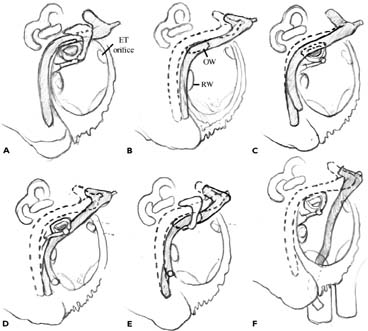
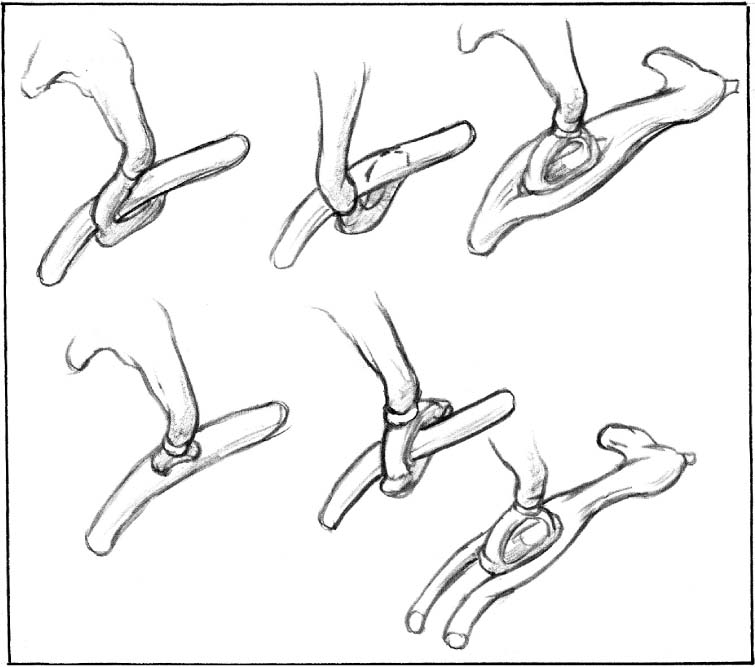
Chapter 13 Treating chronic otitis media in the pediatric population remains a major challenge. Recent advances in microbiologic evaluation and antimicrobial development provide accurate identification and effective eradication of most of the offending organisms. Nevertheless, recurrent ear infection and failure of medical management continue to require surgical intervention. In addition, cholesteatoma, congenital malformations, and cochlear implantation are some of the other indications for pediatric tympanomastoidectomy. The operative details of pediatric tympanomastoidectomy do not vary significantly from those of adult. Yet, special factors in pediatric ear surgery need to be considered preoperatively. Although tympanomastoidectomy implies a canal-wall-up (CWU) technique, canal-wall-down (CWD) mastoidectomy (also termed modified radical mastoidectomy) is briefly discussed. Most ear surgeons are conservative in operating pediatric chronic ears for these reasons: 1. The disease processes in the pediatric patients are different from those in adults. Spontaneous improvement of chronic otitis media in an adult is uncommon, whereas it is the norm for young children to improve with age. It is frequently feasible to “buy time” with medical management and CWU procedures to wait for a child to become immunologically competent and their eustachian tubes to function better.1 2. In children less than 2 years old, the facial nerve is anatomically more vulnerable and risky in radical ear surgeries.1 3. A child’s young age and future lifestyle dictate that the surgeon choose procedures that will last 70 years or longer and will endure the punishment of adolescent sports and sometimes swimming. 4. Minimal postoperative care is a major consideration in selecting types of ear procedures, as frightened children may not cooperate. 5. Young children themselves cannot consent to surgery. It may be prudent to delay an elective operation with significant risk and complication until adulthood. A discussion of the facial nerve embryology is beyond the scope of this chapter. Nevertheless, certain points are worth stressing. The facial nerve and many ossicular parts, notably the stapedial crura, the manubrium of the malleus, and the long arm of the incus, are derived from the second branchial arch. Malformation in one may suggest defect in another.2 The occasional ear surgeon is more likely to operate on ears with minor malformations or with no apparent abnormality at all. Such operations actually pose a greater risk of facial nerve injury than do operations on major malformations because the surgeon may not suspect congenital abnormality. During a routine middle ear or mastoid exploration, extra caution must be paid to dissect “fibrous tissue bands” or “adhesions,” because they may actually represent a dehiscent and aberrant facial nerve. During the preoperative period, subtle or “soft” signs, such as abnormal-looking auricles, preauricular pits, a short and blunt malleus, and small tympanic membrane, should alert the surgeon to a congenitally abnormal ear. In children with identifiable congenital middle ear malformations, expect facial nerve abnormalities. Intraoperatively, to avoid facial nerve injury, be suspicious of any soft tissue tubular structure regardless of its location.3 Keen observation skills, quality imaging modalities, and a thorough knowledge of temporal bone embryology and anatomy are critical in preventing facial nerve injury. The surgeon must understand malformation-related variants of nerves and vessels to avoid catastrophic events. Jahrsdoerfer and Hall4 reported that 24% of ears with congenital anomalies of the middle ear had an aberrant course of the facial nerve. In the middle ear, two most common facial nerve anomalies are nerve displacement (Fig. 13–1) and fallopian canal dehiscence. The nerve may be found at the level of the promontory and covered only by respiratory mucosa. It may be found