CHAPTER 117 Ultrasound Imaging of the Neck
Basics of Ultrasound
One should be familiar with terminology used in US imaging. B-mode sonography refers to a gray-scale mode, where Doppler sonography is used for assessment of blood flow and is color coded. Echogenicity defines the appearance of tissues on the US image relative to its ability to reflect the US wave. Anechoic means no return signal; it represents complete penetration of the energy through a structure, appearing black. An isoechoic object has similar echogenicity to surrounding tissue. Hypoechoic tissue has lower echogenicity than reference tissue, appearing darker. Hyperechoic tissue is brighter compared with the reference structure due to higher echogenicity.1
Utility and Limitations
The majority of structures and pathologies in the neck are located within 5 cm distance from the skin surface. With high-resolution sonographic technology, virtually all extracranial structures can be accurately assessed, though the primary utility is imaging of thyroid, parathyroid, and salivary glands, as well as lymph nodes. Magnetic resonance imaging (MRI) or computed tomography (CT) scans generally offer no additional information regarding size, margin, or malignant potential.2 Being relatively inexpensive, office-based US technology is readily available, portable (size of laptop computer), quick and easy to perform, and harmless to the patient. It also allows real-time diagnostic imaging and image-guided fine-needle biopsy to be performed at the same visit. It does not involve ionizing radiation or require intravenous contrast.
Ultrasonography should be the first imaging modality for evaluation of thyroid nodular disease. The limitations of US include difficulty assessing deep soft tissue and bony invasions and inability to penetrate through bone or cartilage. It cannot reliably evaluate perineural spread, involvement of the skull base, or parapharyngeal/retropharyngeal/mediastinal nodes.4
Operator dependence is one of the major limitations of ultrasonography. Mastering office-based sonography by a surgeon who knows the anatomy, patient, and disease eliminates reliance on someone else’s reporting, provides better real-time preoperative localization, assesses related lymphadenopathy, permits single operator consistent follow-ups with image-based documentation, assists more accurate specimen acquisition, and adds another dimension to physical examination.3,5,6
Brief Description of Technique
It is important to develop a readily replicated, systematic approach for the examination of neck structures. We prefer to use B-mode (gray-scale) scanning in the transverse/axial plane primarily. Starting inferiorly in the lateral neck, the probe is tilted inferiorly to visualize the subclavian vessels and then steadily advanced in superior direction with the carotid along the medial aspect of the field of view. The examination is then repeated on the contralateral side.6,7
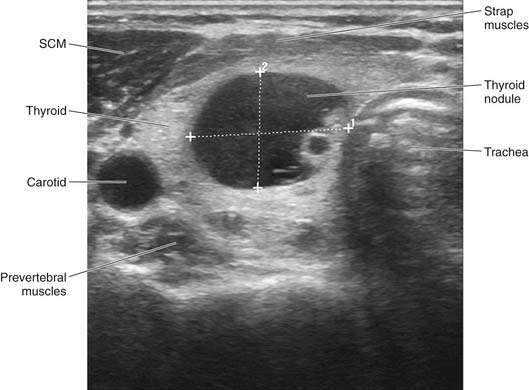
For central compartment evaluation, one half of the trachea should be visible on the medial aspect of the screen and the great vessels visible laterally, proceeding inferiorly to superiorly. A light touch will minimize compression of the jugular vein. Longitudinal/sagittal imaging is less intuitive; thus it is mostly reserved for confirmation and sizing in the cranial-caudal dimension of selected pathology once it is identified. For subtle changes in position, the probe can be slightly tilted back and forth, which allows more precise movement than sliding the probe along the skin surface. Color Doppler imaging can be used to assess vascularity, though most vessels are readily distinguished in gray scale. Once an image is localized in real time, the image can be frozen, labeled, sized, saved, and printed for the patient’s file (Fig. 117-1).8
Thyroid Ultrasound
US provides the most accurate sizing of nodular disease for surveillance, and its sensitivity for detection of thyroid malignancy approaches 80% to 90% in experienced hands.9,10
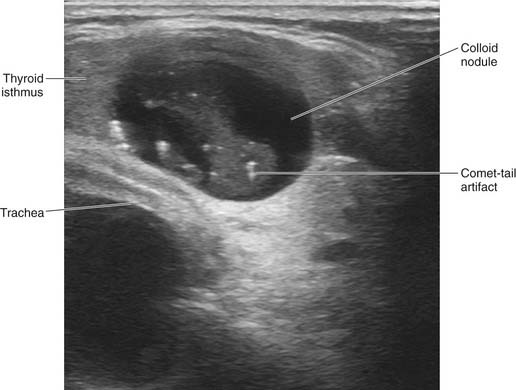
In the setting of a multinodular thyroid, it is important to carefully evaluate each nodule individually and target which sonographic features increase the predictive value of fine-needle aspiration (FNA) for carcinoma. Although there is no single pathognomonic sonographic feature, the constellation of findings may suggest malignancy: microcalcifications, intranodular intrinsic vascularity, absent “halo sign,” extraglandular extension, and irregular or microlobulated margins (Fig. 117-2, Box 117-1). Unless purely cystic, the presence of cystic component within a lesion does not diminish risk of carcinoma, and is common in papillary carcinomas. One should be aware of inspissated colloid as a common misinterpretation for microcalcifications. The presence of a comet-tail or ring-down artifact posterior to the echogenic foci is seen with colloid (Fig. 117-3). We still perform a biopsy of the largest nodule in spite of benign sonographic features, but will select other nodules for biopsy that appear suspicious independent of size alone.11,12
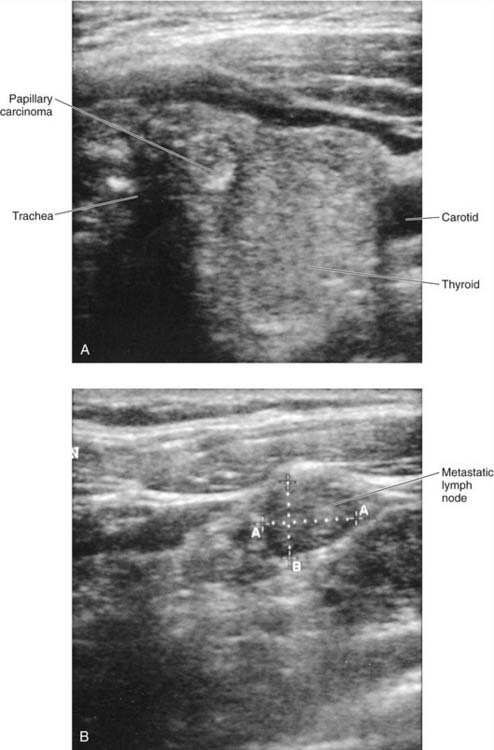
In addition to evaluation of the thyroid gland, cervical lymph nodes must be carefully examined, especially in patients suspected of having malignancy.13 Sonographic identification of round, enlarged, hypoechoic, solid or cystic lymph nodes with microcalcifications and absent echogenic hilum should raise suspicion of papillary or medullary thyroid carcinoma (Fig. 117-4
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


