The majority of recurrent thyroid carcinomas are histologically differentiated and readily diagnosed by light microscopy or immunohistochemical staining. Infrequently, recurrent carcinoma may be less differentiated than the index lesion, creating diagnostic challenges. Complicating issues include thyroid carcinomas that recur years after initial diagnosis or without clinical elevation of serum thyroglobulin. With a favorable outcome and lengthy survival rates after initial diagnosis of differentiated thyroid carcinoma, there is a greater chance for these carcinomas to recur and as less differentiated carcinoma. As more advanced treatment techniques enter daily practice, the pathology of recurrent thyroid carcinomas will be better defined and more readily diagnosed.
Thyroid cancer is the most common primary endocrine malignancy, with an estimated 37,340 new cases each year, accounting for 1590 deaths annually . Classification of thyroid tumors is by cell of origin. The most common thyroid neoplasms, benign or malignant, originate from thyroid follicular epithelial cells and include follicular adenoma, follicular carcinoma, and thyroid papillary carcinoma, and respective variants of these tumor types. The majority of thyroid follicular epithelial cell–derived malignant neoplasms are differentiated cancers. Thyroid follicular epithelial cells give rise, however, to less differentiated thyroid carcinomas, including anaplastic carcinoma and poorly differentiated thyroid carcinomas. Less frequent occurring thyroid neoplasms include those originated from C cells (thyroid medullary carcinoma), lymphoid cells (malignant lymphomas), and mesenchymal cells (sarcomas).
Although there is abundant literature on primary follicular epithelial cell thyroid carcinomas, there is little literature on recurrent thyroid carcinoma. Differentiated thyroid carcinomas have an overall excellent prognosis but recurrence is not uncommon. Follow-up becomes almost a life-long ordeal and pathologic identification of these tumors may be difficult at recurrence because of differing histologies of primary and recurrent tumors.
Thyroid papillary carcinoma
Thyroid papillary carcinoma is the most common primary tumor of the thyroid, accounting for more than 70% of all primary thyroid cancers . Since the Surveillance, Epidemiology and End Results program began recording data in 1988, the incidence of thyroid papillary cancer has increased by 4.1 per 100,000. Despite this increase in incidence, however, the mortality from thyroid papillary carcinoma has remained stable at approximately 0.5 deaths per 100,000 . A long-term study from the Mayo Clinic found the cancer-related mortality to be only 6.5% .
Thyroid papillary carcinomas may show a variety of gross appearances from case to case and even within the same case. These tumors may be wholly solid, wholly cystic, or mixed solid and cystic. Similarly, these tumors may be encapsulated or well circumscribed or they may be infiltrative, usually within the thyroid gland and less often with extrathyroidal extension, including into perithyroidal fat and uncommonly into skeletal muscle and adjacent structures, such as the esophagus, larynx, or trachea. The size of these tumors varies from 1 cm to several centimeters in size but microscopic foci measuring less than 1 cm frequently are seen. These tumors have a firm, white cut surface and can have a gritty texture resulting from the presence of psammoma bodies or even bone formation. Foci of gross necrosis and hemorrhage are uncommon in thyroid papillary carcinoma.
