Tympanic Membrane Structure
The tympanic membrane is composed of two parts, the pars flaccida and the pars tensa. The layers of the pars tensa (external to internal) are as follows1: epidermal layer of keratinizing squamous epithelium, connective tissue layer, and a single layer of mucosal cells.2 The epidermis is three to five cell layers thick and lacks skin appendages.3 The connective tissue layer is well developed and includes two main layers of fibers, an outer radial layer and an inner circular layer. There is a very thin layer of oblique fibers running in between these two layers of fiber.4 The mucosal layer of the tympanic membrane, composed of ciliated columnar epithelial cells, is continuous with that of the middle ear cavity.5 The pars flaccida, by comparison, contains a higher proportion of elastic fibers, lacks the organized separate connective tissue layers of the pars tensa, and lacks cilia on its mucous membrane.3
3.1.2 The Migratory Epithelium of the Tympanic Membrane and External Ear Canal
In humans, the epidermis migrates centripetally from the umbo and then outward to the external meatus (▶ Fig. 3.1),6,7 facilitating a self-cleaning mechanism for the ear canal.3 This process was first described by Burnett (1877) and later confirmed by Stinson (1936), Litton (1963),7 Alberti (1964),6 and Franz (1966).8 The epithelia migrate at an average of 70–131 microns per day6,9 with some diurnal variation.10 The epithelial progenitor cells of the tympanic membrane responsible for this migration are likely to be located at the umbo and along the malleus.11,12 Progenitor cells in the annulus are more likely to have a role in repair. Migration occurs via a plane of separation between more superficial cells sliding over ones below. The presence of intercellular spaces, cytoplasmic processes, and smaller numbers of desmosomes (points of intercellular adhesion) in the stratum basale and stratum spinosum suggest that this is the plane in which migration occurs, along with movement on the basement membrane.13,14 The speed of migration is relatively slower in the anterior and inferior quadrants.15 Migration pathways spread outward from the tympanic membrane and out the external auditory canal to the bony cartilaginous junction, where desquamation occurs.6
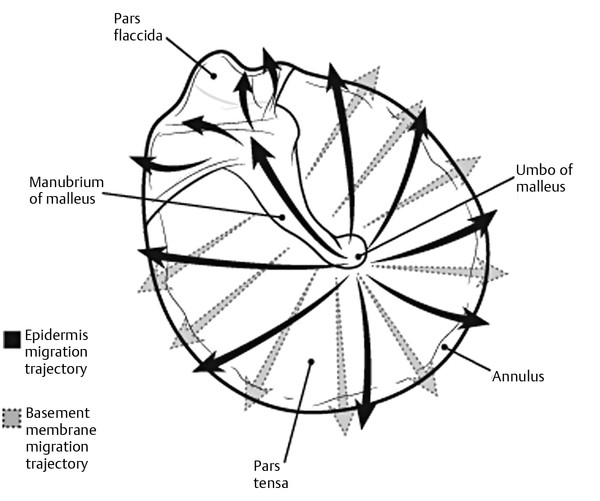
Fig. 3.1 The epithelial migration pattern of the tympanic membrane. The usual pattern of migration is marked in a solid line, with the alternate pathway seen in approximately 20% of subjects shown in broken lines. The migration pattern exactly at the umbo is directly up the handle of the malleus before fanning out radially.
Tympanic membrane migration can be affected by patient factors, including age, with children shown to have migration predominantly in a posterior-superior direction.6 Animal studies show that older animals demonstrate slower migration.16 In the presence of otitis media, the mitotic activity over the whole tympanic membrane increases.17
The migratory mechanisms are likely to involve a reduction in intercellular adhesion between layers of migratory cells.18 The interaction between cell adhesion molecules is complex and includes selectins, desmocolin, F actin, fibronectin, integrin β-1, and cadherin-6.19 Hemidesmosomes link keratin filaments of the basal layer to the underlying basement membrane and must be disassembled so that keratinocyte migration can occur.20 The α3-β1 and α6-β4 integrins are important for maintaining the directional trajectory of cutaneous keratinocyte migration21, and are likely to be important in tympanic membrane migration.
