FIGURE 4.1 A. T1-weighted coronal MRI showing a giant grade 1 pituitary tumor. The tumor does not enter into the confines of the cavernous sinus. The diaphragma sellae is elevated. B. T1-weighted sagittal view showing the large tumor and the elevated diaphragma sellae.
Grade II (Fig. 4.2) pituitary tumors are those that invade the cavernous sinus. Although there are other parameters that suggest invasion of tumor into the cavernous sinus, encasement of the intracavernous carotid artery is a clear sign of cavernous sinus invasion. The cavernous sinus is frequently bloated full by the tumor, but its dural walls are not transgressed.
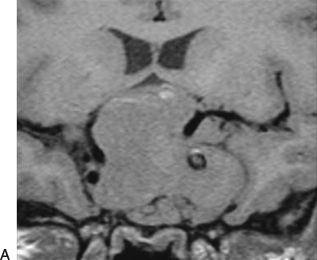
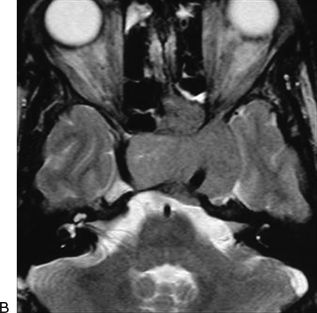
FIGURE 4.2 A. T1-weighted MRI showing a grade 2 giant pituitary tumor. The tumor invades the cavernous sinus. The diaphragma sellae is elevated. B. T2-weighted axial view of the scan showing cavernous sinus involvement by a grade 2 pituitary tumor.
Grade III (Fig. 4.3) giant pituitary tumors are those where the roof of the cavernous sinus is elevated superiorly, sometimes to a considerable degree. Such an elevation of the roof of the cavernous sinus is frequent and can be mistaken as frontal or temporal lobe extension. The dura of the roof of the cavernous sinus is thin, and such elevation usually displaces the third cranial nerve. Although it is not possible to convincingly confirm, it does appear that the tumors that elevate the roof of the cavernous sinus are inherently more aggressive and the recurrence rates in such cases are relatively higher. Primary radiotherapy may be considered in such cases.
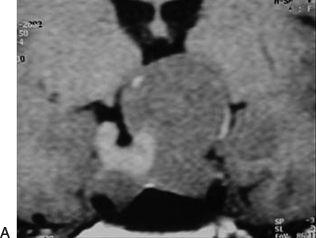
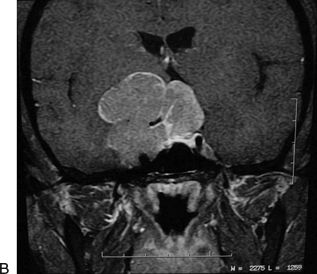
FIGURE 4.3 A. Pre-contrast coronal MRI showing a grade 3 pituitary tumor. The diaphragma sellae is elevated. The roof of the cavernous sinus is seen to be elevated by the tumor. B. Contrast-enhanced coronal MRI showing a grade 3 pituitary tumor. The diaphragma sellae and the roof of the cavernous sinus are elevated.
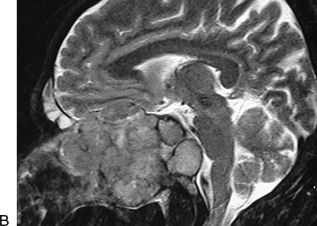
Grade IV (Fig. 4.4) pituitary tumors are those that transgress the diaphragma sellae boundary and enter into the subarachnoid spaces of the brain. These tumors encase the arteries of the circle of Willis.
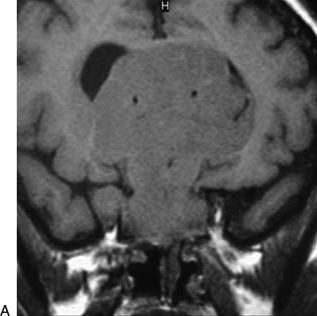
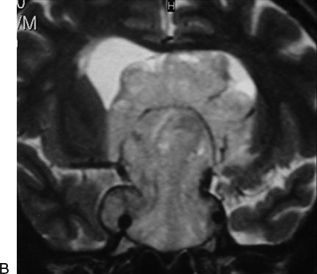
FIGURE 4.4 A. T1-weighted coronal MRI showing grade 4 pituitary tumor. The anterior cerebral arteries are encased by the tumor. B. T2-weighted coronal MRI showing the encasement of both A1 segments and Acom complex of the anterior cerebral artery.
