Neck ultrasound has been shown to be critical for the postoperative evaluation of thyroid cancer patients. The thyroid bed and surrounding tissues are evaluated for the presence of recurrence or nodal disease.
The number of patients diagnosed with thyroid cancer has increased markedly in the past 25 to 30 years caused, at least in part, by improved imaging and diagnostic techniques. Current sonographic techniques allow accurate visualization of even small thyroid lesions. Increasing use of imaging techniques, such as CT, positron emission tomography, and MRI, has resulted in the identification of many incidental thyroid lesions, which have a similar risk of malignancy as nodules identified by other means, such as palpation . The widespread availability of ultrasound-guided fine-needle aspiration (US-FNA) with cytologic analysis has made the diagnosis of thyroid malignancy a quick, office-based process. The end result of the increasing detection of thyroid cancer is a large number of postthyroidectomy patients who require surveillance and long-term management. This article addresses the sonographic evaluation of postthyroidectomy cancer patients, and the postparathyroidectomy patient with a recurrence.
The initial treatment for a thyroid cancer patient is total or near-total thyroidectomy. The surgery is followed in many cases by radioactive iodine ablation to destroy any remaining thyroid cells, either in the bed or in regional lymph nodes. This treatment approach assumes that clinically inapparent cancer cells may have already spread to the regional lymph nodes at the time of initial diagnosis. The risk of recurrence for thyroid cancer varies with the histologic type of malignancy, but may be as high as 10% to 20% in patients with papillary or follicular cancer . Regardless of the type of cancer, all postthyroidectomy cancer patients are monitored with blood tests, such as thyroglobulin and calcitonin (discussed elsewhere in this issue). Neck US has been shown to be critical for the postoperative evaluation of thyroid cancer patients, because recurrences may occur in patients with negative thyroglobulin levels and approximately 50% of recurrences may be seen in low-risk patients .
Imaging of the thyroid bed
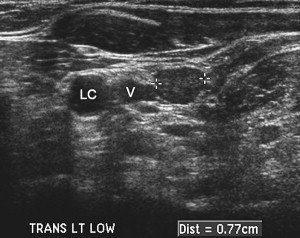
When any patient presents to the US department for imaging postthyroidectomy, a thorough sonographic evaluation of the thyroid bed and surrounding neck is performed. Those patients with elevated thyroidglobulin or calcitonin, positive thyroglobulin antibodies, or a known high-risk or aggressive primary cancer are at particularly elevated risk and require intensive study. Sonographic evaluation of the postthyroidectomy patient is performed with a high-resolution linear transducer, typically with frequencies of 10 to 15 MHz. Newer probe frequencies may reach as high as 17 MHz. Without the thyroid to provide a landmark in the lower neck, inexperienced imagers may have difficulty differentiating normal structures from pathology. The imager should be familiar with the normal anatomy and the normal postsurgical appearance of the neck, so as to not mistake the vocal cords or cricoid cartilage as pathology . In the postthyroidectomy patient, the carotid artery and jugular vein slide medially into the space previously occupied by the thyroid. The right carotid artery typically lies immediately adjacent to the trachea, whereas the left carotid is at the lateral edge of the esophagus ( Fig. 1 ). The thyroid bed should be imaged in both transverse and longitudinal planes; however, the transverse plane is most useful for the detection of lesions. Slow steady movement of the transducer across the thyroid bed, including the former site of the isthmus, allows identification of even small abnormalities. There may be a variable amount of echogenic tissue in the thyroid bed, representing residual thyroid tissue or postoperative change.

For the purposes of this article, masses in the thyroid bed are termed “recurrences.” In many instances, however, the recurrence is actually an abnormal internal jugular chain lymph node that has slid medially into the potential space created postthyroidectomy. The differentiation is only possible by the pathologist, when lymphoid tissue is seen around the cancer cells.
