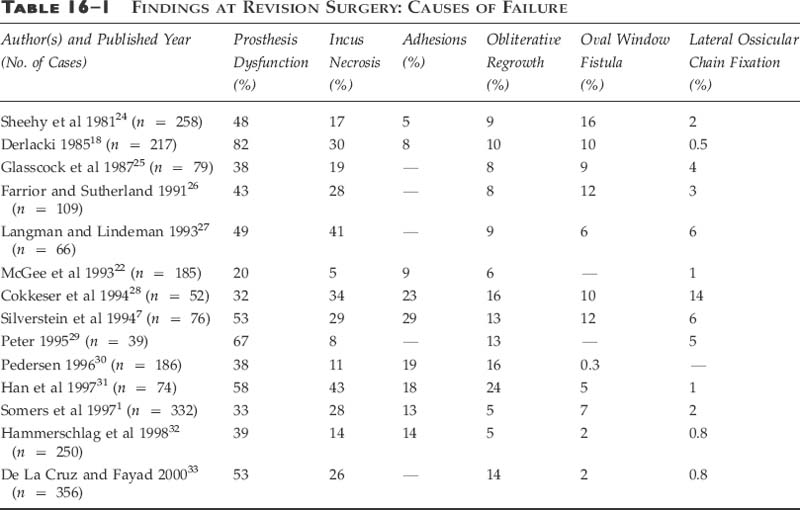
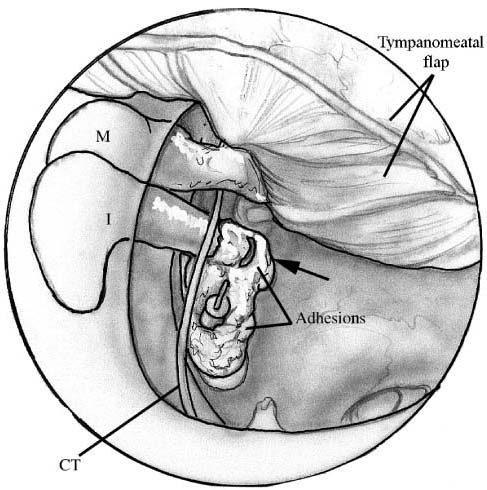
Chapter 16 “Revision stapes surgery offers an entirely different challenge to primary stapes surgery.”1 Although still the crown jewel of otology, stapes surgery is no longer performed with the breadth and wealth of experience once enjoyed; the “golden era” of otologic surgery has passed. Over the last 35 years there has been a decline in the number of stapes surgeries performed, with the depletion of backlogged older otosclerotic patients partly to blame.2 By 1970, the number of stapes surgeries performed yearly had dropped to about one third of the peak number done in 1964.2 With the vanishing numbers of these surgeries has come the loss of the broader technical proficiency enjoyed by those who trained during the earlier era. Nowadays fewer and fewer ears suitable for stapes surgery are available for teaching; so senior residents finish their training with little hands-on experience and feel ill-at-ease performing this technically demanding surgery.3 Not uncommonly, as they may encounter only a few potential stapes cases yearly, they may feel compelled to refer these either to those with a larger otologic practice or to specific centers of excellence.1 Perhaps because of the noted diminution of primary surgical cases, the advent of the “occasional” stapes surgeon, the various kinds of pros-thesis failures, or the variable results seen even in the hands of the most experienced surgeons, revision stapes surgery has emerged as an important component to modern otology. Since the description of oval window fenestration by Shea4 in 1958, there has been both the opportunity and need to correct postoperative failures following stapes surgery. Sheehy and House,5 in 1962, were the first to report the need for revision surgery. Since then, the literature has been replete with articles detailing the growing experience with revision stapes procedures as the “relative frequency of revision operations is increasing.”1 Initially the reported results of revision surgery were much worse than those of primary surgery, calling into question the safety and efficacy of this approach. With the introduction of the laser to primary stapes surgery6 and its subsequent expansion to revision surgery, however, the results encountered in the revision cases have markedly improved. Presently, as it parallels the record of primary surgical procedures, revision stapes surgery represents a safe, effective option for failures. Admittedly, although primary otosclerotic surgery may be technically demanding, revision stapes procedures are often some of the most challenging otology cases to be encountered. Whereas a virgin otosclerotic ear may have pathology centered near the oval window, the revision’s surgeon often encounters various other problems outside of the typical one centered within the fossa ovalis. Veil-like adhesions, which may extend from the tympanic membrane, the incus, the prosthesis, and the scutum, are often found obscuring one’s vision upon elevating the flap. And it is just behind, or through, these concealing investments that more potential pathology exists. Typically, the findings are characterized by one or more of the following problems: prosthesis dysfunction (displaced, loose-wire, too-short, or too-long prosthesis); ossicular resorptive osteitis (incus necrosis); oval window pathology (lateralized neomembrane, adhesions, regrowth of obliterative otosclerosis, or a perilymphatic fistula); or lateral ossicular chain fixation (adhesions, attic ankylosis, or ossification of the anterior malleal ligament). The surgeon should also be cognizant that a failure may also reflect obliterative otosclerosis at the round window. Therefore, a surgeon performing revision stapes surgery should be prepared to encounter and address any of these various findings at surgery.7 During the nearly 50 years of stapes surgery, the development of different