The tumors in grades 1 to 3 are below the diaphragma sellae and the superior wall of the cavernous sinus. As the cavernous sinus is considered to be an extradural entity, these tumors are essentially “extradural” in nature. The tumors in these three grades can and should be resected by an extracranial transnasal route. The exact mode and modality of surgery in grade 4 pituitary tumors is still debated. However, this group of tumors may be operated by a transcranial route. A transcranial route for pituitary tumors is also indicated in cases of functioning pituitary tumors that involve the cavernous sinus and extend lateral to the internal carotid artery. Transcranial surgery is sometimes indicated in cases with tumor recurrence where the cranial component is large and adoption of the nasal route is difficult due to previous operation.
Trigeminal Schwannomas
Three distinct types are middle fossa type (type A), posterior fossa root type (type B) where the tumor is in front of the brainstem, and the dumbbell type with both middle and posterior fossa components (type C) (Figs. 4.5 to 4.9). Depending on the nerve of origin, the extracranial part (type D) of the tumor is classified into orbital, infratemporal, and pterygopalatine fossa components. Middle fossa lesions are located within the confines of the dura in the lateral wall of the cavernous sinus and Meckel’s cave and as such termed as “interdural.” Despite the sometimes massive growth of these benign lesions, the confines of the dura are not eroded. The posterior fossa component of the tumor can be “intradural” in nature. However, frequently, even this part of the tumor may be “interdural” in nature. The tumor remains within the confines of dura. The cavernous sinus and internal carotid artery are displaced and a relatively thick wall of dura separates them from the tumor. The extracranial component of the tumor is also surrounded by a layer of “dural” sheath. Despite the frequently large tumor size, the majority of trigeminal nerve fibres are only displaced by the tumor.
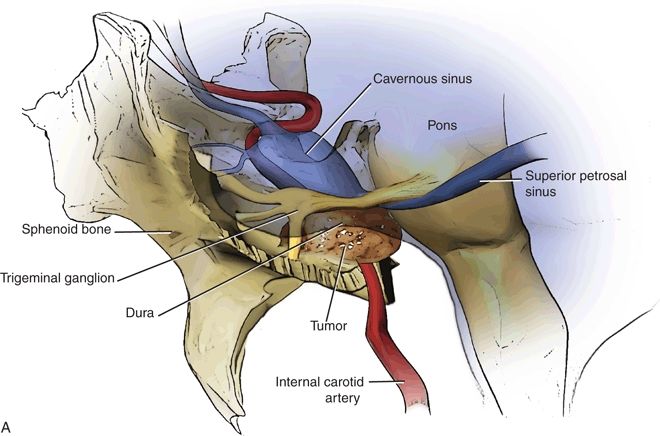
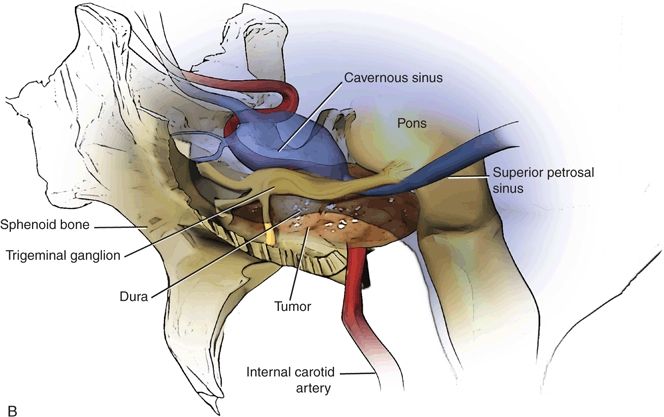
FIGURE 4.5 A. Line drawing showing the interdural trigeminal schwannoma in the middle cranial fossa. The trigeminal nerve is displaced on the superior aspect of the tumor. The carotid artery and cavernous sinus are also displaced by the tumor. B. Line drawing showing the dumbbell-shaped trigeminal schwannoma extending both in the middle and posterior cranial fossae. The trigeminal nerve is displaced by the tumor.