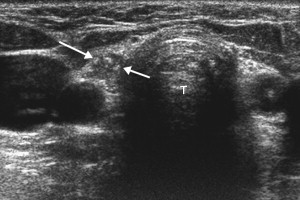
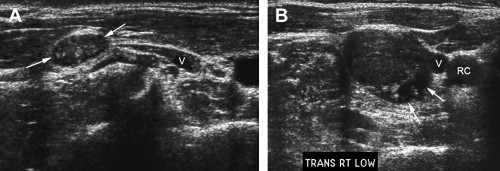
A recurrence in the thyroid bed is typically round and hypoechoic, situated between the carotid and the trachea. Most have well-defined margins, and some may have microcalcifications ( Fig. 2 ) or a cystic component. Despite a reported accuracy of 90% or greater for the diagnosis of cancer recurrence with US , sonography alone is insufficient because of the overlap in appearance with such lesions as postoperative fibrosis, suture granulomata, reactive lymph nodes, parathyroid adenoma, and other etiologies . US-FNA is typically necessary to confirm a recurrence. Evaluation for the presence of thyroglobulin in the needle aspirate may be more sensitive than cytology for the diagnosis of recurrent thyroid cancer .
Sonographic characteristics of nodal recurrence
Once the thyroid bed has been examined, abnormal internal jugular (IJ) chain nodes should be searched for bilaterally. Scanning in transverse plane helps the imager differentiate enlarged nodes from the normal strap muscles of the neck. Cancers that arise in the mid and upper thyroid gland typically spread to the ipsilateral low and mid IJ chain nodes. Isthmic and lower pole cancers spread to the inferior pretracheal nodes immediately below the thyroid, extending toward the superior mediastinum. These nodes are often overlooked, but are a common site for metastatic disease. Because of the slow growing nature of many thyroid cancers, it may be decades before an abnormal lymph node becomes clinically or sonographically apparent. In certain circumstances, such as suspected recurrence of aggressive tumors in patients who have already undergone local nodal resection, the sonographic examination must extend to the supraclavicular, lateral cervical, and submandibular nodes. Any new palpable lesion in the neck should also be imaged.
Sonographically, abnormal cervical lymph nodes in the thyroid cancer patient may be caused by inflammatory or infectious processes, or even metastatic disease from other cancers. Sonographic characteristics of each lymph node can be analyzed to help predict benign or malignant disease. The submandibular region nodes are commonly enlarged at sonography in both normal and affected patients, but they are only rarely involved by thyroid cancer. In the postthyroidectomy patient, the sonographic criteria used to raise concern for malignancy in a node are similar to the preoperative patient, with the exception of node size. For the follow-up of a thyroid cancer patient, every middle and lower IJ chain node should be included in the US report, regardless of size. Nodes or masses as small as 3 mm should be reported, with three dimensions and the location for each node. However, simply listing measurements of any node found in the US report is inadequate. Each node should be categorized by the sonologist in some fashion as benign, indeterminate, or worrisome or suspicious.
The challenge for the sonologist is to separate nodes with metastatic disease from normal reactive nodes. Benign sonographic criteria include a long thin shape, a well-defined echogenic hilum, and vascularity entering into the center or hilum of the node and extending toward each tip ( Fig. 3 ) . Nodes with these characteristics can be described as “benign appearing,” “likely benign,” or even “nonworrisome” in the US report. Other nodes with a nonspecific slightly abnormal appearance, such as a somewhat rounded shape, can be termed “not completely benign appearing” or “indeterminate” ( Fig. 4 ). Sonographically indeterminate nodes may require US-FNA depending on the clinical circumstances, and should be carefully documented so that interval growth or appearance of worrisome characteristics within the node can be appreciated and acted on with biopsy in the future. The time for follow-up varies; in the low-risk patient, repeat sonography in 6 months is appropriate, with additional follow-up at 9- to 12-month intervals until the nodes are established as stable. In the high-risk patient with nodes of indeterminate appearance, if the thyroglobulin is negative, follow-up in 4 to 6 months is appropriate. In a patient with an aggressive type of cancer or elevated thyroglobulin, immediate US-FNA may be warranted.

