This article presents an overview of medical management of persistent or recurrent differentiated thyroid cancer, in particular focusing on monitoring strategy and treatment plans. Most patients with differentiated thyroid carcinoma can be successfully rendered to be free of disease with initial treatments, and those with persistent or recurrent disease can still expect long-term survival when they are monitored properly and treated accordingly. Along with serum thyroglobulin, neck ultrasonography, and radioactive iodine whole-body scans, the use of cross-sectional imaging studies and (18F) fluoro-2-deoxy-D-glucose-positron emission tomography have facilitated the effort in localizing lesions and traditional treatments can be implemented effectively. For disease resistant to conventional therapies, there are new treatment modalities emerging and being tested, including several agents targeting specific signaling pathways, each of which may offer the potential remedy.
The incidence of thyroid cancer has remarkably increased in recent years, from 4.9 cases per 100,000 in 1975 to 9.8 per 100,000 in 2004 in the United States . According to the recent data, the incidence of thyroid cancer in the United States was estimated to be 33,550 in the year 2007, closely following the incidence of leukemia, pancreatic cancer, and oropharyngeal cancer but preceding that of ovarian cancer, multiple myeloma, esophageal cancer, and cervical cancer . Between 1988 (the first year SEER collected data on tumor size) and 2002, 49% of the increase consisted of cancers measuring 1 cm or smaller; 87% consisted of cancers measuring 2 cm or smaller, suggesting the recent rise in its incidence is mainly caused by early detection of small tumors . It probably resulted from incidental discovery of thyroid nodules during the widespread use of imaging for unrelated reasons and readily available ultrasound-guided fine-needle aspiration biopsy.
Differentiated thyroid carcinoma consists of papillary thyroid carcinoma and follicular thyroid carcinoma, accounting for approximately 90% and 10% of new cases, respectively . Despite the dramatic rise in its incidence, differentiated thyroid carcinoma has maintained a low mortality rate in the past 25 years . The survival rates of papillary and follicular thyroid carcinomas were reported to be 98% and 92% in 10 years , and 94% and 84% in 40 years , respectively.
The primary treatment of differentiated thyroid carcinoma comprises thyroidectomy, near-total or total in most cases, with or without lymph node dissection and subsequent radioactive iodine remnant ablation and thyroid-stimulating hormone (TSH) suppression with thyroxine. With regard to specific recommendations for initial treatment, there have been comprehensive guidelines published that readers are referred to for detailed information.
In general, total or near total thyroidectomy is indicated for patients with papillary thyroid carcinoma more than 1 to 1.5 cm in diameter, a personal history of radiation exposure to the head and neck, a first-degree family history of differentiated thyroid carcinoma, unfavorable histology (eg, tall, insular, columnar cell variant), extrathyroidal invasion, or cervical or distant metastasis. For follicular thyroid carcinoma, total thyroidectomy is indicated perhaps except for small tumors with minimal capsular invasion.
Radioactive iodine remnant ablation is indicated for all TNM stage III and IV disease, most stage II disease, and selected stage I (<2 cm of primary tumor in diameter) disease if they demonstrate unfavorable features, such as multifocal disease, nodal metastases, extrathyroidal extension, vascular invasion, or aggressive histologies. The benefit of radioactive iodine remnant ablation in low-risk patients has not been clearly verified but may improve detection sensitivity and specificity during the follow-up. Radioactive iodine remnant ablation is not recommended for small (<1–2 cm), intrathyroidal, well-differentiated papillary thyroid cancer without evidence for worrisome pathologic features or evidence of metastases outside the thyroid.
The degree of long-term TSH suppression has been a matter of debate. For high-risk patients, current guidelines uniformly endorse TSH to be kept below 0.1 mIU/L unless there are any contraindications. This was supported by a recent report by Jonklaas and colleagues with data analysis on 1548 patients showing that high-risk patients had fewer recurrences and better survival rates when their TSH were suppressed to a undetectable level. In regard to low-risk patients, although the National Comprehensive Cancer Network (NCCN) and British thyroid association propose TSH levels below the reference range (typically 0.1–0.5 mIU/L), American thyroid association and European consensus recommend them in the low normal range (typically 0.5–1 mIU/L). A recent report by Hovens and colleagues supports aiming at TSH levels in low normal range for low-risk patients. It was a single-center observational study in 366 consecutive patients with differentiated thyroid carcinoma during a median follow-up of 8.85 years. In their study where most patients were at low risk, the effect of median TSH on relapse only became discernable at a cutoff level of 2 mU/L, whereas at cutoff levels of 0.1 and 0.4 mU/L no significant differences in relapse were observed.