prostheses, both with respect to design and material, has afforded better and more consistent long-term results. The type of oval window fenestration, which includes the complete stapedectomy, the platinectomy, and the small-fenestra stapedotomy, has changed in accordance with the evolution of the prosthesis and with a desire to diminish the risk of complications.8,9 Currently, with the different techniques and prostheses, primary stapes surgery results in closure of the air bone gap to less than 10 dB in nearly 85% of the cases, with an approximate 1% risk of sensorineural hearing loss. Despite acknowledging that the vast majority of primary stapes surgeries are successful, a small percentage fails. Either the patient or the surgeon recognizes a suboptimal outcome. Problems may present shortly after surgery or many years later. Common problems likely to prompt early assessment include symptoms of dizziness or vertigo or a marked drop in hearing. Presenting signs and symptoms later can include a delayed but progressive hearing loss, dizziness, dysequilibrium, vertigo, or hearing that fluctuates. Even with an uncomplicated and successful surgery it is not uncommon to have mild post-operative dizziness when perforating the footplate.10 The frequency of this occurrence has dropped with the development and use of the fenestration (stapedotomy) technique. Nonetheless, short-term dysequilibrium can occur but usually requires little more than tempered observation, rest, and occasionally medications, such as oral steroids, vestibular suppressants, or antiemetics. The dizziness or dysequilibrium is usually secondary to a serous labyrinthitis (secondary to either blood or displaced proteolytic enzymes in the vestibule),11 infrequently benign paroxysmal positional vertigo,12 or rarely a pneumolabyrinth.13 The persistence of severe vertigo, lasting more than a week and not responding to conservative measures, however, requires a more attentive assessment and raises concern for the presence of a perilymphatic fistula, an overly long prosthesis, or a reparative granuloma. Shortly after surgery, depending on the approach, technique, and postoperative course, most patients experience an appreciation of improved audition. If they judge diminished or equivocal hearing, however, then further assessment is warranted at that time. Typically this is done not only to assuage general concerns but also to assess the retention of the preoperative cochlear function. If there has been a drop in the bone curve, then attention should focus on the possibility of saccular injury (as from a too-long prosthesis), a perilymphatic fistula, or a reparative granuloma. Delayed hearing problems can occur at any time following the operative procedure. The loss of hearing acuity may reflect lenticular process erosion, obliterative otosclerotic regrowth at the fossa ovalis, lateral ossicular fixation, adhesions causing prosthesis fixation or displacement, or a perilymphatic fistula. Other pathologies can coexist, though, and may include suppurative labyrinthitis, endolymphatic hydrops, or retrocochlear disease.10 As with any otologic evaluation, obtaining a good history is very important. What was done, as well as when and under what circumstances, can help direct the assessment and possible intervention. Signs and symptoms presenting early are more likely to indicate more serious problems, for example a perilymphatic fistula, whereas those presenting years later are more likely to reflect a loss of lenticular process integrity or the propagation of adhesions with prosthesis displacement. Otomicroscopy should be performed to evaluate the appearance, position, and integrity of the tym-panic membrane. Other problems such as perforations, retraction pockets, and cholesteatomas may coexist within an otosclerotic ear, and if unrecognized, substantially alter the surgical approach and outcome. Furthermore, a dull and erythematous tympanic membrane, in