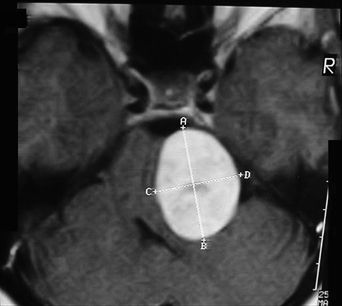
FIGURE 4.6 Trigeminal schwannoma located in the posterior cranial fossa.
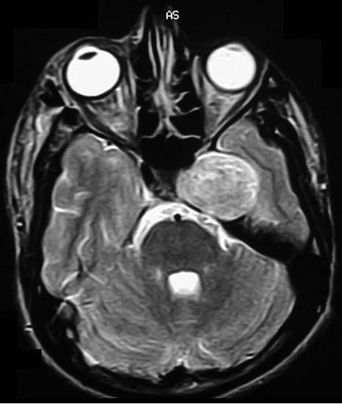
FIGURE 4.7 Trigeminal schwannoma located in the middle fossa.
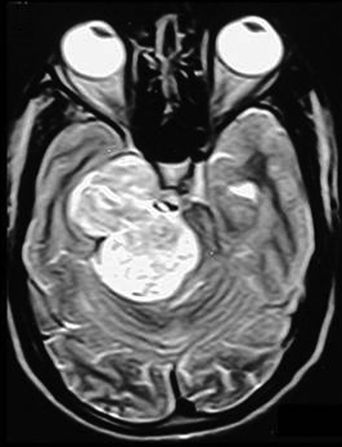
FIGURE 4.8 Large dumbbell-shaped trigeminal schwannoma extending both in the middle and posterior cranial fossae.
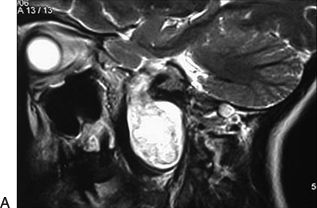
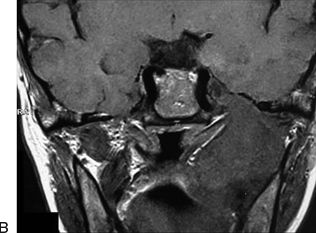
FIGURE 4.9 A. T2-weighted sagittal image showing trigeminal schwannoma extending into the extracranial compartment along the mandibular nerve. B. T1-weighted coronal image showing the trigeminal schwannoma extending into the extracranial compartment. The soft tissues are displaced by the tumor.
Chordomas
These tumors destroy bone and displace soft tissue. This character of the tumor distinguishes it from other tumors in the region (Figs. 4.10 and 4.11). Although various authors have noted cavernous sinus invasion by chordomas and chondrosarcomas, it is observed that even in massive tumors the cavernous sinus involvement by these tumors is in the form of displacement rather than invasion. This tumor arises from the clivus or the sphenooccipital synchondrosis and grows eccentrically into the subcavernous sinus region and elevates it on its dome. The functional involvement of the cranial nerves of the region is usually due to stretch. The precavernous and cavernous segments of the carotid artery are displaced anteriorly by the tumor. The tumor is primarily extradural, and actual transgression of the dura is a rare feature. Even in large lesions, a layer of dura separates the tumor from neural and vascular structures, providing a plane of cleavage for surgical resection. The location of the tumor in the extradural space makes an extracranial surgical route a viable surgical option. However, cranial approaches are suitable and safer and are compatible with radical tumor resection in a significant number of these patients. The functional recovery of cranial nerves displaced by these tumors is more remarkable than that following surgery on most other tumors in the region.
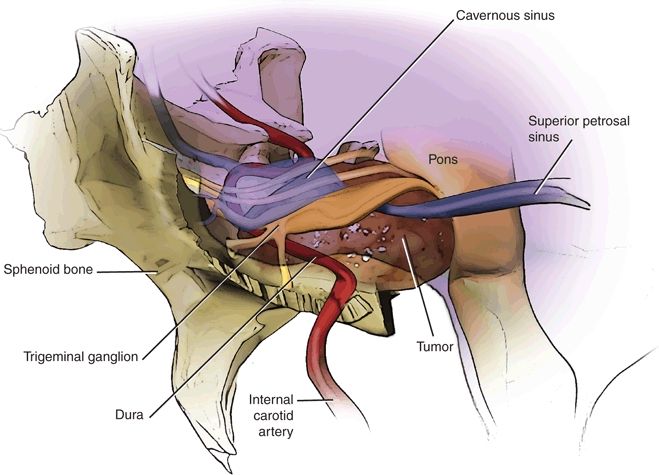
FIGURE 4.10 Line drawing showing the extradural chordoma (brown) that displaces the internal carotid artery (red) anteriorly/anterolaterally and the nerves of the cavernous sinus (yellow) superiorly.

