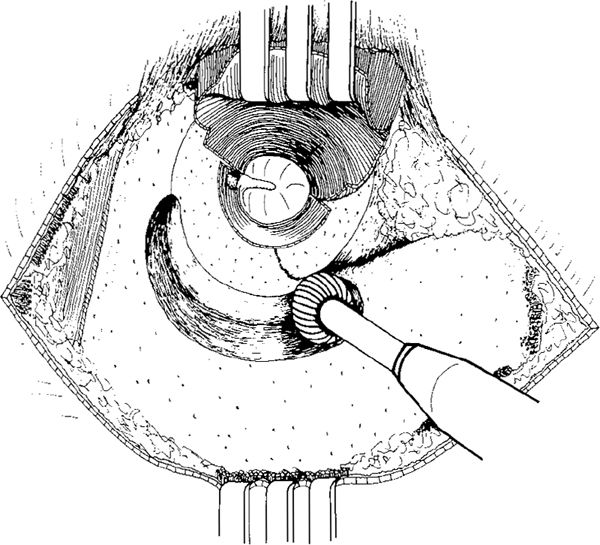
Fig. 615 Transmeatal outside-in canal wall–down mastoidectomy in a retroauricular approach. After a retroauricular flap incision (Vol. 1, Fig. 135–147) an anterior-based subcutis–muscle–periosteum flap is elevated, exposing the mastoid plane and temporal line, in the ear canal. A medial circumferential incision between the 12-o’clock and 6-o’clock positions and radial incisions at the 12-o’clock and 6-o’clock positions, with elevation of the posterior ear canal skin flap, are carried out. The posterior half of the ear canal and the mastoid plane are exposed, and drilling at the entrance to the ear canal using a large cutting burr is initiated
Transmeatal canal wall–down mastoidectomies can therefore be divided into: a) retroauricular operations and b) endaural ones.
The retroauricular operations are:
1. Outside-in mastoidectomy, starting at the suprameatal spine in a retroauricular approach.
2. Inside-out mastoidectomy, starting at the bony annulus in a retroauricular approach.
The endaural operations are:
1. Outside-in mastoidectomy, starting laterally by widening the ear canal in an endaural approach.
2. Inside-out mastoidectomy, starting at the annulus in an endaural approach.
Inside-out mastoidectomies are also termed “retrograde mastoidectomies.”
Outside-In Transmeatal Canal Wall–Down Mastoidectomy
With a retroauricular approach, an anteriorly pedicled subcutis–muscle–periosteum flap is elevated and held in place using a self-retaining retractor. The canal skin is incised with a medial circumferential incision from the 12-o’clock, to the 6-o’clock positions and superior and inferior radial incisions at the 12-o’clock and 6-o’clock positions, respectively, allowing elevation of a large laterally based posterior ear canal skin flap (Körner flap), which is held in place with a selfretaining retractor. The mastoid plane and most of the ear canal are exposed (Fig. 615), the temporal line is demarcated, and drilling is started using the largest cutting burr, first removing the suprameatal spine, and then the lateral part of the posterior bony ear canal wall (Fig. 616). The drilling proceeds by continued removal of the posterior bony ear canal wall between the 12-o’clock and 5-o’clock positions, and moves further posteriorly, along the middle fossa dural plate (Fig. 617). Körner’s septum has not yet been reached, and the antrum has not been opened (Fig. 618). After further deeper drilling in a posterior direction along the middle fossa dural plate, Körner’s septum is penetrated, and the antrum becomes visible through a small opening (Fig. 619). The lateral mastoid air cells are exenterated toward the mastoid tip. The depth of the drilling is easy to determine because of the constantly visible surface of the ear canal, allowing assessment of the distance to the bony annulus (Fig. 620). The opening to the antrum is gradually enlarged, and Körner’s septum is removed until the antrum has been completely opened (Fig. 621). The bony overhangs over the antrum are removed, the middle fossa and posterior fossa dural plates polished, and the ear canal wall is further lowered (Fig. 622).