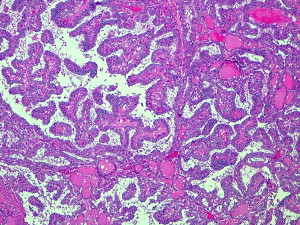
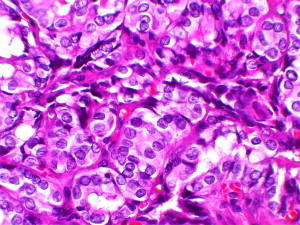
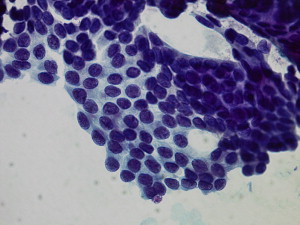
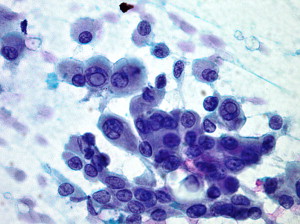
Microscopically, as the name implies, thyroid papillary carcinomas show a papillary architecture so named because of its resemblance to a tree with arborizing neoplastic cells and central fibrovascular cores ( Fig. 1 ). Papillary architecture, however, is not diagnostic for thyroid papillary carcinoma as other lesions, including adenomatoid nodules and untreated diffuse hyperplasia (Graves’ disease), may have papillary architecture. Conversely, the absence of papillary architecture does not exclude a diagnosis of thyroid papillary carcinoma. The diagnostic nuclear findings in thyroid papillary carcinoma include a constellation of changes and not any one finding. The nuclear features diagnostic for thyroid papillary carcinoma include nuclear enlargement with variation in the size and shape of the nuclei, dispersed (very fine) to optically clear-appearing nuclear chromatin, nuclear crowding and overlapping, nuclear grooves, and nuclear pseudoinclusions ( Fig. 2 ). The nuclear grooves are formed by deep in-folding of the nuclear membrane whereas the pseudoinclusions are formed by an invagination of cytoplasm into the nucleus . A diagnosis of thyroid papillary carcinoma is predicated on the nuclear features, which accounts for the reason that this diagnosis potentially can be made by aspiration cytology ( Figs. 3 and 4 ). In contrast, the diagnosis of follicular carcinoma and its differentiating from follicular adenoma is predicated on invasive growth, a finding not present in aspiration cytology.
Thyroid papillary carcinomas include a variety of histologic variants. These variants are diagnosed when certain histologic features dominate the tumor. These variants are determined by growth characteristics, including follicular, macrofollicular, diffuse sclerosing, solid, and cribriform variants; cell types, including oncocytic, clear cell, tall cell, and columnar cell variants; and size, including microcarcinomas. To re-emphasize, the diagnosis of any type or variant of thyroid papillary carcinoma is based on the nuclear features and not growth pattern, cell type, or size. So-called aggressive variants of thyroid papillary carcinoma include diffuse sclerosing, columnar cell, and tall cell variants but biologic behavior and prognosis are based on clinical staging and not on the basis of cell type or growth pattern.
Thyroid follicular carcinoma
In the absence of nuclear alterations diagnostic for thyroid papillary carcinoma, the differential diagnosis for an encapsulated thyroid follicular neoplasm includes follicular adenoma and follicular carcinoma. Differentiation of a benign from malignant follicular neoplasm is not based on nuclear changes as follicular adenomas and follicular carcinomas have similar cytologic findings. Rather, this differentiation is based on whether or not there is invasive growth. Invasive growth includes capsular invasion or lymph-vascular space invasion; the latter must be lymph-vascular spaces outside the main mass in the capsule or beyond the capsule. Follicular carcinoma represents only 5% of primary thyroid cancer . Follicular carcinoma is classified as minimally invasive or widely invasive based on the extent of invasive growth.
Minimally invasive or low-grade follicular carcinoma is more common than widely invasive follicular carcinoma. In contrast to the widely invasive tumors, the minimally invasive carcinomas tend to be grossly well circumscribed or encapsulated. On macroscopic examination, they resemble follicular adenomas. The diagnosis of carcinoma is based on the presence of microscopic evidence of capsular or lymph-vascular space invasion ( Figs. 5 and 6 ). These tumors can be divided further into those minimally invasive follicular carcinomas with capsular invasion only and those minimally invasive follicular carcinomas with lymph-vascular space invasion only or with capsular invasion. Although the overall prognosis for minimally invasive follicular carcinomas is good, those with capsular invasion only are believed to have a better overall prognosis than those minimally invasive follicular carcinomas with lymph-vascular space invasion . Finally, there is controversy among pathologists as to what constitutes capsular invasion, with some authorities requiring complete transgression of the capsule to render this diagnosis whereas other authorities are less restrictive in their definition of what constitutes capsular invasion.