inferior to or at the level of the stapes or oval window. Sometimes the stapes superstructure ends blindly in the soft tissue substance of the facial nerve. The facial nerve may also bifurcate around an intact stapes, and the split nerve may or may not remain separate (Fig. 13–2). Discovering a malformed stapes during the operation should immediately alert the surgeon that the facial nerve could be out of position. If the oval window is absent, in almost 80% of the cases there is facial nerve displacement.5 Lastly, an uncovered and displaced facial nerve may be found in association with a congenital cholesteatoma. An inferiorly displaced facial nerve may conceal the round window. It is recommended not to transpose the facial nerve simply to locate the round window. If an oval window is present, hearing preservation procedures should be attempted. It is uncommon to encounter an absent round window as an isolated anomaly. If an oval window is absent, a round window may or may not be present. If an oval window is present, a round window is almost always present.3 FIGURE 13–1 (A F) Patterns of facial nerve displacement in congenital middle ear malformations. ET, eustachian tube; OW, oval window; RW, round window. FIGURE 13–2 Patterns of stapes malformations in relation to facial nerve associated with congenital middle ear malformation. Finding a large chorda tympani nerve warrants a pause and reappraisal of the operative condition. It is best not to sacrifice any large chorda tympani nerve because it may be the real facial nerve with a sharp anterior and lateral curving feature. At least it may herald an abnormal facial nerve. Electrical stimulation is of no diagnostic value as the chorda tympani nerve propagates the electrical stimulation to the facial nerve. The mastoid portion of the facial nerve almost always migrates anteriorly with external and middle ear anomalies.3 Ossicular anomalies without malformation of the external ear have been classified into three groups: malleus and/or incus fixation, incudostapedial disconnection, and stapes fixation. Combinations of these anomalies may occur and may be associated with facial nerve and otic capsule anomalies. Isolated ossicular chain malformations are often bilateral, especially in familial cases of congenital ossicular malformations. The most commonly involved ossicle is the stapes; least commonly, the malleus.6 The most significant vascular malformation is the aberrant internal carotid artery (ICA). The ICA is separated from the tympanic cavity by a thin (less than 0.5 mm) bony carotid plate. Rarely, this plate is dehiscent. A second abnormality is the persistent stapedial artery. There may or may not be an associated aberrant ICA. A third abnormality is a dehiscent jugular bulb that may protrude into the middle ear cavity. 1. Audiometry is always needed. In general, post-operative air bone gaps are larger than preoperative ones when the stapes superstructure is involved by diseases. Though rare, operation on the wrong ear has happened. Therefore, verify the correct ear to operate upon with the audiogram immediately before the surgery. 3. Some inner ear anomalies can also be detected on CT. Inner ear defects like a wide internal auditory canal (IAC) (>10 mm in diameter), enlarged vestibular, or cochlear aqueduct predispose patients to a perilymphatic gusher during cochlear implantation. Absence of the IAC is a contra-indication for cochlear implantation. 4. Magnetic resonance imaging (MRI) scanning is indicated if there is suspicion of disease involvement or invasion of the dura, sub- or epidural abscess, brain tissue herniating into the mastoid, invasion of the membranous labyrinth or facial nerve, or sigmoid sinus thrombosis.
PEDIATRIC TYMPANOMASTOIDECTOMY
GOALS AND TYPES OF SURGERY
FACIAL NERVE ABNORMALITY
TYPES OF CONGENITAL MALFORMATIONS OF THE FACIAL NERVE
OSSICULAR ABNORMALITY
VASCULAR ABNORMALITY
OPERATIVE CONSIDERATIONS
PREOPERATIVE TESTS
INTRAOPERATIVE MONITORING
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