3.2 Tympanic Membrane Perforation
3.2.1 Etiology of Tympanic Membrane Perforation
Tympanic membrane perforations most commonly result from otitis media or trauma. Perforations associated with otitis media are typically small and usually heal spontaneously upon resolution of the infection. Ongoing infection may prevent a perforation from healing and is more common in developing countries, poor socioeconomic groups, and children.22 During acute infection, the middle ear becomes full, with exudate putting pressure on the tympanic membrane, causing it to bulge outward. This pressure causes the central area to become ischemic and give way.22 Traumatic causes include blunt injury, penetrating injury, barotrauma, and acoustic pressure (occurs between 195 dB and 199 dB at 30°C, with more sound pressure required at lower frequencies). Heat, corrosives, lightning, and water sports have the lowest incidence of spontaneous closure.23
3.2.2 Tympanic Membrane Wound Healing
The tympanic membrane is unique in that it is a structure suspended in air.22 Repairing cells therefore have to bridge a gap. Unlike other wounds, there is no ready-made bed over which the cells can migrate24 and no influx of reparative cells, nutrients, and fibroblasts as found in other epithelial healing.25,26 Tympanic membrane perforations typically heal within 7–10 days.27 The spontaneous healing rate of traumatic perforations is close to 80%.23 Clinically, a perforation may be described as chronic when stable and present for 3 months. It can be divided into the following stages (▶ Fig. 3.2).28
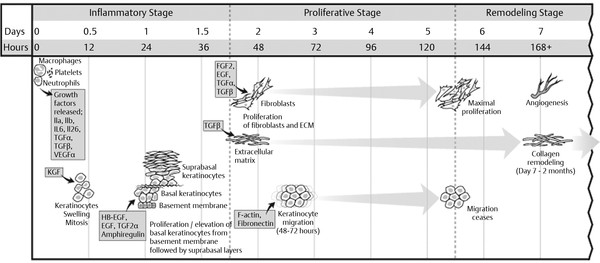
Fig. 3.2 Summary of the major events leading to perforation closure in the tympanic membrane. Wound healing in the tympanic membrane is divided into three stages, with keratinocyte migration beginning as early as 48 hours following perforation.
The Inflammatory Stage (0–48 hours)
After acute injury, an acute inflammatory response occurs, with an exudate composed of interstitial fluid, lymph, and blood accumulating at the perforation margin. A crust layer forms, containing wound debris, providing a medium for the healing process. Within 12 hours the increased vascularity of the tympanic membrane can be observed along the handle of the malleus, the malleolar ligaments, and the annulus.14 Mitotic activity can be demonstrated histologically 10–12 hours following perforation.29,30
The Proliferative Stage (48 hours to days 5–7)
Two days after perforation, the epithelium begins to migrate and the epithelia of the surrounding tympanic membrane becomes elevated from the connective tissue layer, with advancement of the wound edge beginning at 48–72 hours.29,31,32,33 Perforation closure mainly occurs via proliferation of the epidermal layer from a distant origin, predominantly at the attachment of the tympanic membrane to the handle of malleus.14,17 There is a small amount of local mitotic activity at the wound edge, but it occurs later in the process and is less intense.22 Basal keratinocytes first spread and migrate, then proliferate, followed by migration of suprabasal keratinocytes.25,34 Supporting granulation tissue beneath the proliferating squamous epithelium is a prerequisite for perforation closure. Without it, the epithelium shows only local hyperplasia and thickening without closure. The advancing keratinizing squamous epithelium occurs ahead of ingrowing connective tissue,35 that is most pronounced on day 5, just prior to closure.36 It is theorized that the rate of tympanic membrane closure is determined by the rate of advancement of the fibrous layer.37
Keratin was initially thought to act as a scaffold for the epithelium; however, it is not necessary for repair and is probably more a byproduct of the keratinocytes.14 The mucosal cell layer could possibly provide a one cell–thick scaffold across the wound, with the other cells migrating over this.38 The perforation is generally macroscopically closed by 5–7 days,31 with pinpoint perforations often closing sooner than 4 days.9,24 The final layer to migrate across the perforation, the connective tissue layer, may fail to migrate, leaving the perforation closed by two layers, not three (thin segment).22
The Remodeling Stage
After the perforation is closed macroscopically, the remodeling stage occurs, with the content of this area reducing over the next 7 days. The epithelium at this time is 3 or 4 times thicker than the uninjured tympanic membrane, taking approximately 2 months to return to a normal thickness.30 The epithelium is of normal appearance, but the connective tissue layer is still thicker than normal, with a disorganized collagen framework and persistence of giant cells.29,35 There is a macroscopically visible scar up to 6 months following perforation.
