Although there are numerous procedures for external auditory canal wall reconstruction after its removal during cholesteatoma surgery, the soft-wall canal reconstruction (SWCR) technique, first reported by Smith et al in 1986,1 is now quite popular (especially in Japan) due to its characteristic features and clinical versatility. The process of SWCR comprises canal wall-down mastoidectomy followed by reconstruction of the external auditory canal wall defect using only soft tissues, such as a remnant of the external auditory canal wall skin and a piece of temporalis fascia (▶ Fig. 39.1).
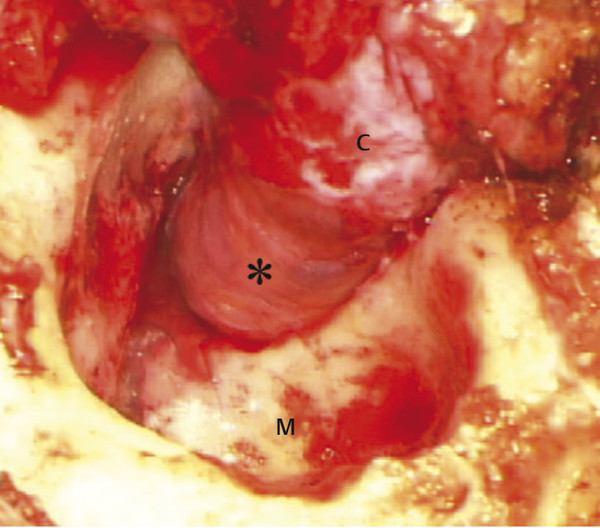
Fig. 39.1 Intraoperative view of SWCR (right ear). Defects in the posterior canal wall skin (C) and tympanic membrane are reconstructed only with a piece of temporalis fascia (asterisk). M, mastoid cavity.
39.2 Patient Selection
Any patient undergoing removal of all or part of the external auditory canal wall may be a candidate for SWCR. Additionally, SWCR can be used in cases of non-inflamed ears, such as surgery for facial decompression, cochlear implantation, and ossiculoplasty for congenital or traumatic ossicular disruption.6
Contraindications to this procedure would be cases that require reconstruction of both the anterior and posterior canal wall using free skin grafts, such as surgery for lateralization of the eardrum. In those cases, if all the directions of the ear canal (360 degrees) were reconstructed by a soft tissue, stricture and shrinkage would ensue.
The generally recognized advantages of SWCR include a wide surgical view, similar to that of the canal wall-down procedure; less required time and effort for fitting and trimming of material, unlike hard-tissue reconstruction; and a shorter time for wound healing as the area of the open wound is far smaller than with the canal wall-down procedure. Also, SWCR uniquely allows the status of the underlying mastoid mucosal function to naturally determine the ultimate contour of the healed ear canal as the soft wall either remains in a canal wall-up configuration or gradually retracts into a radical cavity canal wall-down configuration.
39.3 Surgical Technique
39.3.1 General Approach
SWCR is performed after removing the portion of the superior and posterior external auditory canal wall required for satisfactory cholesteatoma exposure and after removal in combination with either an epitympanectomy or canal wall-down mastoidectomy, as determined by the surgeon. A piece of temporalis fascia is harvested in the typical fashion, pressed thin, and appropriately sized and shaped. The size and shape absolutely depend on the underlying defect of the eardrum and ear canal wall after cholesteatoma removal, but typically this involves a rough size of 1.5 cm2 and a rounded shape. The fascia is then placed to account for the canal wall defect on the extra-luminal aspect of the external auditory canal wall. The fascia is usually fixed with fibrin glue, but this is not necessary if it is of sufficient size to widely cover the defect. The residual preserved canal wall skin is then re-draped overlying the fascia, and the canal wall is packed with 2–3 small pieces of antibiotic-soaked gauze through the outer canal.
39.3.2 SWCR with Mastoid Obliteration
If the drilled mastoidectomy cavity is deemed excessively large, mastoid obliteration using bone paté and/or other material in combination with SWCR is recommended in order to avoid a problematic cavity should the soft wall ultimately retract (▶ Fig. 39.2a). The space between the mastoidectomy cavity and the soft posterior wall will typically shrink gradually and the soft wall retracts, forming a smoothly shaped posterior wall (▶ Fig. 39.2b).7
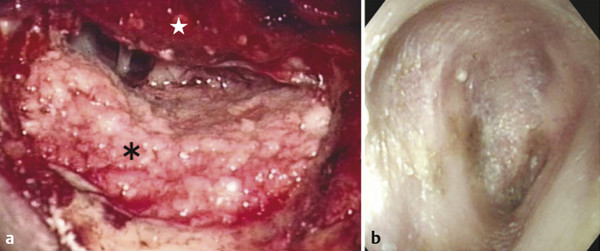
Fig. 39.2 Intraoperative views of mastoid obliteration combined with SWCR on the right ear (a) and postoperative otoscopic view (b). After SWCR (star), the mastoid was obliterated with bone paté (asterisk), and the space between them gradually shrinks to form a smoothly shaped posterior wall after surgery.