the face of vertigo and sensorineural hearing loss, may be indicative of a reparative granuloma.14 Microscopic evaluation of membrane mobility, or otomicropneumotoscopy, should also be done in the office examination. Adhesive otitis media localized to the epitympanic recess, or a subtle retraction pocket into Prussak’s space, may be demonstrated by this exam. Ear insufflation is also important in evaluating two other causes of surgical failure. A temporary shift in auditory acuity with positive- or negative-pressure insufflation suggests a loose prosthetic wire. In a similar manner, but with the addition of Frenzel glasses, a perilymphatic fistula is implicated when ear insufflation produces ocular deviation and/or nystagmus (positive fistula test). Perhaps lost on some otolaryngologists is the invaluable information obtained from a careful tuning-fork evaluation. The audiologist’s assessment of hearing acuity should not preclude this examination, especially when there is concern regarding anacusis in an operated ear or when there is a coexisting bilateral moderately severe sensorineural hearing loss. The use of a tuning fork with a Bárány box masker can be invaluable. The patient must unabashedly have a full audiologic assessment. Establishment of both air and bone curves is essential. The audiologist can assist in objectifying the degree and type of hearing loss, aspects of cochlear insult, and even fluctuating hearing levels. In cases of vertigo that last beyond the immediate postoperative period, one should consider obtaining multiplanar fine-cut temporal bone computed tomography (CT).15 Prosthesis subluxation into the vestibule, an overly long prosthesis, perisaccular bone fragments, reparative granuloma, and pneumolabyrinth have all been adequately visualized and identified with this imaging modality.13,16,17 “Prior to undertaking re v ision stapes surgery, it is helpful for the otologic surgeon to know what problems he may encounter.”18 The most common finding at revision surgery is related to prosthesis dysfunction, which is reported to occur in perhaps up to 80% of the cases. The most common intraoperative findings, as cited in the literature, are summarized in Table 16–1. But pros-thesis dysfunction, like the other findings noted below, is unlikely to be the only problem detected at surgery. In more than 50% of the cases, it is typical to find more than one cause of failure.7 Within the category of prosthesis dysfunction are the reported findings of slipped, loose, too-long, too-short, bent, fractured, and displaced prostheses. Of these, a displaced prosthesis is most commonly found, and is often seen with other problems including oval window adhesions, obliterative regrowth of oto-sclerosis, a lateralized neomembrane, and incus necrosis (Fig. 16–1). The finding of a deficient incus is encountered in between 5 and 30% of revision surgeries.19 The spiculated, atrophic, or even absent long process has, at best, only limited contiguity with the stapes prosthesis (Fig. 16–2). Nadol20 notes in his series, though, that it is the only finding on histopathology in just 7% of the cases. There exist many theories as to the etiopathogenesis of this problem. The loss of incus integrity is thought to result from the disruption of an already tenuous vascularity, and can occur with any type of prosthesis.19,20 Medial fixation of the prosthesis, a loose crimping, postoperative inflammation, and fixation of the prosthesis (i.e., from adhesions or otosclerotic regrowth) creating friction at the point of incudal-prosthetic contact are postulated causes of the avascular necrosis and resorptive osteitis.20 Management of this problem may be accomplished with recrimping more proximally on the long process (which is associated with a high rate of re-erosion19) or as discussed below. FIGURE 16–1
REVISION STAPES SURGERY
PRESENTATION
EVALUATION
SURGICAL FINDINGS
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