3.2.3 Pars Flaccida Healing
Perforations in the pars flaccida differ from the pars tensa in that they show greater exudation and bleeding. They show fibrous layer proliferation on the first day with no epithelial retraction. Epithelial proliferation is only seen around the perforation near the annulus, with none near the handle of the malleus.39 Perforations in the pars tensa do not cause changes in the pars flaccida, whereas perforations in the pars flaccida cause epidermal hyperplasia in the pars tensa.39
3.2.4 Key Growth Factors in Tympanic Membrane Wound Healing
Immunohistochemical studies and microarray research have identified important growth factors in the healing of the tympanic membrane following perforation (▶ Table 3.1). Growth factors often require the presence of other growth factors, with little or no effect on their own.19 Although the mechanisms are multifactorial, the largest number of upregulated genes following injury are from the cystatin family, which are involved in epidermal development.19
Growth factor | hours | day | |||||||
12 | 24 | 36 | 2 | 3 | 4 | 5 | 6 | 7 | |
KGF | ↑↑ | ↓↓ | ↑ | – | ↑ | ↑ | ↑ | ↑↑ | – |
FGF2 | ↓ | ↓ | ↑ | ↑↑ | – | – | – | – | – |
HB-EGF | ↑↑↑↑ | ↓ | – | ↑ | – | – | ↓ | ↑ | – |
EGF | ↓ | ↓ | ↓ | – | – | – | ↑ | ↓ | – |
VEGFa | ↑↑ | – | – | – | – | – | – | – | – |
TGFα | ↑ | ↓ | – | – | – | – | – | ↓ | ↓ |
TGFβ | ↑ | ↑ | – | – | – | – | – | – | – |
HA | ↑ | – | – | – | ↑ | ↑ | ↑ | ↑ | – |
BMP6 | ↓↓ | – | – | – | – | – | – | – | – |
IL1a | ↑↑ | ↓ | ↑ | ↑ | ↑ | – | – | – | ↑ |
IL1b | ↑↑ | – | – | ↓ | – | – | ↑ | ↓ | – |
IL6 | ↑↑↑ | ↓ | – | – | – | – | – | – | ↓ |
IL24 | ↑↑↑↑ | – | – | ↓ | – | – | – | – | ↓ |
a Tympanic membrane wound healing relies on the expression of key growth factors with specific timing. Usually the gene expression precedes the detection by immunohistochemistry by 12–24 hours. Some growth factors, such as PDGF, do not significantly change their expression, but the receptor expression can change dramatically. Data from Santa Maria PL, Redmond SL, McInnes RL, Atlas MD, Ghassemifar R. Tympanic membrane wound healing in rats assessed by transcriptome profiling. Laryngoscope. 2011;121(10):2199–2213. doi: 2110.1002/lary.22150. Epub 22011 Sep 22114. | |||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