FIGURE 4.11 T1-weighted MRI showing the chordoma. The tumor is essentially extradural and displaces the internal carotid artery anteriorly (arrow).
Craniopharyngiomas
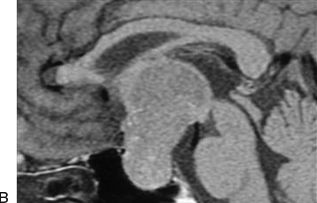
Craniopharyngiomas have been treated by craniotomy for decades (Figs. 4.12 and 4.13). However, recently, several groups recommend an endoscopic approach for such tumors. Presence of infradiaphragmatic craniopharyngioma appears to be a clear indication for a nasal approach. Such tumors have a large extension into the sella that is bloated. However, in the presence of supradiaphragmatic craniopharyngiomas and of a small sella, a transcranial approach may be more suitable. Surgery on craniopharyngiomas continues to be debated. The extent of capsular resection, the need to preserve the pituitary stalk, and the indications of radiation treatment are still debated. The dissection of intracranial intradural tumor and of the arteries of the Circle of Willis from the dome of the tumor is simpler and safer by a transcranial approach than by a nasal endoscopic approach.
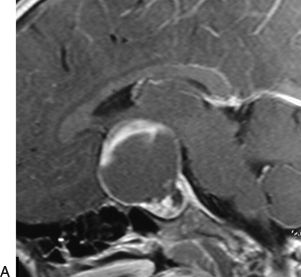
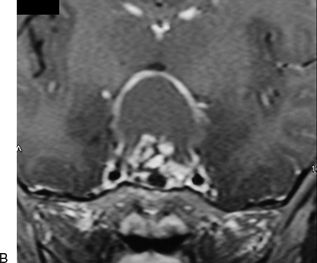
FIGURE 2.12 A. Sagittal contrast-enhanced T1-weighted MRI showing a craniopharyngioma with enlarged sella. The craniopharyngioma in this case is subdiaphragmatic in nature. B. Coronal post-contrast T1-weighted view showing the craniopharyngioma.
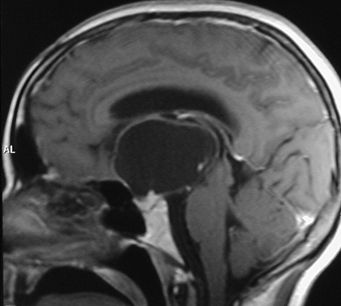
FIGURE 4.13 Sagittal contrast-enhanced T1-weighted view of MRI showing a craniopharyngioma with a small sella. The craniopharyngioma is essentially suprasellar in nature.
Sellar and Suprasellar Meningiomas
Tuberculum sellae meningiomas are relatively common and are a formidable surgical problem (Figs. 4.14 to 4.17). They represent approximately 4% to 10% of all intracranial meningiomas. These tumors arise from the region of the tuberculum sellae, chiasmatic sulcus, limbus sphenoidale, and diaphragma sellae and grow in a subchiasmatic location. As with most other cranial base lesions, tuberculum sellae meningiomas have a relatively innocuous clinical presentation despite their commonly large size. The neurologic, visual, and long-term outcomes are determined by the success of the surgical endeavor. The extent of surgical resection will determine tumor recurrence and regrowth. If they are treated properly and in a timely manner, the results of surgery are gratifying and the long-term outcome is extremely good. Conversely, any surgical mishap can lead to a disastrous outcome. Intradural origin and ease of neurovascular dissection make them well suited for a transcranial approach.
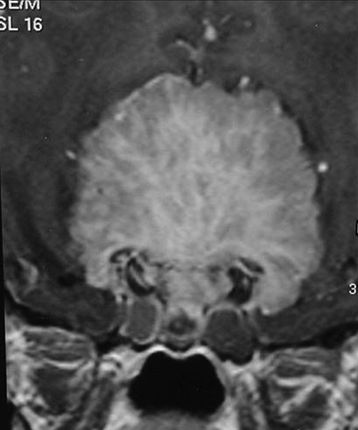
FIGURE 4.14 Contrast-enhanced T1-weighted coronal MRI showing a suprasellar meningioma.