Although most thyroid cancer patients do well after initial therapy and are at low risk of recurrence and death from disease, tumor recurrence occurs at clinically significant rates. In the Ohio State series, the overall recurrence rate of differentiated thyroid carcinoma was at 23.5% with local recurrence rate of 17.8% and distance recurrence rate of 7.5% at a median of 16.6 years after diagnosis . Mayo Clinic series presents similar data with 25-year tumor recurrence rates at 14% . Local recurrence occurs largely in the neck, most often in the lymph nodes . Distant metastasis is most frequently found in the lungs (50%) followed by bones (25%), lungs and bones (20%), or at other sites (5%) . The disease recurrence holds significant clinical implication because 30-year cancer mortality rates were reported to be about 12% in patients with local recurrence and 43% in those with distant recurrence .
Because most patients are at low risk of recurrence and death from disease but clinically evident recurrences cause significant morbidity and mortality, it is of paramount importance to establish a long-term follow-up strategy that keeps tests to a minimum but provides sufficient sensitivity to detect recurrence at an early stage when conventional treatment modalities can be effective and achieve long-term survival. At the same time, there have been recent advances in the novel approaches of therapy for refractory disease. This article reviews a follow-up strategy and treatment options for persistent or recurrent differentiated thyroid carcinoma. Also briefly covered are investigational treatments that use agents targeting signaling pathways, redifferentiation agents, and gene therapy.
Risk stratification
Risk stratification is an essential element in managing patients with differentiated thyroid carcinoma. There have been several prognostic indicators of disease-specific mortality and risk of recurrence predominantly tested in a retrospective manner . These include
- 1.
Patient factors, such as age at diagnosis and gender
- 2.
Tumor factors, such as size, multicentricity, histology, extrathyroidal invasion, nodal metastasis, and distant metastasis
- 3.
Therapeutic factors, such as completeness of resection and treatment with radioactive idodine-131
Appreciation of these relevant prognostic factors has led to several staging or scoring systems , among which the TNM system is most widely accepted. It also provides a means to classify patients with differentiated thyroid carcinoma into low-, intermediate-, or high-risk groups according to cause-specific mortality. Because most disease-related deaths result from clinically significant recurrent events at local or distant sites, although they are not perfectly corresponding, the previously mentioned categorization also offers information predicting recurrence in patients who have undergone initial surgery and radioactive iodine-131 remnant ablation. Low-risk patients have the following characteristics: no local or distant metastases, complete resection of all macroscopic tumor, no tumor invasion of locoregional tissues or structures, no aggressive histology (eg, tall cell, insular, columnar cell carcinoma) or vascular invasion, and, if I-131 is given, no I-131 uptake outside the thyroid bed on the first posttreatment radioiodine whole-body scans . Intermediate-risk patients have microscopic invasion of tumor into the perithyroidal soft tissues at initial surgery or tumor with aggressive histology or vascular invasion . High-risk patients have macroscopic tumor invasion, incomplete tumor resection, distant metastases, or I-131 uptake outside the thyroid bed on the posttreatment scans . Additionally, both extremes of age (age less than 15 years or greater than 45 years) at diagnosis and tumor size greater than 4 cm in diameter have been shown independently to predict increased risk of recurrence . Although they are at high risk for recurrent disease, however, pediatric patients with differentiated thyroid carcinoma have an excellent long-term survival. The reason is thought to be the differences in genetic mutations and growth factor expression patterns of childhood thyroid cancers compared with those of adults and a robust immune response in children with thyroid cancers . A response-to-therapy variable over the course of follow-up period should also be taken into account for risk stratification. The follow-up strategy to detect recurrence should be tailored on a case-by-case basis, and the professional judgment of physicians plays an important role in the care of patients with differentiated thyroid carcinoma.