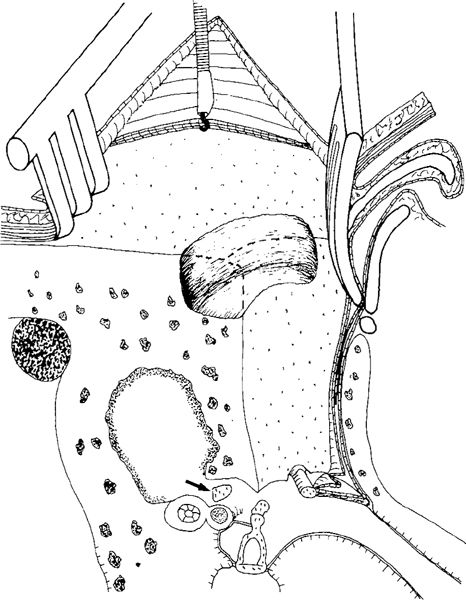
Fig. 616 Side view with some perspective, illustrating a retroauricular approach and House selfretaining retractor with a protecting blade placed in the anterior part of the ear canal, protecting the posterior meatal skin flap. In the tympanic cavity, the malleus handle with the anterior part of the drum, the stapes with the lenticular process, and the short process of the incus (arrow) are indicated, as well as the facial nerve and the lateral semicircular canal.
The initial drilling is started at the entrance to the bony ear canal wall. The dashed line indicates the original position of the entrance of the ear canal (also in the following side-view figures)
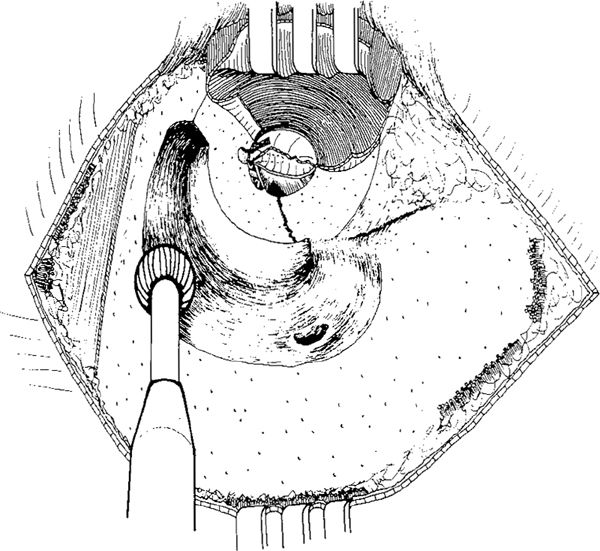
Fig. 617 Drilling continues along the mastoid tegmen, and more of the posterior bony ear canal is removed. Interiorly, the very lateral part of the facial ridge is indicated. The antrum has not yet been reached, and the medial two-thirds of the ear canal are still intact
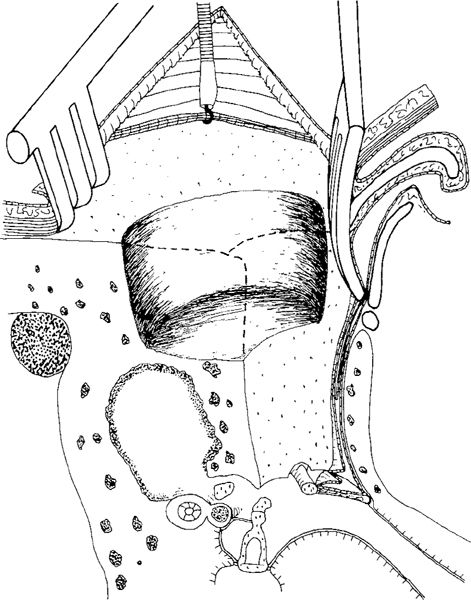
Fig. 618 Side view some perspective of the drilling, which has just reached the Körner’s septum level. The antrum has not been opened yet. A posterior tympanotomy is performed, exposing the incudostapedial joint
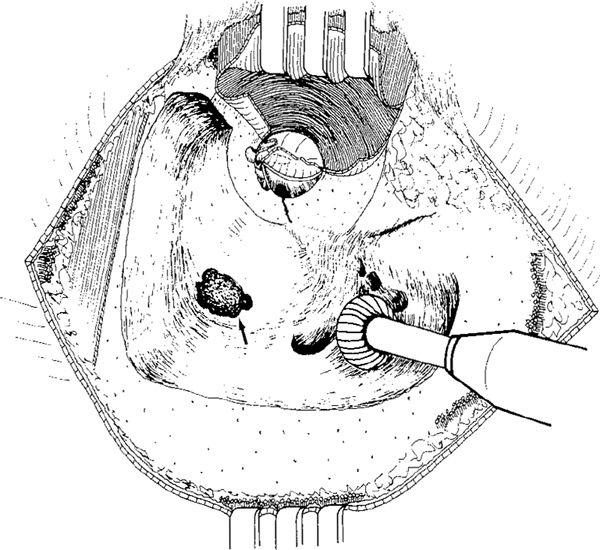
Fig. 619 Körner’s septum is penetrated, and posteriorly the antrum is opened (arrow). The lateral mastoid cells are exenterated toward the mastoid tip. Superiorly, drilling along the mastoid tegmen is extended up to the middle fossa dural plate and the temporal line. The medial half of the posterior ear canal wall is still intact