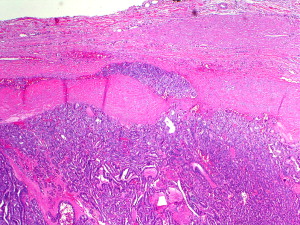
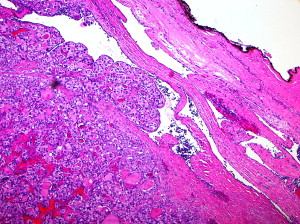
The widely invasive follicular carcinomas are less common than minimally invasive follicular carcinomas. On macroscopic examination, these tumors can show foci of obvious invasive growth. Grossly, the widely invasive tumors are unencapsulated or partially encapsulated with apparent protrusion of tumor into surrounding thyroid parenchyma. The tumors commonly have a firm, white cut surface and may show areas of hemorrhage and necrosis. Microscopically, the widely invasive follicular carcinomas show the presence of tumor extending well beyond a capsular delineation. Often, there is a mushroom-like protrusion of tumor into adjacent thyroid parenchyma. In addition, invasion of larger caliber-sized lymphatic/vascular spaces can be seen. Less frequently, the neoplastic proliferation may invade outside the confines of the thyroid gland with extension into perithyroidal soft tissues or into adjacent anatomic sites.
So-called Hürthle cell carcinoma is a histologic variant of follicular carcinoma and, like all follicular carcinomas, can be minimally invasive or widely invasive. Hürthle cell is a description of a cell with oncocytic cytoplasmic changes resulting from the presence of increased mitochondria. Hürthle cells can be identified in a wide array of thyroid lesions including non-neoplastic lesions (eg, lymphocytic thyroiditis or adenomatoid nodules) and benign neoplasms (eg, follicular adenomas). The presence of Hürthle cells in cytologic specimens or surgical specimens does not equate to a neoplastic proliferation let alone a malignant one. As such, the use of the term, Hürthle cell , is discouraged as clinicians are apt to make the assumption that a thyroid lesion with Hürthle cells is a malignant neoplasm. This is simply not true. Rather than Hürthle cell, a better designation is oncocytic cell, which is purely descriptive and not indicative or misconstrued as a malignant neoplasm. As with other differentiated thyroid carcinomas, staging and prognosis are predicated on extent of disease and not on the basis of cell type (ie, Hürthle cells).
Thyroid follicular carcinoma
In the absence of nuclear alterations diagnostic for thyroid papillary carcinoma, the differential diagnosis for an encapsulated thyroid follicular neoplasm includes follicular adenoma and follicular carcinoma. Differentiation of a benign from malignant follicular neoplasm is not based on nuclear changes as follicular adenomas and follicular carcinomas have similar cytologic findings. Rather, this differentiation is based on whether or not there is invasive growth. Invasive growth includes capsular invasion or lymph-vascular space invasion; the latter must be lymph-vascular spaces outside the main mass in the capsule or beyond the capsule. Follicular carcinoma represents only 5% of primary thyroid cancer . Follicular carcinoma is classified as minimally invasive or widely invasive based on the extent of invasive growth.
Minimally invasive or low-grade follicular carcinoma is more common than widely invasive follicular carcinoma. In contrast to the widely invasive tumors, the minimally invasive carcinomas tend to be grossly well circumscribed or encapsulated. On macroscopic examination, they resemble follicular adenomas. The diagnosis of carcinoma is based on the presence of microscopic evidence of capsular or lymph-vascular space invasion ( Figs. 5 and 6 ). These tumors can be divided further into those minimally invasive follicular carcinomas with capsular invasion only and those minimally invasive follicular carcinomas with lymph-vascular space invasion only or with capsular invasion. Although the overall prognosis for minimally invasive follicular carcinomas is good, those with capsular invasion only are believed to have a better overall prognosis than those minimally invasive follicular carcinomas with lymph-vascular space invasion . Finally, there is controversy among pathologists as to what constitutes capsular invasion, with some authorities requiring complete transgression of the capsule to render this diagnosis whereas other authorities are less restrictive in their definition of what constitutes capsular invasion.