Surveillance for disease recurrence
The goals of surveillance of patients with differentiated thyroid carcinoma are to detect clinically significant recurrences at an early stage when effective therapy can be used, and at the same time to minimize unnecessary tests, procedures, or treatment that can cause discomfort and anxiety to the patients without proved benefit. Commonly used tests include (1) serum thyroglobulin determination, (2) neck ultrasonography, (3) routine diagnostic whole-body scans, and (4) cross-sectional imaging, such as CT and MRI, and (18F) fluoro-2-deoxy-D-glucose–positron emission tomography (18 FDG PET) CT scanning.
In the past decade, there has been an important paradigm shift with growing confidence on the use of stimulated serum thyroglobulin and neck ultrasonography, and decreased use of routine diagnostic whole-body scans, in particular, for low-risk patients. Modern assays for serum thyroglobulin determination with improved sensitivity and the use of recombinant human thyrotropin (rhTSH) for stimulated serum thyroglobulin have made a considerable change in the surveillance protocol of disease recurrence . For practical purposes, thyroglobulin levels should be measured serially with the same method in the same laboratory whenever possible and antithyroglobulin antibodies should be checked in the same sample, because considerable variability has been reported across the methods and antithyroglobulin antibody can cause the assay interference, often giving falsely low thyroglobulin values . Although thyroglobulin is a valuable tumor marker of well-differentiated thyroid carcinoma, its production can be significantly reduced even with endogenous or exogenous TSH stimulation in poorly differentiated tumor . Thyroglobulin measurement should be accompanied by other follow-up modalities, especially in intermediate- and high-risk patients.
Neck ultrasonography has become the principal imaging study in patients with thyroid cancer . Most of the recently updated guidelines view a combination of serum thyroglobulin measurement and routine neck ultrasonography as an excellent follow-up tool for low-risk patients, given its high sensitivity and negative predictive value . Ultrasonography may have a particular role when serum thyroglobulin measurements are unreliable because of the presence of assay interference or poor thyroglobulin production by the tumor. In general, neck ultrasonography is recommended at 6 and 12 months after radioactive iodine remnant ablation, and then yearly for at least 3 to 5 years, depending on the risk for recurrence and the thyroglobulin status of each patient. Because ultrasound evaluation is uniquely operator-dependent, dedicated ultrasonographers specialized in thyroid imaging are preferred to achieve optimum sensitivity and specificity for detection of disease recurrence.
Routine diagnostic whole-body scans have low sensitivity and are usually not needed in low-risk patients who are clinically free of disease with negative stimulated serum thyroglobulin and neck ultrasonography . It may be of some value in the follow-up of patients with intermediate or high risk of recurrent disease. The NCCN guidelines recommend regular diagnostic whole-body scans either with withdrawal of thyroid hormone or rhTSH every 12 months until no radioiodine-avid tumor is evident for patients with detectable thyroglobulin, distant metastases, or soft tissue invasion on initial staging . Because of the concerns over I-131–induced stunning of thyroid cancer, if diagnostic whole-body scans are indicted, the use of I-123 or low-dose I-131 (1–3 mCi) is preferred.
The role of cross-section imaging and 18 FDG PET scanning is less clear for surveillance of disease recurrence. In general, additional nonradioiodine imaging, such as 18 FDG PET scanning with or without CT, is considered for patients whose whole-body scans are negative but thyroglobulin levels are elevated, commonly more than 2 to 5 ng/mL . The 18 FDG PET scanning becomes especially sensitive in identifying recurrence when thyroglobulin levels are greater than 10 ng/mL . CT of neck to detect local disease extension to surrounding structures, such as trachea or esophagus, CT of lungs, and MRI of bones and brain are used as complementary imaging modalities. Iodinated contrast should be avoided if radioiodine treatment is anticipated. Bone scintigraphy is poorly sensitive because most metastatic lesions of differentiated thyroid carcinoma are lytic .