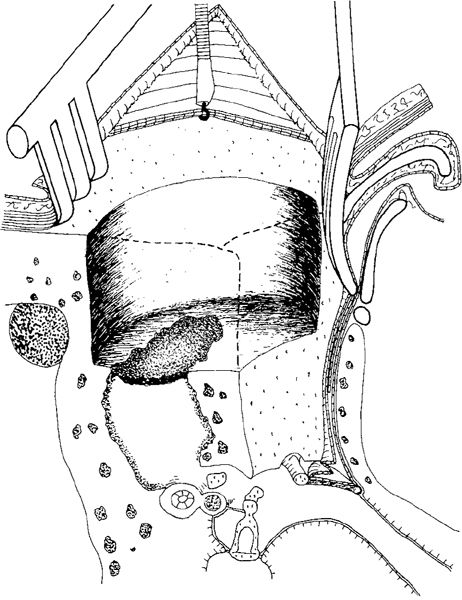
Fig. 620 The level of the drilling, illustrated in a side view of the mastoid process with some perspective. The antrum has been opened. The dashed line indicates the original entrance of the ear canal. The medial half of the bony ear canal wall is still intact
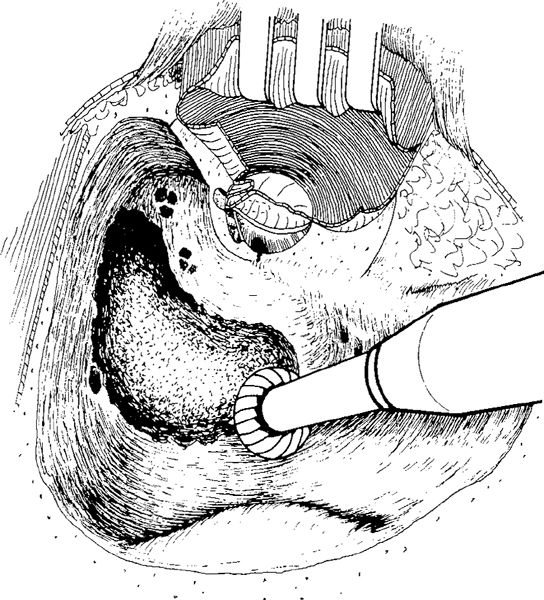
Fig. 621 The antrum has been widely opened, and the cavity walls have been smoothed. Posteriorly, the prominence of the lateral sinus and a smoothed posterior fossa dural bony plate are seen, and medially, the anterior attic. The ossicular chain and the lateral semicircular canal are conceded by bone and not visible
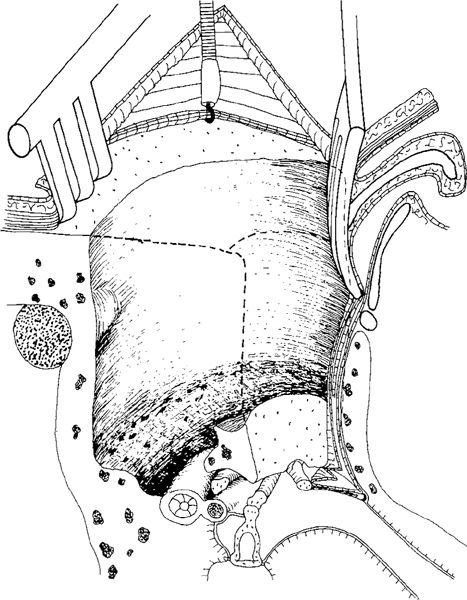
Fig. 622 Side view with some perspective illustrating the level of the drilling in transmeatal outside-in canal wall–down mastoidectomy. The mastoid tegmen is smoothed, and the antrum has been completely opened. The posterior fossa dural plate is smoothed, but more or less the medial quarter of the ear canal wall is still intact, covering the incus and the lateral semicircular canal
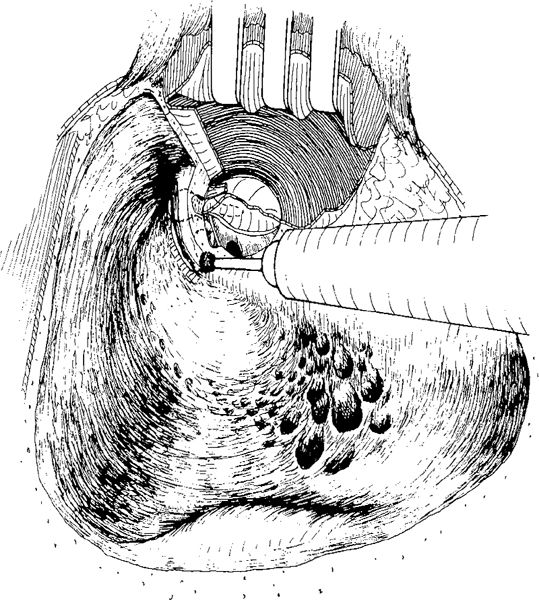
Fig. 623 The lateral semicircular canal, incus body, and malleus head are only partly exposed, but still some 2 mm of the ear canal remains to be removed. The tegmen antri is smoothed, and the facial ridge is gradually lowered to achieve removal of the ear canal wall