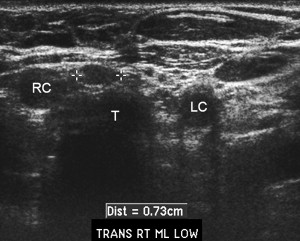
Sonographic criteria that raise suspicion for malignancy include the presence of calcifications, cystic or necrotic changes, a rounded or irregular shape, abnormal vascularity, and loss of the normal echogenic hilum . Of these, the first two are most useful, with specificities at or approaching 100% ( Fig. 5 ). Other criteria have specificities ranging from 70% to 90% . If any of these criteria are present, or if there is detectable serum thyroglobulin, US-FNA should be performed of the node in question. The use of US guidance for FNA has been shown to increase accuracy , because many of these lesions are quite small and nonpalpable. Consideration should be given to aspirating more than one lymph node for assistance in surgical planning. For example, if there are bilateral abnormal IJ nodes, the most abnormal appearing node on each side should be sampled. The pretracheal nodes can be difficult to identify and image particularly in the sagittal plane with a linear probe, but these are a common site of metastatic disease, especially in patients whose primary tumor was in the lower lobes, as stated previously ( Fig. 6 ).
Sonographic characteristics of nodal recurrence
Once the thyroid bed has been examined, abnormal internal jugular (IJ) chain nodes should be searched for bilaterally. Scanning in transverse plane helps the imager differentiate enlarged nodes from the normal strap muscles of the neck. Cancers that arise in the mid and upper thyroid gland typically spread to the ipsilateral low and mid IJ chain nodes. Isthmic and lower pole cancers spread to the inferior pretracheal nodes immediately below the thyroid, extending toward the superior mediastinum. These nodes are often overlooked, but are a common site for metastatic disease. Because of the slow growing nature of many thyroid cancers, it may be decades before an abnormal lymph node becomes clinically or sonographically apparent. In certain circumstances, such as suspected recurrence of aggressive tumors in patients who have already undergone local nodal resection, the sonographic examination must extend to the supraclavicular, lateral cervical, and submandibular nodes. Any new palpable lesion in the neck should also be imaged.
Sonographically, abnormal cervical lymph nodes in the thyroid cancer patient may be caused by inflammatory or infectious processes, or even metastatic disease from other cancers. Sonographic characteristics of each lymph node can be analyzed to help predict benign or malignant disease. The submandibular region nodes are commonly enlarged at sonography in both normal and affected patients, but they are only rarely involved by thyroid cancer. In the postthyroidectomy patient, the sonographic criteria used to raise concern for malignancy in a node are similar to the preoperative patient, with the exception of node size. For the follow-up of a thyroid cancer patient, every middle and lower IJ chain node should be included in the US report, regardless of size. Nodes or masses as small as 3 mm should be reported, with three dimensions and the location for each node. However, simply listing measurements of any node found in the US report is inadequate. Each node should be categorized by the sonologist in some fashion as benign, indeterminate, or worrisome or suspicious.
The challenge for the sonologist is to separate nodes with metastatic disease from normal reactive nodes. Benign sonographic criteria include a long thin shape, a well-defined echogenic hilum, and vascularity entering into the center or hilum of the node and extending toward each tip ( Fig. 3 ) . Nodes with these characteristics can be described as “benign appearing,” “likely benign,” or even “nonworrisome” in the US report. Other nodes with a nonspecific slightly abnormal appearance, such as a somewhat rounded shape, can be termed “not completely benign appearing” or “indeterminate” ( Fig. 4 ). Sonographically indeterminate nodes may require US-FNA depending on the clinical circumstances, and should be carefully documented so that interval growth or appearance of worrisome characteristics within the node can be appreciated and acted on with biopsy in the future. The time for follow-up varies; in the low-risk patient, repeat sonography in 6 months is appropriate, with additional follow-up at 9- to 12-month intervals until the nodes are established as stable. In the high-risk patient with nodes of indeterminate appearance, if the thyroglobulin is negative, follow-up in 4 to 6 months is appropriate. In a patient with an aggressive type of cancer or elevated thyroglobulin, immediate US-FNA may be warranted.