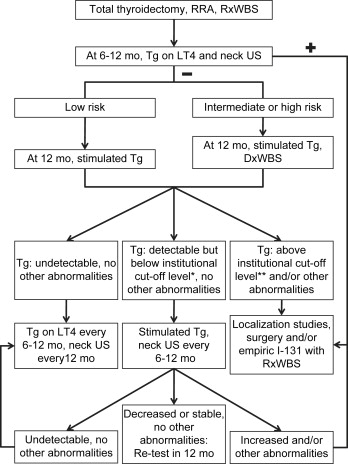
Current guidelines are in agreement on the subject of the general follow-up strategy after initial therapy . Follow-up strategy based on risk stratification is summarized in Fig. 1 . After total thyroidectomy and radioactive iodine remnant ablation followed by posttreatment scans, the initial follow-up in 6 to 12 months comprises neck ultrasonography and suppressed serum thyroglobulin measurements. If either of these tests is positive, the localization studies for persistent or recurrent disease should be pursued. If both the neck ultrasonography and suppressed serum thyroglobulin do not reveal any evidence of disease, low-risk patients can be followed with stimulated thyroglobulin alone, whereas intermediate- and high-risk patients usually require diagnostic whole-body scans along with stimulated thyroglobulin measurement. Thereafter, the disease-free patient can be followed with suppressed thyroglobulin every 6 to 12 months and neck ultrasonography on a yearly basis depending on the risk of recurrence. The timing or necessity of subsequent stimulated testing is uncertain for those found to be free of disease. If thyroglobulin levels are detectable but below the institutional cut-off level (commonly, between 2 and 5 ng/mL after rhTSH stimulation or below 10 ng/mL after thyroid hormone withdrawal) and no other evidence of disease exists, stimulated thyroglobulin measurement and neck ultrasonography should be repeated in 6 to 12 months. An increase of thyroglobulin levels on serial measurements likely indicates a disease progression . In a situation of an elevated thyroglobulin or other abnormalities, the imaging studies are recommended typically with CT of the chest in addition to neck ultrasonography. If imaging is negative for surgically treatable disease, then empiric therapy with radioiodine is considered for possible treatment and to facilitate localization of persistent or recurrent disease on posttreatment whole-body scans. High-risk patients may require additional cross-sectional imaging studies or 18 FDG PET scans because they tend to have disease recurrence with poorly differentiated tumors whose ability to produce thyroglobulin and concentrate radioiodine may be diminished.
Follow-up should be lifelong even for low-risk groups because of the following reasons: the disease may have a prolonged natural history, late recurrence can occur, late side effects of I-131 treatment may develop, and clinical consequences of TSH suppression with thyroxine treatment require monitoring .
Surveillance for disease recurrence
The goals of surveillance of patients with differentiated thyroid carcinoma are to detect clinically significant recurrences at an early stage when effective therapy can be used, and at the same time to minimize unnecessary tests, procedures, or treatment that can cause discomfort and anxiety to the patients without proved benefit. Commonly used tests include (1) serum thyroglobulin determination, (2) neck ultrasonography, (3) routine diagnostic whole-body scans, and (4) cross-sectional imaging, such as CT and MRI, and (18F) fluoro-2-deoxy-D-glucose–positron emission tomography (18 FDG PET) CT scanning.
In the past decade, there has been an important paradigm shift with growing confidence on the use of stimulated serum thyroglobulin and neck ultrasonography, and decreased use of routine diagnostic whole-body scans, in particular, for low-risk patients. Modern assays for serum thyroglobulin determination with improved sensitivity and the use of recombinant human thyrotropin (rhTSH) for stimulated serum thyroglobulin have made a considerable change in the surveillance protocol of disease recurrence . For practical purposes, thyroglobulin levels should be measured serially with the same method in the same laboratory whenever possible and antithyroglobulin antibodies should be checked in the same sample, because considerable variability has been reported across the methods and antithyroglobulin antibody can cause the assay interference, often giving falsely low thyroglobulin values . Although thyroglobulin is a valuable tumor marker of well-differentiated thyroid carcinoma, its production can be significantly reduced even with endogenous or exogenous TSH stimulation in poorly differentiated tumor . Thyroglobulin measurement should be accompanied by other follow-up modalities, especially in intermediate- and high-risk patients.