Drilling continues posteriorly along the middle fossa dural plate, smoothing it and exenterating the cells from the sinodural anlge (Fig. 623). The ear canal is further lowered, and a careful inspection of the lateral semicircular canal and ossicular chain, which now becomes visible, is made (Fig. 624). Further lowering of the bony ear canal, using a diamond burr, exposes more and more of the ossicular chain (Fig. 625). The anterior attic is reached by further lowering of the bridge, and the tensor tympani fold (Figs. 92–94) is penetrated using a curved rugine (Fig. 626). Further drilling leads to maximal thinning of the bony bridge. The facial ridge is lowered, and all the walls of the cavity are polished (Figs. 627, 628).
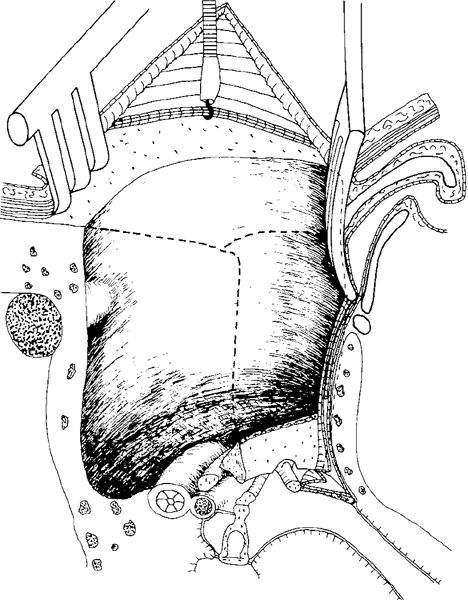
Fig. 624 Side view of the level of the drilling, illustrating gradual removal of the ear canal wall, which has been lowered to 1.5 mm
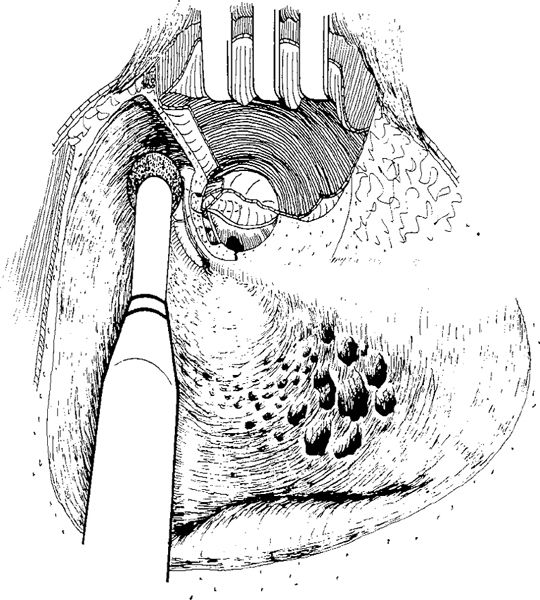
Fig. 625 Further removal of the ear canal wall and exposure of the malleus head and incus body, continuing with drilling toward the anterior attic
In cases with extensive pneumatization, any large mastoid tip cells have to be removed (Fig. 629), resulting in a large cavity (Fig. 630). In cases with extensive pneumatization, the advantage of the retroauricular approach compared to the endaural approach is therefore evident. Drilling toward the mastoid tip is difficult in an endaural approach, but easy in a retroauricular approach (Fig. 629).
