, temporal mandibular joint; VII, facial nerve.
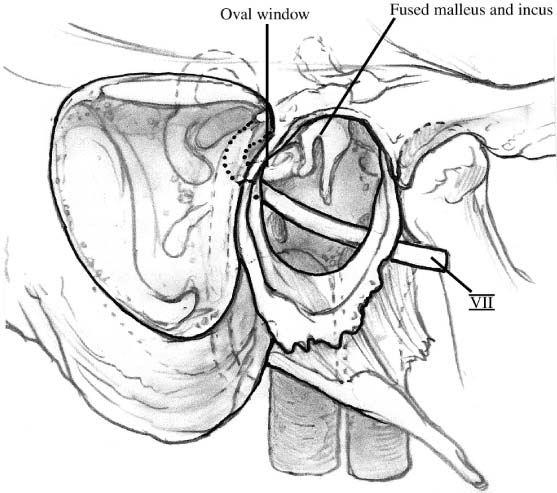
FIGURE 22–2 Aberrant anatomy in an atretic ear, with a fused malleus incus complex as well as anterior and superior displacement of the facial nerve. VII, facial nerve.
Group I (mild) | External auditory canal (EAC) is present, although hypoplastic; tympanic bone is hypoplastic, and the tympanic membrane is small; tympanic cavity is normal or hypoplastic |
Group II (moderate) | EAC is absent; tympanic cavity is small and its contents are malformed; an atretic plate is present and ossified |
Group III (severe) | EAC is absent; the tympanic cavity is missing or severely hypoplastic |
Minor malformations (candidates for hearing restorative surgery) Normal mastoid pneumatization Normal oval window Reasonable oval window facial nerve relationship Normal inner ear |
Major malformations (candidates for bone-anchored hearing aids) Poor mastoid pneumatization Abnormal or absent oval window Abnormal facial nerve course Inner ear abnormalities |
| Parameter | Points |
| Stapes present | 2 |
| Oval window open | 1 |
| Middle ear space | 1 |
| Facial nerve normal | 1 |
| Malleus incus complex present | 1 |
| Mastoid well pneumatized | 1 |
| Incus stapes connection | 1 |
| Round window normal | 1 |
| Appearance of external ear | 1 |
| Total available points | 10 |
Rating/Candidacy |
|
| 10 | Excellent |
| 9 | Very good |
| 8 | Good |
| 7 | Fair |
| 6 | Marginal |
| ≤5 | Poor |
PATIENT EVALUATION AND SELECTION
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