Neck ultrasonography has become the principal imaging study in patients with thyroid cancer . Most of the recently updated guidelines view a combination of serum thyroglobulin measurement and routine neck ultrasonography as an excellent follow-up tool for low-risk patients, given its high sensitivity and negative predictive value . Ultrasonography may have a particular role when serum thyroglobulin measurements are unreliable because of the presence of assay interference or poor thyroglobulin production by the tumor. In general, neck ultrasonography is recommended at 6 and 12 months after radioactive iodine remnant ablation, and then yearly for at least 3 to 5 years, depending on the risk for recurrence and the thyroglobulin status of each patient. Because ultrasound evaluation is uniquely operator-dependent, dedicated ultrasonographers specialized in thyroid imaging are preferred to achieve optimum sensitivity and specificity for detection of disease recurrence.
Routine diagnostic whole-body scans have low sensitivity and are usually not needed in low-risk patients who are clinically free of disease with negative stimulated serum thyroglobulin and neck ultrasonography . It may be of some value in the follow-up of patients with intermediate or high risk of recurrent disease. The NCCN guidelines recommend regular diagnostic whole-body scans either with withdrawal of thyroid hormone or rhTSH every 12 months until no radioiodine-avid tumor is evident for patients with detectable thyroglobulin, distant metastases, or soft tissue invasion on initial staging . Because of the concerns over I-131–induced stunning of thyroid cancer, if diagnostic whole-body scans are indicted, the use of I-123 or low-dose I-131 (1–3 mCi) is preferred.
The role of cross-section imaging and 18 FDG PET scanning is less clear for surveillance of disease recurrence. In general, additional nonradioiodine imaging, such as 18 FDG PET scanning with or without CT, is considered for patients whose whole-body scans are negative but thyroglobulin levels are elevated, commonly more than 2 to 5 ng/mL . The 18 FDG PET scanning becomes especially sensitive in identifying recurrence when thyroglobulin levels are greater than 10 ng/mL . CT of neck to detect local disease extension to surrounding structures, such as trachea or esophagus, CT of lungs, and MRI of bones and brain are used as complementary imaging modalities. Iodinated contrast should be avoided if radioiodine treatment is anticipated. Bone scintigraphy is poorly sensitive because most metastatic lesions of differentiated thyroid carcinoma are lytic .
Current guidelines are in agreement on the subject of the general follow-up strategy after initial therapy . Follow-up strategy based on risk stratification is summarized in Fig. 1 . After total thyroidectomy and radioactive iodine remnant ablation followed by posttreatment scans, the initial follow-up in 6 to 12 months comprises neck ultrasonography and suppressed serum thyroglobulin measurements. If either of these tests is positive, the localization studies for persistent or recurrent disease should be pursued. If both the neck ultrasonography and suppressed serum thyroglobulin do not reveal any evidence of disease, low-risk patients can be followed with stimulated thyroglobulin alone, whereas intermediate- and high-risk patients usually require diagnostic whole-body scans along with stimulated thyroglobulin measurement. Thereafter, the disease-free patient can be followed with suppressed thyroglobulin every 6 to 12 months and neck ultrasonography on a yearly basis depending on the risk of recurrence. The timing or necessity of subsequent stimulated testing is uncertain for those found to be free of disease. If thyroglobulin levels are detectable but below the institutional cut-off level (commonly, between 2 and 5 ng/mL after rhTSH stimulation or below 10 ng/mL after thyroid hormone withdrawal) and no other evidence of disease exists, stimulated thyroglobulin measurement and neck ultrasonography should be repeated in 6 to 12 months. An increase of thyroglobulin levels on serial measurements likely indicates a disease progression . In a situation of an elevated thyroglobulin or other abnormalities, the imaging studies are recommended typically with CT of the chest in addition to neck ultrasonography. If imaging is negative for surgically treatable disease, then empiric therapy with radioiodine is considered for possible treatment and to facilitate localization of persistent or recurrent disease on posttreatment whole-body scans. High-risk patients may require additional cross-sectional imaging studies or 18 FDG PET scans because they tend to have disease recurrence with poorly differentiated tumors whose ability to produce thyroglobulin and concentrate radioiodine may be diminished.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


