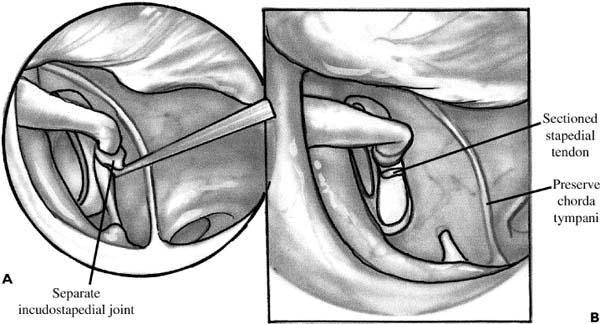
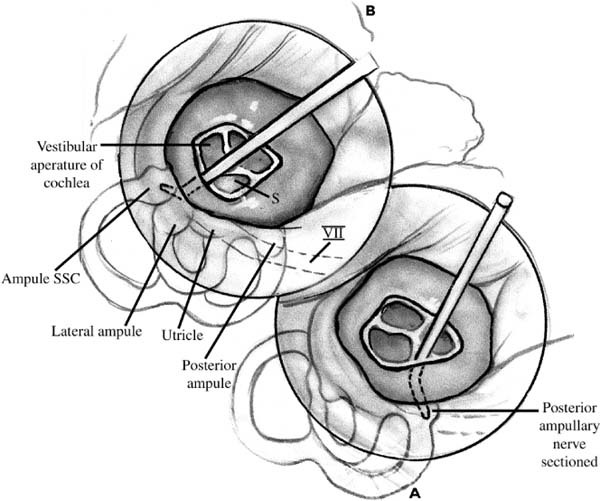
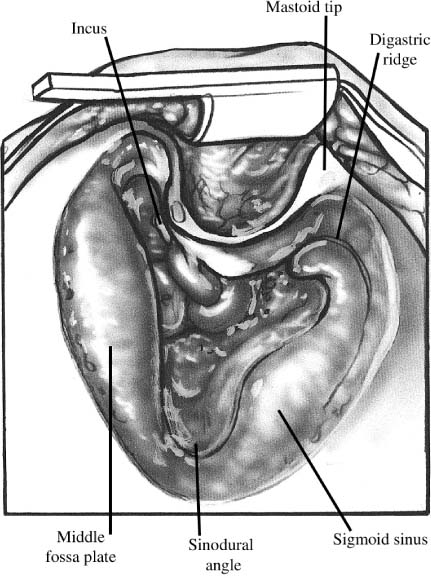
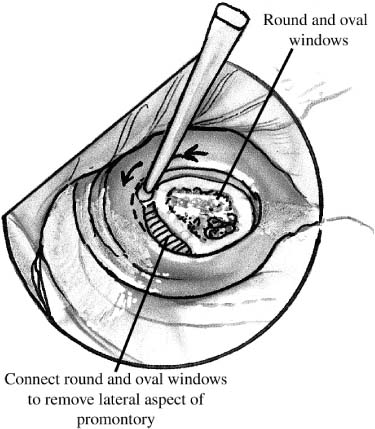
Chapter 25 Initial attempts to control vertigo are primarily medical; when those attempts fail, however, surgical approaches for control may be necessary. Multiple options exist including cochleosacculotomy, endolymphatic sac surgery, labyrinthectomy (transcanal and transmastoid) with or without vestibular nerve section, and vestibular nerve section (middle cranial fossa or retrosigmoid approach). Chemical labyrinthectomy has also become a commonly used option. Surgical labyrinthectomy is a highly successful procedure for a patient with nonserviceable hearing in the affected ear. Jansen in 1895 was the first to describe ablation of the labyrinth during radical mastoidectomy for suppurative labyrinthitis. In 1904 Lake described the use of the transmastoid labyrinthectomy for control of vertigo in nonsuppurative vertigo. Cawthorn reported a wall-up mastoid approach for labyrinthine ablation in 1943. Crockett in 1903 was the first to describe a transcanal procedure for control of vertigo by removing the stapes. Lempert in 1948 reported on the endaural approach with removal of the stapes and decompression of the labyrinth. The transcanal labyrinthectomy with removal of the vestibular end organs, however, was first described by Schuknecht in 1956. In addition to removal of the membranous labyrinth manually or with suctioning, various agents have also been injected into the labyrinth for further ablation, and the use of laser and ultrasound has also been described.1–3 Labyrinthectomy is usually the option of last resort for patients with intractable vertigo. It has classically been described for Meniere’s disease patients without useful hearing for whom medical management has failed. Vestibular suppressants, diuretics, and vestibular rehabilitation should be given an adequate trial before surgical procedures. Labyrinthectomy is used in refractory cases and it is therefore important to confirm a unilateral peripheral vestibular deficit and rule out other central causes of vertigo. A careful history should be reviewed for any trauma, systemic diseases, and neurologic disorders. Patients with vertigo due to sequelae from head trauma, vestibular neuronitis, viral labyrinthitis, ischemic disease, neurologic disorders, and positional vertigo are less likely to benefit from labyrinthectomy. Careful counseling is needed for these situations. Therefore, it is recommended that all patients should have a full audiometric evaluation, electronystagmography including cold calorics, and imaging of the internal auditory canals, preferably using magnetic resonance imaging. Laboratory tests for syphilis, Lyme disease, autoimmune disorders, and thyroid function should also be obtained. High-resolution computed tomography of the temporal bones may also be obtained for surgical planning and to check for any anomalies of the facial nerve or labyrinthine structures. Because surgical labyrinthectomy is expected to result in total sensorineural hearing loss in the operated ear, confirmation of severe hearing loss is needed. Candidates generally have greater than 50-dB speech reception thresholds (SRTs) and less than 50% speech discrimination scores (SDSs) in the affected ear. Those patients with less than 30 dB SRT and greater than 70% SDS are generally considered candidates for hearing preservation procedures.4,5 These guidelines assume normal hearing in the contralateral ear. In cases where the contralateral hearing is poor, the decision for surgery must be done on a case-by-case basis. Assessment of the binaural hearing should be done in cases where the opposite ear is also affected. Some surgeons advocate even greater SRT and SDS thresholds in Meniere’s patients because of the possibility of developing bilateral Meniere’s.5 In addition, a unilateral peripheral vestibular deficit must be demonstrated. Although the absence of a caloric response on the affected side should be approached cautiously, patients have had relief of vertigo even with an absent cold caloric. Caloric testing tests only the horizontal