The major advantages of the canal wall reconstruction (CWR) procedure are that it provides the improved exposure to eradicate disease afforded by canal wall-down techniques and, when reconstructed, it provides a near-normal middle ear space, eliminates the need for routine bowl cleanings, allows patients to swim, and, aesthetically, does not require a large meatoplasty. Recurrence rates are low with CWR because blocking the attic physically prevents retraction of the tympanic membrane and obliterating the mastoid removes gas-absorbing mucosa.1
38.2 Patient Selection
Canal wall reconstruction is indicated for patients with cholesteatoma that extends into the epitympanum or mastoid and is not amenable to transcanal procedures such as tympanoplasty or atticotomy. Both congenital and acquired cholesteatomas in patients of any age can be treated with this technique. Canal wall reconstruction can be used to treat recurrent cholesteatoma in patients with prior mastoidectomy as long as the canal wall is intact and the lateral portion of the canal wall has not been lowered. Canal wall reconstruction can also be used to treat disease in patients with facial paralysis, labyrinthine fistula, encephalocele, or extensive scutal erosion. The inability to remove cholesteatoma from the mastoid air cells, such as in severe mastoid cholesteatosis, represents the major contraindication for the CWR technique.
38.3 Surgical Technique
38.3.1 Patient Preparation
The patient is given perioperative antibiotics to cover pseudomonas infection (typically piperacillin-tazobactam and ciprofloxacin). Pediatric patients are not given fluoroquinolones. Penicillin-allergic patients are given clindamycin and ciprofloxacin. The area posterior and superior to the auricle is shaved about 2 cm into the hairline. A C-shaped incision just inside the hairline is marked and injected with approximately 10 mL of 1% lidocaine with 1:100,000 epinephrine.
38.3.2 Incision and Collection of Bone Pate
The incision is made inside the hairline and carried down to the level of the temporalis fascia superiorly. The postauricular skin is carried forward in this plane, leaving the mastoid periosteum down. An anteriorly based musculoperiosteal (Palva) flap is incised along the temporal line and curved down to the mastoid tip. The Palva flap is elevated off the mastoid cortex. However, if there is a cortical mastoid defect from prior surgery or from cholesteatoma, this step is delayed until bone paté is collected. The temporalis muscle and the posterior musculoperiostium are elevated. Bone paté is obtained by drilling the occipital and temporal cortex with a large cutting burr and suctioning the paté through a screen collector attached to the suction (Otomed Corporation, Lake Havasu City, Arizona). Paté collection is limited to the cortical bone and stops if the mastoid air cells are entered or when there is approximately 10 mL of paté. The paté is soaked in 50,000 units bacitracin diluted with 10 mL of Ringer’s solution until needed at the reconstructive portion of the case.
38.3.3 Mastoidectomy
Next, an intact canal wall cortical mastoidectomy with facial recess is performed. The posterior canal wall should not be lowered (medialized) or violated. Cholesteatoma and diseased air cells in the sinodural angle, mastoid tip, and retrofacial areas are removed. The facial recess is opened inferiorly, leaving the facial nerve covered with bone to protect it, as the saw blade will start in the facial recess. The incus and head of the malleus are removed.
The patient is then rotated toward the surgeon, and the external canal skin is elevated off the posterior, superior, and inferior ear canal down to the annulus. The annulus is elevated, and the tensor tympani tendon is cut. The canal skin and anterior drum remnant are pushed anteriorly.
38.3.4 Canal Wall Cuts
A microsagittal saw is used to cut out the posterior canal wall in a manner that, when reconstructed, will prevent it from collapsing into the mastoid. There are two cuts superiorly at 90 degrees to each other (▶ Fig. 38.1). The first cut runs posterior to anterior and parallel to the tegmen/temporal lobe. The second cut is perpendicular to the first, starting in the external canal and running toward the tegmen/temporal lobe. The inferior cut is a compound miter (angled and beveled) starting in the inferior facial recess and running laterally (▶ Fig. 38.1). It is important to bevel the cut from medial to lateral and posterior to anterior so that when the canal wall is replaced, it does not collapse back into the mastoid.
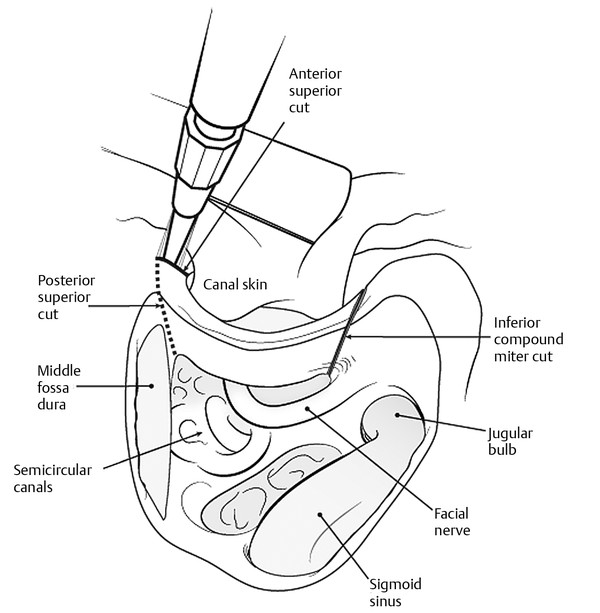
Fig. 38.1 Canal wall cuts. First, the posterior-superior cut is parallel to the middle fossa dura and bony tegmen. The second cut (anterior-superior) is made at a 90-degree angle to the tegmen. Finally, the inferior compound miter cut is made from medial to lateral. This beveled and angled cut prevents the replaced canal bone from falling into the mastoid after reconstruction.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


