
 he anterior portion of the eyelid contains the lashes embedded in hair follicles. In some instances, a lash can point toward the eye. This condition is called “trichiasis.” Trichiasis without entropion must be treated by destroying the roots of the individual cilia.
he anterior portion of the eyelid contains the lashes embedded in hair follicles. In some instances, a lash can point toward the eye. This condition is called “trichiasis.” Trichiasis without entropion must be treated by destroying the roots of the individual cilia.
According to Elders1 the dimensions of the follicles are (mean ±SD): upper lid follicle depth, 1.8±0.3 mm; bulb width, 188±44 µm; shaft width, 205±28 µm; lower lid follicle depth, 0.9±0.2 mm; bulb width 132±19 µm; and shaft width, 158±26 µm. Significant differences exist in the anatomy of the follicles between the two lids. For an electrolysis needle to completely contact 95% of all follicles, it must be inserted 2.4 mm into the upper lid and 1.4 mm into the lower lid.
The causes of lash misdirection are numerous, and some are listed in Table 4.1. The most common among these are trachoma, Steven–Johnson syndrome, and trauma. When trichiasis is accompanied by entropion, both the lid and the lashes must be treated. In congenital districhiasis (Fig. 4.1), an extra row of small eyelashes abnormally grow on the inner surface or very edge of the eyelids. Both upper and lower lids may be involved. This leads to epiphora and hazy vision. Each individual cilium must be dealt with.
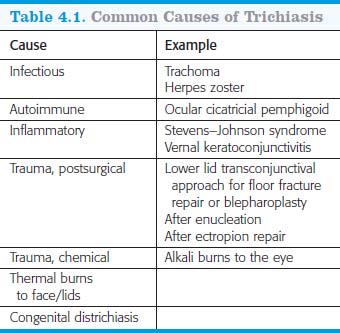

Figure 4.1. Congenital districhiasis.
Regardless of the cause, when errant eyelashes touch the cornea, treatment is indicated.
TECHNIQUE
Many procedures have been described for the treatment of trichiasis: simple epilation, electrolysis, cryosurgery, argon-laser ablation, and radiofrequency ablation. But epilation is a temporary measure, electrolysis is tedious, and cryosurgery has potential problems as damaging additional hair follicles. Radiofrequency ablation is effective; the core tissue is removed by the cut–coagulate method. A lot of energy is transferred to the tissue in the process, however, which produces tissue reaction and some scarring. The Fugo blade is swift and highly effective for cilia removal. It does so swiftly and effectively. The technique could be termed the “fugolysis” of cilia.
The figures 4.2, 4.3, 4.4, and 4.5 record the treatment of a patient with Steven–Johnson syndrome in who a new row of cilia had developed as a result of metaplasia of the meibomian glands.
Anesthesia
Prepare the patient by injecting adequate lidocaine along the lid margin.
Surgical Technique
Several Fugo blade tips are available. I use either a 3.5-mm naked (without insulating tubing) 100-µm Fugo blade tip or a long, tapered 300-µm tip.
- Use medium power and energy settings for destroying the cilia roots.
- Align the tip with the cilium. Slip the ablating tip alongside the shaft of the cilium (Fig. 4.2). (If the misdirected cilia are short, stiff, and tight in the tissue and do not allow a 100-µm tip to enter alongside the shaft, use a sharp, pointed 300-µm tip; it performs just as well as the 100-µm tip.)
- When the tip reaches the desired depth, activate it momentarily (Fig. 4.3). For the tip to be effective, it should reach the root of the cilia for ablation.
- As you withdraw the inactivated tip, the cilium comes along with it.
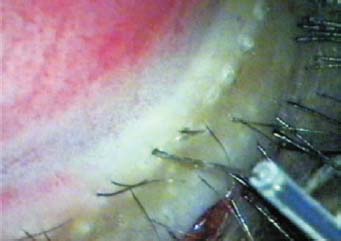
Figure 4.2. The naked 100-µm fiber of the Fugo blade tip is slipped alongside the cilium.

Figure 4.3. The tip is activated when it reaches the depth of the follicle.
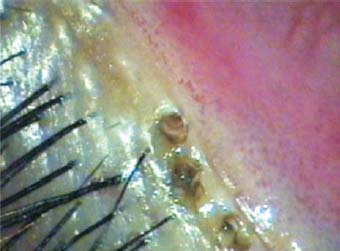
Figure 4.4. No burning effect is seen at the site where ablation has been carried out.

Figure 4.5. The whole row of cilia have been removed.
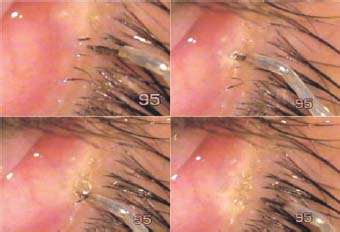
Figure 4.6. A 300-µm tapered tip has been used to ablate the cilia roots in this case.
The procedure is extremely quick. You can confidently remove a whole row of cilia in congenital districhiasis in a couple of minutes. You can remove the core tissue by ablation using minimal energy transfer through resonance. No burning or coagulation of the tissues is involved (Figs. 4.4–4.6).
Postoperative Management
This procedure does not cause postoperative pain or scarring. If a follicle fails to be destroyed, the proce-dure can be repeated.
Reference
1. Elders MJ. Anatomy and physiology of eyelash follicles: relevance to lash ablation. Ophthalmol Plast Reconstr Surg. 1997;13:21–25.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