canal. There should be some function on the contralateral side, however. Patients with bilateral vestibular deficits often do poorly after unilateral vestibular ablation secondary to inadequate compensation. They are unable to maneuver in the dark and have constant dysequilibrium and oscillopsia. Even patients with normal contralateral vestibular function may suffer persistent ataxia after ablation, although it is usually not disabling. The preoperative status of the patient must also be taken into account. Obesity, impaired vision, arthritis, peripheral neurologic deficits, and other conditions that may impair patients’ maneu-verability may negatively impact their postoperative recovery. Finally, the decision of transcanal versus transmastoid labyrinthectomy must be made. Chemical labyrinthectomy is also an option and is discussed later in the chapter. Although a transcanal procedure is shorter, has lower morbility, and is a more direct route to the labyrinth, multiple studies have shown that the success rate of a transcanal labyrinthectomy is lower and the recurrence rate of vertigo higher. This is likely due to the incomplete removal of all of the vestibular end organs. In patients who are a substantial operative risk, however, it is a valid approach. Patients must undergo general anesthesia for surgical labyrinthectomies because of the nausea and vomiting that accompany removal of the labyrinth. A facial nerve monitor may be used during the procedure due to the proximity of the horizontal segment of the facial nerve to the operative site. Preoperative antibiotics and steroids are not required. Anesthesiologists should be asked not to use paralytic agents if facial nerve monitoring is performed. The patient is placed supine on the operating table with the affected ear up. The ear is prepped with antiseptic solution and draped accordingly. The operating microscope is also draped after checking for proper balance. A transcanal approach is sufficient for most patients; however, if the canal is narrow, an endaural or postauricular incision may be necessary for full exposure. Local anesthetic with 1:100,000 epinephrine is injected into the canal. Using the largest speculum possible in a speculum holder, a long tympanomeatal flap is raised. Part of the scutum is then removed either using a curette or a small bur to expose the horizontal segment of the facial nerve. Full exposure of the facial nerve and oval and round windows is required (Fig. 25–1A). A portion of the posterior bony canal may also need to be removed. The incus can be removed and the stapedial tendon sectioned (Fig. 25–1B). The stapes is carefully removed by rocking in an anteroposteriormotion to prevent fracture of the footplate. Avoid suctioning to prevent retraction of the utricle super-iorly. The oval window is now enlarged using a microdrill, or the oval and round windows may be connected to remove the bony promontory (Fig. 25–2). The inferior portion of the round window niche is then removed to expose the posterior ampullary nerve (singular nerve). Sectioning of the singular nerve facilitates a full labyrinthectomy, as the crista of the posterior semicircular canal is difficult to remove using the transcanal approach. The nerve is approximately 1 mm medial to the posterior edge of the round window niche at a 45-degree angle. Sectioning is done using a small pick (Fig. 25–3A). Any cerebrospinal fluid (CSF) leak that occurs can be controlled using bone wax. FIGURE 25–1 (A) Transcanal labyrinthectomy. A tympanomeatal flap has been raised and the incudostapedial joint separated. (B) Stapedial tendon is sectioned in preparation for removal of the stapes. FIGURE 25–2 The oval and round windows are connected to remove the bony promontory. Carefully examine the facial nerve for areas of dehiscence. The utricle is now removed using a 3- or 4-mm right-angle hook, whirlybird, or utricular hook. It lies in a recess that is deep and superior to the horizontal facial nerve (Fig. 25–3B). Irrigating with saline may be helpful at this point to free the utricle from the walls of the recess. Removal of the utricle usually also results in removal of the membranous horizontal and superior