The widely invasive follicular carcinomas are less common than minimally invasive follicular carcinomas. On macroscopic examination, these tumors can show foci of obvious invasive growth. Grossly, the widely invasive tumors are unencapsulated or partially encapsulated with apparent protrusion of tumor into surrounding thyroid parenchyma. The tumors commonly have a firm, white cut surface and may show areas of hemorrhage and necrosis. Microscopically, the widely invasive follicular carcinomas show the presence of tumor extending well beyond a capsular delineation. Often, there is a mushroom-like protrusion of tumor into adjacent thyroid parenchyma. In addition, invasion of larger caliber-sized lymphatic/vascular spaces can be seen. Less frequently, the neoplastic proliferation may invade outside the confines of the thyroid gland with extension into perithyroidal soft tissues or into adjacent anatomic sites.
So-called Hürthle cell carcinoma is a histologic variant of follicular carcinoma and, like all follicular carcinomas, can be minimally invasive or widely invasive. Hürthle cell is a description of a cell with oncocytic cytoplasmic changes resulting from the presence of increased mitochondria. Hürthle cells can be identified in a wide array of thyroid lesions including non-neoplastic lesions (eg, lymphocytic thyroiditis or adenomatoid nodules) and benign neoplasms (eg, follicular adenomas). The presence of Hürthle cells in cytologic specimens or surgical specimens does not equate to a neoplastic proliferation let alone a malignant one. As such, the use of the term, Hürthle cell , is discouraged as clinicians are apt to make the assumption that a thyroid lesion with Hürthle cells is a malignant neoplasm. This is simply not true. Rather than Hürthle cell, a better designation is oncocytic cell, which is purely descriptive and not indicative or misconstrued as a malignant neoplasm. As with other differentiated thyroid carcinomas, staging and prognosis are predicated on extent of disease and not on the basis of cell type (ie, Hürthle cells).
Recurrent differentiated thyroid carcinoma
Locally recurrent differentiated thyroid carcinoma is not uncommon, with recurrence rates ranging from 5% to 20% in patients who have thyroid papillary carcinoma and 25% to 73% in patients who have widely invasive follicular and Hürthle cell carcinomas . Some patients ultimately succumb to recurrent disease .
The histology of recurrent (and for that matter metastatic) differentiated thyroid carcinoma in the majority of cases is similar to that of the primary carcinoma. Recurrent (and metastatic) thyroid carcinoma may transform, however, to less differentiated types, thereby presenting a diagnostic challenge to surgical pathologists, especially if clinical information is lacking or a pathologist is unaware of a history of differentiated thyroid carcinoma. Detailed clinical information provided to pathologists assists in avoiding such potential diagnostic difficulties. Harada and colleagues found that in 59% (36 of 61) of cases of metastatic thyroid carcinoma, the metastatic lesion had differing histology than the primary carcinoma. Goretzki and colleagues reported that in approximately one third of patients in their series, the histology of the recurrent lesion was less differentiated tumor than the primary carcinoma. In some patients, the recurrent carcinoma may occur years after the initial presentation, further complicating the diagnosis of recurrent disease, especially if the recurrent lesion is a less differentiated carcinoma . Under most circumstances, immunohistochemical staining is specific for differentiated thyroid carcinomas. These lesions are uniformly immunoreactive with a variety of cytokeratins including (but not limited to) pancytokeratin (eg, AE1/AE3), low molecular weight cytokeratin (eg, CAM5.2), and other cytokeratins (eg, CK7, others). Cytokeratin immunoreactivity, however, is not specific or sensitive relative to differentiated thyroid follicular epithelial cell–derived carcinomas. Thyroid medullary carcinoma, a neuroendocrine carcinoma of the thyroid gland, also is immunoreactive with a wide variety of cytokeratin stains. Thyroglobulin represents a specific and sensitive marker for differentiated thyroid follicular–derived neoplasms, being uniformly reactive in the overwhelming majority of thyroid papillary carcinomas, thyroid follicular carcinomas, and respective variants of these tumor types. Thyroglobulin immunoreactivity also represents an excellent marker in the presence of recurrent (and metastatic) differentiated thyroid carcinomas. Thyroglobulin is not reactive in thyroid medullary carcinoma, nonfollicular epithelial cell neoplasms of thyroid origin, and metastatic tumors to the thyroid gland from a remote primary malignancy. The less differentiated any neoplasm becomes, however, the less antigenicity is retained so that a recurrent (or metastatic) thyroid carcinoma that has less differentiated histologic features may show a marked decrease in the presence of thyroglobulin reactivity or even complete absence of thyroglobulin reactivity. This is further reason why detailed clinical information always should be provided to surgical pathologists. Thyroid transcription factor 1 (TTF1) is an immunomarker used in the diagnosis and differential diagnosis of thyroid carcinomas. In contrast to thyroglobulin (and cytokeratins), which are cytoplasmic in their localization, TTF1 is a nuclear stain. Although TTF1 is an excellent marker for differentiated thyroid follicular epithelial cell–derived carcinomas, it also is found in other tumor types, including thyroid medullary carcinoma. Further, similar to thyroglobulin, once a carcinoma becomes less differentiated there may be a marked decrease to complete absence of TTF1 immunoreactivity.
