Reoperative surgery for hyperparathyroidism is associated with increased incidence of complications including vocal cord paralysis, permanent hypoparathyroidism, and persistent hypercalcemia. Surgical re-exploration should consist of symptomatic or low-risk patients. The use of nuclear medicine imaging, ultrasound, and high-resolution CT and MRI may aid in surgical planning. Knowledge of potential
Hyperparathyroidism has become recognized as a disease entity over the last century. The chronic effects of hyperparathyroidism result in osteoporosis, nephrolithiasis, renal failure, hypertension, increased cardiovascular risk, depression, mental status changes, and fatigue. Fortunately, hyperparathyroidism can be cured on initial surgical exploration in greater than 90% of cases, and in experienced hands greater than 95% . The gold standard of routine bilateral neck exploration with subsequent biopsy confirmation of both enlarged and normal-sized glands has given way to less invasive techniques over the last two centuries as the initial surgical treatment. Unfortunately, preoperative localization studies may fail to locate the affected gland or glands. In addition, preoperative localization studies have the unwanted potential to lure less experienced surgeons to embark on attempts at surgical cure of hyperparathyroidism. Previously, patients may have been referred to high-volume centers for the longer, more invasive bilateral explorations. As a result, many patients require evaluation for reoperation to control persistent hyperparathyroidism.
Evaluation for reoperative parathyroidectomy
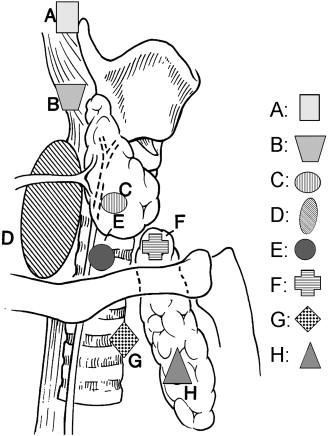
Re-exploration for control of hyperparathyroidism in a patient with prior thyroid or parathyroid surgery is complicated by previous scarring within the surgical bed. This results in distortion of the surgical planes, often obscuring normal anatomy of recurrent and superior laryngeal nerves. Abnormal parathyroid glands may be encased in bundles of scar, making identification of abnormal or normal glands much more difficult. In a reoperative case, the incidence of either postoperative hypoparathyroidism or persistent hyperparathyroidism is increased and may approach 10% . Surgical re-exploration in this patient population may result in significant complications in up to 27% of patients . In surveyed patients after reoperation for persistent hyperparathyroidism, only 70% of patients had resolution of symptoms and 19% stated they would not consent to reoperation again. Interestingly, the patients with nerve injuries and permanent hypoparathyroidism reported better satisfaction with reoperation than patients with persistent hyperparathyroidism. Patients with unidentified parathyroid glands may have a higher incidence of tumors in ectopic locations, multigland hyperplasia, and may be associated with recurrence of parathyroid carcinoma. Ectopic parathyroid locations include thymus, intrathyroidal, carotid sheath, retroesophageal, superior mediastinum, tracheoesophageal groove, submandibular, and posterior mediastinum ( Fig. 1 ) .
Patients being considered for reoperation should be limited to either low-risk re-explorations or symptomatic patients. Low-risk exploration specifically refers to exploration of an unexplored field as in the case of unsuccessful minimal exploration unilateral parathyroidectomy. In situations of previous unilateral exploration, the unexplored side is used unless localization studies suggest the initial side to harbor the active gland. Provided the initial surgeon has not violated the opposite side, scarring and inflammation should be minimal. Preferably, surgical exploration should be delayed for at least 6 months after initial surgery to allow for inflammation and scarring to subside. Patients with life-threatening hypercalcemia, failing renal function, severe osteoporosis, mental status changes, and constipation should be considered for re-exploration. Patients who are marginally symptomatic should be encouraged to consider medical management as a first line of treatment. In these patients, the 1990 National Institutes of Health guidelines from the Consensus Development Conference may help define surgical candidates.
Baseline retesting of serum calcium, intact parathyroid hormone, and 24-hour urine calcium should be undertaken to ensure the diagnosis of hyperparathyroidism exists. In addition, such medications as lithium, thiazides, and vitamin D should be eliminated. Systemic diseases, such as sarcoidosis, multiple myeloma, and benign familial hypocalciuric hypocalcemia, should be investigated as potential contributors of hypercalcemia.
Previous operative reports and surgical pathology reports should be obtained and reviewed when available. This allows for surgical planning in the high-yield, low-risk areas. Pathologically verified glands may have been clipped and left in situ or perhaps autotransplanted, which inherently may result in directed re-exploration. Often, what seemed to be parathyroid tissue to the operating surgeon is found to be merely lymph nodes or thyroid tissue when analyzed microscopically by pathologic analysis.
Preoperative imaging
Localization studies may aid in identifying ectopic and hyperfunctioning glands, while reducing the morbidity of re-exploration . The previous knowledge of any parathyroid or thyroid surgery allows for more appropriate interpretation of two-dimensional or three-dimensional volume imaging, such as high-resolution ultrasound, CT, or MRI. Imaging studies should be repeated and should include sestamibi imaging to look for new or ectopic activity . Ultrasound examination should determine presence of thyroid nodules and paratracheal masses, which may represent enlarged parathyroid glands. CT or MRI may also be considered to evaluate the mediastinal and retroesophageal regions that may not be visualized by ultrasound . Selective venous sampling by interventional radiology may help determine laterality and possibly venous outflow location of the most active gland .
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