semicircular canals. The saccule is then removed by aspirating the medial portion of the vestibule. Fracture of the cribrose area, in the medial portion of the vestibule, results in a CSF leak from the internal auditory canal. The bony semicircular canals are then probed to destroy any residual neuroepithelium. The vestibule can be packed either with Gelfoam or fat. This is not absolutely necessary, but leaving the windows open results in a pneumolabyrinth. Packing also helps contain any CSF leaks that may have occurred. The flap is then replaced and the canal packed. If a postauricular incision was made, the incision is closed and a dressing placed.6,7 FIGURE 25–3 (A) The posterior ampullary nerve is sectioned with a pick. It is located 1 mm medial to the posterior edge of the round window at a 45-degree angle. (B) A hook is used to remove the utricle and semicircular canals, which are located deep and superior to the horizontal facial nerve. SCC superior semicircular canal; VII, facial nerve; S, saccule. The patient is placed under general anesthesia and placed supine on the operating table. The table should be turned 90 or 180 degrees. The affected ear is up and the postauricular shave prep is extended several finger-breadths behind the ear. The exposure is usually a little more than that used in a standard mastoidectomy because of the need for greater exposure for the medial dissection. Place the facial nerve monitor leads and ensure that the monitor is working properly. A high-speed drill with multiple cutting and diamond burs should be available. Both monopolar and bipolar cautery should also be available. The postauricular area is then injected with epinephrine (1:100,000). If this is combined with local anesthesia, care must be taken not to inject at the mastoid tip and anesthetize the facial nerve. The anesthesiologist should be informed that nerve monitoring is taking place, and so paralytics should be avoided. If more than one anesthesiologist is giving agents during the procedure, it is important to communicate this instruction. In some operating room settings, this is instruction is posted in a prominent location. Preoperative antibiotics and steroids have not been shown to affect outcomes or postoperative infection rates. The area is then prepped and draped in a sterile fashion. The surgeon should also check the operating microscope and ensure proper balance prior to draping. A postauricular incision is made and carried down to the temporalis muscle. Monopolar cautery is then used to make a T incision along the linea temporalis and down to the mastoid tip. A Lempert elevator is used to widely elevate the periosteum off the mastoid cortex, taking care to identify the spine of Henle anteriorly. The soft tissues are then held in place using self-retaining retractors. Any bleeding encountered during the dissection is controlled using electrocautery. A dry field is important for good visualization of the operative area. A cortical mastoidectomy is then performed using a large cutting bur and continuous suction irrigation. The tegmen and sigmoid sinus are identified and the posterior bony canal thinned. The sinodural angle is opened widely for exposure of the vestibule. The antral air cell is entered and the horizontal canal, fossa incudis, and body of the incus should all be seen clearly (Fig. 25–4). The sigmoid sinus may also need to be decompressed for adequate exposure of the posterior semicircular canal. The bone over the sinus is carefully thinned and removed. Bipolar cautery is then used to collapse the sinus. Leaving an island of bone covering the sinus requires the use of a retractor. No ill effects usually result from superficial coagulation and contraction of the sigmoid sinus. The vertical segment of the facial nerve is now carefully identified using a large diamond bur. FIGURE 25–4 Transmastoid labyrinthectomy. A view of the horizontal canal, fossa incudis, body of the incus, tegmen, and sigmoid sinus after the cortical mastoidectomy.
TRANSMASTOID AND TRANSCANAL LABYRINTHECTOMY
PATIENT SELECTION
SURGICAL TECHNIQUE
TRANSCANAL LABYRINTHECTOMY
TRANSMASTOID LABYRINTHECTOMY
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