39.3.3 Second-Stage Surgery and Silicone Sheeting
In the event that a second-stage surgery is deemed necessary, a large silicone sheet can be used to cover the Eustachian tube up into the mastoid cavity in lieu of mastoid obliteration (▶ Fig. 39.3). This has been shown to facilitate recovery of mastoid aeration even after mastoidectomy.8
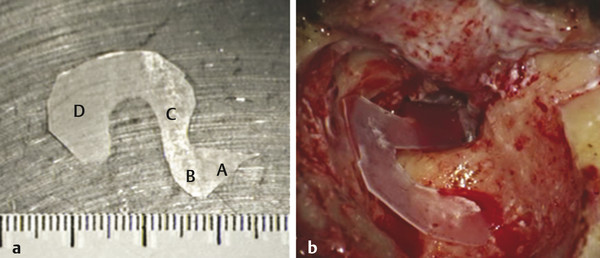
Fig. 39.3 Whole view (a) and intraoperative view (b) of a large-sized silicone sheet extending from the Eustachian tube (A), tympanum (B), epitympanum (C), and mastoid (D).
39.3.4 Application of SWCR for Non-Inflamed Ears
In cases that do not involve cholesteatoma and chronic ear disease, most of the intact mastoid and epitympanic mucosa can be preserved. Thus, the bony posterior wall can be removed with a high degree of confidence that mastoid aeration will recover in the early postoperative period and that the soft canal wall will not retract. It is actually easier to preserve the mastoid and epitympanic mucosa during surgery in these ears than in those with chronic otitis media because the middle ear is usually clean and does not have to be eradicated. For example, in such instances, a transmeatal atticotomy can be confidently extended to a transmeatal antrotomy and then further extended to a canal wall-down procedure, if needed, without hesitation. Similarly, a transmastoid facial recess approach can be expanded in the lateral direction to encompass the entire bony posterior external auditory canal wall if necessary. With any of these approaches, the soft wall will not retract after surgery if the canal skin and most of intact mastoid and epitympanic mucosa can be preserved.
39.4 Postoperative Care
Packing is kept in place usually for 3-6 days. After removal of packing, all we should do is to use eardrops containing both antibiotics and steroids for 3 days. Patients are followed up at 1, 3, 6, and 12 months after surgery and once every year for 5 years after that.
39.5 Complications
One possible disadvantage of SWCR is difficulty with post-surgical inspection and care of an open mastoid cavity that may result if the soft posterior wall retracts, especially if this cavity is large relative to the small size of the external auditory meatus. To avoid this, the surgeon may opt to make an incision in the soft posterior wall medially up to the edge of the tympanic membrane, opening the skin; however, the result will typically be an open mastoidectomy cavity instead of a SWCR, and the ear will lack the advantage of rapid healing. Alternatively, the M-meatoplasty, first reported by Mirck,9 is the author’s preferred technique to deal with this possible complication, due to the ability to selectively open the lateral aspect of the meatus while relatively sparing the deep part of the meatal wall, thereby allowing inspection of the ear while preserving the advantages of SWCR. The technique of M-meatoplasty is described in detail in Chapter 20.
Other possible complications, such as graft failure, necrosis, or incomplete canal wall closure, are similar to standard canal wall–up mastoidectomy procedures in their incidence. Antibiotic eardrops often successfully prevent infection on necrotic fascia, leading to natural healing, and placement of antibiotic-soaked absorbable packing may often cause natural closure of the defect. Finally, although the soft wall may hide residual cholesteatoma, its incidence is usually low given that this procedure includes a wide surgical view, similar to that of the canal wall–down mastoidectomy procedure.
39.6 Outcomes
As already alluded to, two distinct patterns can be observed postoperatively regarding the behavior of the soft posterior canal wall. In some ears, the reconstructed soft wall retracts to form a space similar to an open mastoidectomy cavity; however, in other ears, the canal wall remains in the original position, similar to a canal wall-up procedure. When viewing this phenomenon from the standpoint of middle ear ventilation and pressure regulation, interesting features have been noted. When the mastoid and possibly the epitympanic mucosa are preserved even partially during surgery, the soft wall typically remains in position without retraction. However, if mastoid mucosa is sacrificed via mastoidectomy, the soft wall usually retracts (▶ Fig. 39.4, ▶ Fig. 39.5). Thus, whether or not the soft posterior canal wall retracts appears to be strongly correlated with whether or not the mastoid mucosa was removed during surgery (▶ Fig. 39.6). Subsequent retraction also seems highly related to postoperative recovery of mastoid aeration, which also depends on the surgical treatment of the mastoid (▶ Fig. 39.7).
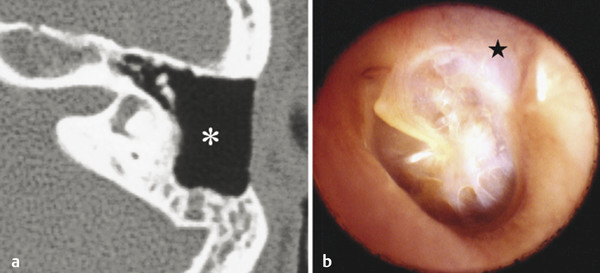
Fig. 39.4 Computed tomography (CT) scan (a) and clinical appearance (b) 6 months after surgery for attic cholesteatoma in a 21-year-old female patient. Mastoid mucosa was preserved during surgery, and mastoid aeration recovered clearly (asterisk), with the soft posterior wall (star) keeping a proper position without retraction.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