Of course, canal wall–down mastoidectomy usually results in removal of the bridge, and the results are exactly the same as those illustrated for transcortical canal wall–down mastoidectomy, leading to the following situations:
1. Preservation of the intact ossicular chain, without the bridge but with a relatively high facial ridge (Figs. 584, 585).
2. Preservation of the intact ossicular chain and a low facial ridge (Figs. 586, 587).
3. Removal of the incus, but preservation of the malleus and a low facial ridge (Figs. 588, 589).
4. Resection of the malleus head and removal of the incus, with lowering of the facial ridge (Figs. 590, 591).
5. Removal of the entire malleus and incus, usually accompanied by an absent stapedial arch (Fig. 631) and its reconstruction with an reshaped columella and fascial graft (Fig. 632).
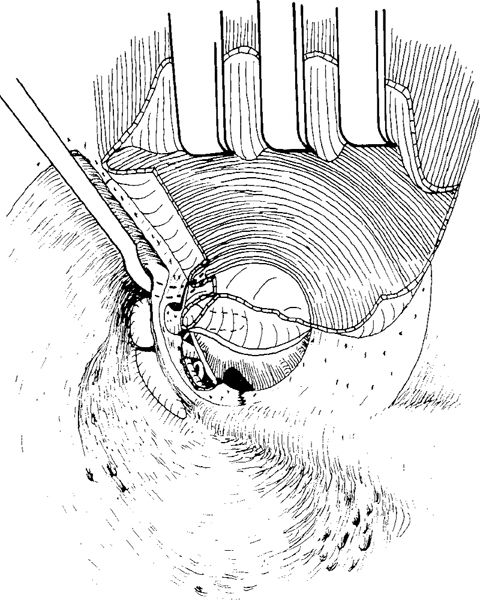