Less frequently, recurrent differentiated thyroid carcinomas recur with histologic features more characteristic of poorly differentiated carcinomas characterized by solid growth, absence of colloid or colloid-filled follicles, marked nuclear pleomorphism, necrosis, and increased mitotic activity, including atypical mitoses . Although therapy for differentiated thyroid carcinoma typically includes a total thyroidectomy, recurrent carcinoma in glands not totally resected may include the presence of extranodal invasion. Zbären and colleagues reported five patients all of whom had extrathyroidal extension of recurrent carcinoma into the larynx necessitating total laryngectomy. In two of the five patients, the primary (nonrecurrent) carcinomas were differentiated thyroid carcinomas .
Recurrence of follicular carcinomas is closely associated with degree of invasion. Minimally invasive follicular carcinomas have an extremely low rate of recurrence and metastases. Thompson and colleagues reported 95 patients who had only partial- or full-thickness capsular invasion and only three patients developed recurrence or metastatic disease. Loh and colleagues found a higher risk for recurrence but not death in patients who had multifocal tumors.
Follicular carcinomas with angioinvasion at the initial diagnosis have a significantly increased propensity to be clinically aggressive . Some studies have found that up to 50% of patients who had angioinvasive follicular carcinomas had a recurrence or distant metastases . Such potential aggressive biologic behavior, however, usually does not occur in minimally invasive follicular carcinoma with capsular invasion only but tends to be restricted to those follicular carcinomas in which invasion includes (or may be limited to) angioinvasion. Further, there is an ongoing debate in the pathology literature regarding determination of quantitative criteria relative to angioinvasion, with some authorities indicating that greater risk for aggressive behavior occurs when there is invasion of four or more blood vessels . To date, there are no absolute reports identifying a quantitative basis for reporting the extent of angioinvasion, but this issue requires further clarification.
The treatment for recurrent, less-differentiated thyroid carcinomas may be problematic. Thyroid tumorigenesis may be associated with progressively more aggressive histology and loss of thyroid-specific functions . During the dedifferentiation process, these tumors lose thyroid-specific genes leading to a loss of thyroid-specific functions. These genetic losses result in a decreased response to thyroid cancer–specific treatments, such as radioactive iodine . This has led research into the usefulness of redifferentiation therapy. Several redifferentiating agents have been found tentatively effective in thyroid cancer cells. Agents, such as retinoids, aromatic fatty acids, and peroxisome proliferator-activated receptor gamma agonists, are of particular interest . In vitro, in vivo, and some clinical trials suggest that these new medical treatments may benefit patients who have poorly or undifferentiated types of thyroid cancer .
Lymph nodes are one of the most common sites for thyroid papillary carcinoma to recur or metastasize ( Fig. 7 ). Furlan and colleagues originally found lymphatic/vascular invasion to have no affect on prognosis. This finding was refuted in other reports, however . Although these pathologic findings are important, location also may have an impact on recurrence. Beasley and colleagues found that patients who had lateral neck lymph node metastases at presentation had higher rates of recurrence. Dedifferentiation of thyroid carcinoma can occur in association with lymph node recurrence/metastasis and distant metastases .



