Conventional thyroid surgical techniques, introduced 100 years ago, continue to be applied in modern endocrine surgery practices. Minimally invasive approaches, however, have been proposed by Miccoli and others, and have been increasingly embraced. Reoperative thyroidectomy poses special challenges for even the expert surgeon, and these challenges are no less important when undertaking minimally invasive surgery. Nevertheless, the authors’ experience with reoperative minimally invasive thyroid surgery would suggest that this approach is not only safe and effective, but confers many of the same advantages as primary minimally invasive surgery (particularly superior cosmetic results and rapid wound healing leading to early discharge). When applied judiciously, reoperative minimally invasive thyroid surgery offers advantages over conventional surgery and is an appropriate component of a high-volume head and neck endocrine practice.
The advent of minimally invasive surgical techniques has ushered in an era in which surgery is less painful and is associated with better cosmetic results. Since Mouret performed the first laparoscopic cholecystectomy in 1987, similar techniques have populated most surgical fields, with oncologic outcomes and complication rates that are comparable to conventional surgery. The benefits seen in intra-abdominal surgery are readily apparent, with shorter hospital stays, reduced scarring, and decreased pain. Although not as dramatic, similar advantages have been realized with minimally invasive head and neck surgery, particularly with minimally invasive thyroidectomy .
Various approaches to the minimally invasive thyroidectomy have been proposed, but the most widely practiced by far has been the minimally invasive video-assisted thyroidectomy (MIVAT), described by Miccoli and colleagues from Pisa. This technique has proved to incur not only reduced pain and superior voice outcomes , but also an improved cosmetic appearance, which is particularly important because thyroid diseases preferentially affect younger women, for whom aesthetics are generally important.
In some clinical circumstances, reoperation in the thyroid compartment may be necessary. Reoperative thyroid surgery poses certain challenges (related to inflammation and fibrosis) that are no less important when considering minimally invasive surgery. The authors sought to determine whether a minimally invasive approach is safe and effective in patients who require reoperation in the thyroid compartment.
Methods and materials
A retrospective analysis was undertaken of patients undergoing thyroidectomy in the Medical College of Georgia Department of Otolaryngology between January 2004 and July 2007. In each of 24 reoperations, one of two minimally invasive approaches was used. The demographic and clinical data, including age, gender, indications for surgery, incision length, duration of surgery, blood loss, and complications, were reviewed and analyzed. Institutional Review Board approval to perform the data retrieval and analysis was sought and obtained.
Surgical techniques
Minimally invasive (endoscopic)
Minimally invasive (endoscopic) surgery has been described in detail previously, and video clips demonstrating the major steps of the procedure are available online . Reoperative surgery is customized to the specific patient characteristics.
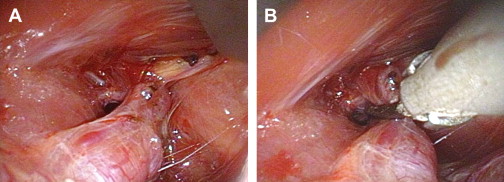
Briefly, while the patient is sitting up in the holding area, a 15- to 20-mm horizontal cervical marking is made in a natural skin crease approximately one fingerbreadth above the sternal notch. The procedure is performed with the patient in the supine position under general or local-regional anesthesia. After the patient is injected with local anesthesia, the incision is made and carried down through the subcutaneous tissues to expose the strap muscles. The midline raphe is separated and the strap muscles on the side of the intended surgery are dissected away from the thyroid gland. Mobilization lateral around the thyroid gland is accomplished using blunt elevators (Terris elevators, Medtronic-ENT, Jacksonville, Florida). At this point, the room lights are darkened and a 5-mm 30° laparoscope is used to visualize the superior pole of the thyroid gland. Harmonic-ACE shears (ACE23P, Ethicon Endo-Surgery, Cincinnati, Ohio) are used to divide the superior pedicle as a single bundle (This approach to managing the superior pole vessels is a more recent one and is illustrated in Fig. 1 ). The superior parathyroid gland is identified and dissected away from the thyroid.
Attention is directed inferiorly, and the recurrent laryngeal nerve (RLN) is identified and traced for a distance of approximately 20 to 30 mm. The inferior parathyroid gland is identified and dissected away from the thyroid. The gland is exteriorized with the use of hemostat clamps placed directly on the superior pole. The RLN is traced to its entrance at the cricothyroid joint, as the Harmonic-ACE shears are used to ligate vessels and divide tissue.
The wound is copiously irrigated, hemostasis is assured, and Surgicel is placed in the thyroid bed. The strap muscles are closed with a single figure-of-eight suture of 3-0 Vicryl, the subcutaneous tissues are closed with a single suture of 4-0 Vicryl, and the skin is reapproximated with Dermabond. Drains are not required and skin sutures are avoided. Most patients are discharged to home after a short stay in the recovery room .
Minimally invasive (nonendoscopic)
Minimally invasive (nonendoscopic) surgery is performed through a 2- to 6-cm horizontal cervical incision (depending on the clinical circumstances), one fingerbreadth above the sternal notch. After transection of the platysma, the strap muscles are retracted laterally, exposing the thyroid gland (note that subplatysmal flaps are not raised). The gland is removed in a fashion similar to that described earlier, except that endoscopes are not necessary to visualize and ligate the superior pole, or to identify the RLN. It is sometimes desirable to deliver the gland early (after ligating the superior pole) to facilitate identification of the RLN.
Results
Twenty-four minimally invasive reoperative thyroidectomies were performed in the Medical College of Georgia Department of Otolaryngology between January 2004 and July 2007. The study included 21 female patients and 3 male patients, with a mean age of 44.2 ± 14.0 years (standard deviation). The most common indication for reoperation was to accomplish a contralateral lobectomy when a follicular neoplasm was determined to be an invasive follicular carcinoma on pathologic examination (6 of 24), representing 25% of patients.
The time between the primary and reoperative surgeries ranged from 4 days to 22 years, with a median of 357.5 days. The incision length ranged from 20 to 50 mm, with a median of 39.4 mm. The median blood loss was 10 mL, with a range of 0 to 30 mL. The duration of surgery ranged from 59 to 173 minutes, with a mean of 92.9 ± 26.7 minutes. All patients were managed without the use of a drain perioperatively. In one patient, wound edema prompted a 1-day hospitalization. A second patient developed a pulmonary embolism 4 days after the operation and was hospitalized for a day to accomplish anticoagulation. No other complications occurred, and all other patients were managed on an outpatient basis. Representative photographs from a patient managed with a reoperative endoscopic thyroidectomy are shown in Fig. 2 .