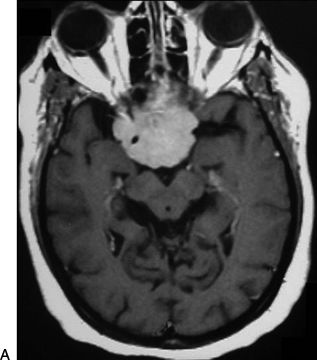
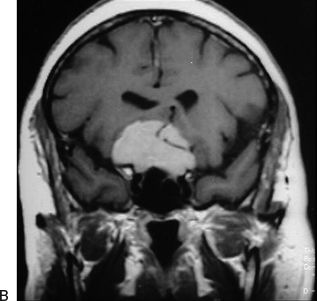
FIGURE 4.15 A. Axial contrast-enhanced T1-weighted MRI of a suprasellar meningioma showing encasement of the internal carotid artery. B. Coronal contrast-enhanced T1-weighted MRI showing a meningioma having encasement of the anterior cerebral artery.
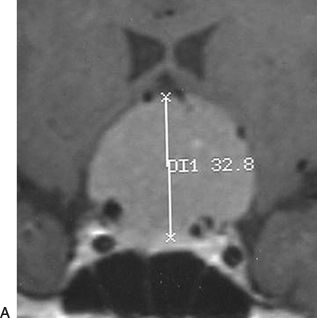
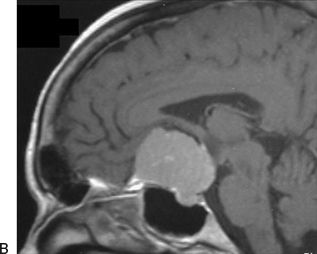
FIGURE 4.16 A. Coronal contrast-enhanced T1-weighted MRI showing a typical tuberculum sellae meningioma. B. Sagittal contrast-enhanced T1-weighted image of MRI showing the meningioma. The pituitary gland can frequently be seen discrete of tumor.


FIGURE 2.17 A. Axial CT scan showing a calcified suprasellar meningioma. B. Coronal CT scan showing the suprasellar calcification.
Nasopharyngeal Angiofibromas
These lesions are primarily extracranial and extradural (Figs. 4.18 and 4.19). In larger lesions, the basal bones are eroded, thinned out, and elevated superiorly. Dural and cavernous sinus involvement is usually in the form of superior elevation and seldom as invasion. The entire cavernous sinus with its contained neural and vascular structures is pushed superiorly by the tumor. This character of the tumor assists in developing a plane between the tumor and basal dura even with blunt dissection. Although transcranial approaches have been described and become popular, an extracranial approach is the rational surgical approach in a vast majority of these cases.
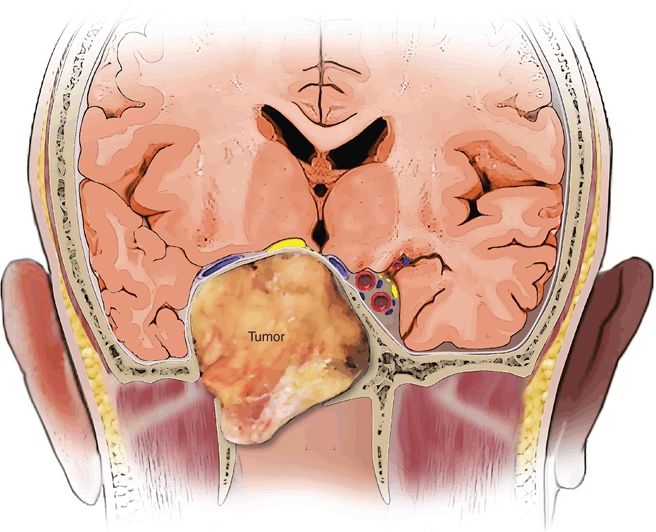
FIGURE 4.18 Line drawing showing characteristic meningeal relationships of nasopharyngeal angiofibromas. The tumors are not only extradural but are also extracranial in nature.