Fig. 626 Transmeatal anterior atticotympanotomy. With a curved rugine, the tensor tympani fold is penetrated, the bony bridge is further thinned and the facial ridge is lowered
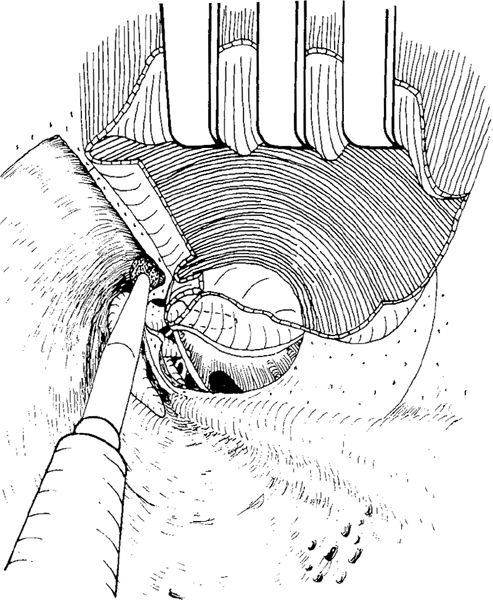
Fig. 627 Using a diamond burr, the anterior bony plate is removed and the anterior attic further exposed
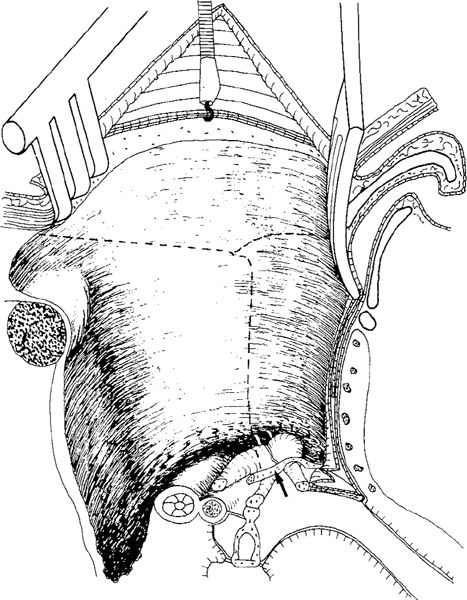
Fig. 628 Side view of the cavity in transmeatal canai wall–down mastoidectomy with preservation of the bridge. The bony bridge is thin (arrow), and the cavity walls have been smoothed
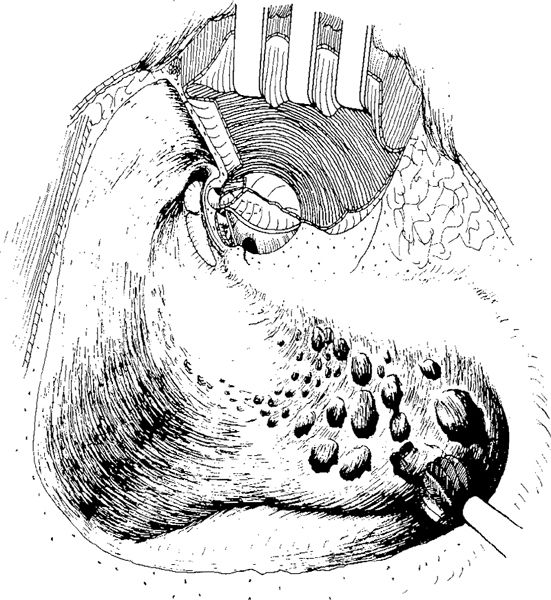
Fig. 629 Extensive pneumatization with large mastoid tip cells being exenterated using a large cutting burr
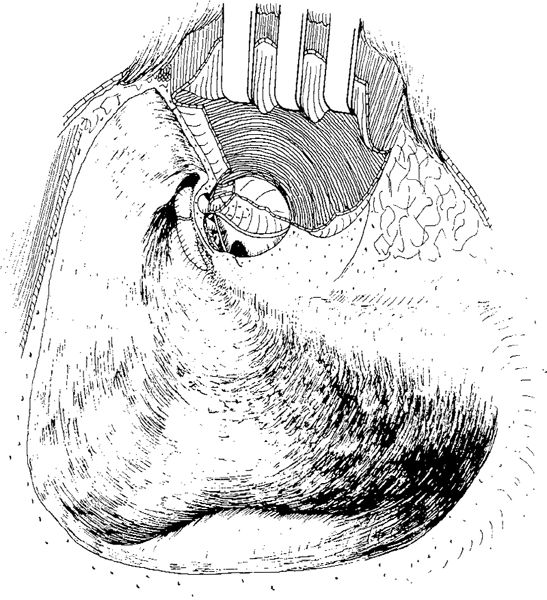
Fig. 630 The mastoid tip air cells are exenterated, resulting in a relatively large cavity
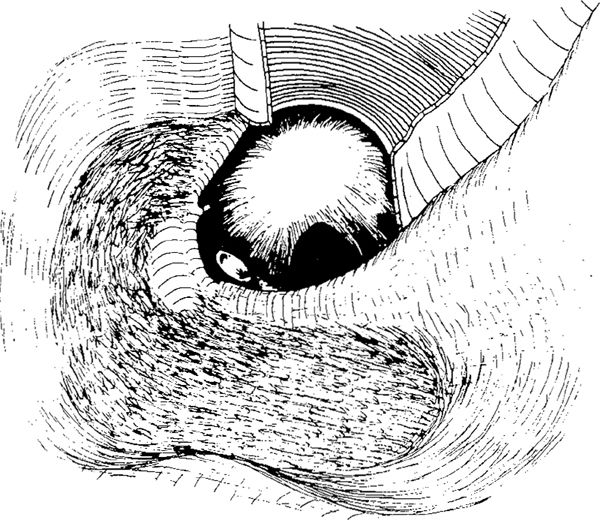
Fig. 631 Canal wall–down mastoidectomy leaving only the fibrous annulus of the drum and a mobile foot-plate
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


