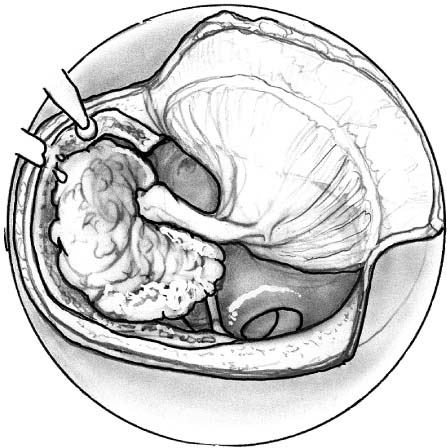
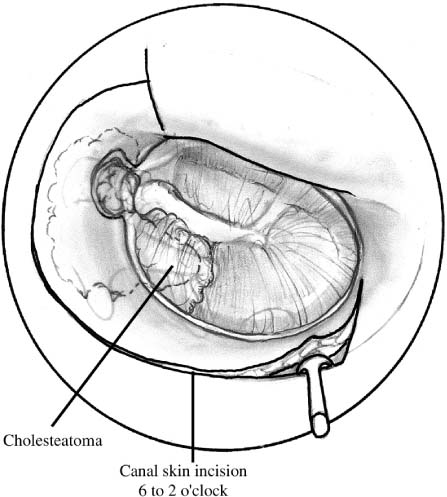
Chapter 7 Transcanal procedures for the removal of cholesteatoma are the most direct approach for the removal of disease originating in the middle ear and epitympanum, and the hypotympanum. Frequently the cholesteatoma is confined to this area of the temporal bone and does not involve the mastoid. The exposure of disease involving the epitympanum and middle ear using a transcanal approach permits the complete removal of cholesteatoma, reconstruction of the tympanic membrane, and ossicular chain, avoiding unnecessary mastoid surgery.1,2 If more extensive disease is encountered, however, then these approaches can be expanded to allow the removal of cholesteatoma involving the mastoid. The anterior atticotomy is used when cholesteatoma originates from an attic retraction pocket, which is not thought to extend beyond the aditus into the mastoid antrum, or if the extent of disease is unknown. It is also useful in the management of cholesteatoma associated with tympanic membrane perforations, or involving the ossicular chain, and congenital cholesteatoma originating in the middle ear. Other indications include the management of congenital conductive hearing loss with middle ear reconstruction, ossicular chain problems, and facial nerve injuries in the middle ear and mastoid segments.3–7 In the evaluation of an attic retraction pocket computed tomograms of the middle ear and attic may be useful, but not mandatory, in determining the extent of the disease process and whether the mastoid is involved. Complete audiometric evaluation should be confirmed by tuning fork test. The anterior atticotomy allows direct visualization of disease involving the epitympanum for the aditus, fossa incudis, and forward to the eustachian tube. Removal of the body of the incus and head of the malleus permits direct visualization of all disease in the epitympanum and protympanum. In the middle ear the posterior extent of the approach is the vertical facial nerve. The use of the 30-degree and 70-degree 4-mm endoscopes, following the removal of cholesteatoma, allows for direct inspection of the mastoid antrum, sinus tympani, and posterior tympanic recesses, ensuring the complete removal of the cholesteatoma.8 Intraoperative facial nerve monitoring is useful in the transcanal removal of cholesteatoma, particularly as one approaches the level of the drum. The anterior atticotomy may be performed using an endaural (preferred) or postauricular incision. It is necessary to have wide exposure of the external auditory canal. The tympanomeatal flap is extended anterior to the short process of the malleus, at the 2 o’clock position in a right ear and the 10 o’clock position in a left ear (Fig. 7–1). Depending on the extent of middle ear involvement, the tympanomeatal flap may be folded inferiorly or removed completely, ensuring adequate exposure of the pathology. The skin of the anterior and inferior canal may be elevated lateral or medial depending on the surgeon’s preference. FIGURE 7–1 For the anterior atticotomy, the tympanomeatal flap is extended anterior to the short process of the malleus. In a right ear the tympanomeatal flap is made circumferentially around the posterior canal from the 6 o’clock position to the 2 o’clock position. The ear canal is circumferentially enlarged with straightening of the anterior canal wall to expose the anterior drum and annulus. The posterior canal wall is thinned until air cells are seen through a thin layer of bone. Do not drill into the mastoid air cells, as this may lead to postoperative drainage. The roof or the canal is elevated to the level of the tegmen. The tegmen is followed medial to the scutum and lateral attic wall. The tympanic membrane and short process of the malleus are guides to the depth of bone removal. The scutum, the lateral attic wall, is thinned using a diamond or polishing bur rotating away from the malleus, clockwise in a left ear and counterclockwise in a right ear. The egg-shelled lateral attic wall is elevated away from the cholesteatoma sac and the heads of the malleus and incus, which are 0.5 to 1 mm medial to the lateral attic wall2(Fig. 7–2). With removal of the scutum, cholesteatoma is exposed in the attic from the fossa incudis, the aditus, and forward to the protympanum, above the eustachian tube. Once the drum is elevated, the incudostapedial joint is separated and the incus removed. Cholesteatoma is dissected from the epitympanum. The head of the malleus is amputated to access disease in the protympanum. FIGURE 7–2 The tegmen is followed medial to the level of the drum and short process of the malleus with thinning of the scutum and posterior canal wall. The scutum and posterior canal wall are egg-shelled and then elevated away from the cholesteatoma and ossicles. Cholesteatoma is exposed in the middle ear and epitympanum from the aditus, the fossa incudis, forward to the protympanum, above the eustachian tube. Greater exposure of the oval window, posterior middle ear, and sinus tympani can be obtained by removing the posterior annulus and medial bony canal wall back to the vertical facial nerve. The pyramidal segment of the facial nerve, superior to the oval window and the chordae tympani nerve, serves as a guide to the vertical facial nerve (the lateral genu of the facial nerve is approximately 1 to 3 mm posterior to the tympanic annulus at the fossa incudis and up to 8 mm posterior to inferior tympanic annulus).9 The technique for safely removing the posterior annulus is with the drill rotating away from the stapes, clockwise in a right ear and counterclockwise in a left ear. Strokes with the drill are from inferior to superior, toward the stapes. This reduces the risk of the drill running into the stapes and facial nerve.5 With anterior thinning of the posterior canal wall and removal of the annular rim, wide exposure of the middle ear and attic are obtained (Fig. 7–3).
TRANSCANAL APPROACHES TO CHOLESTEATOMA
TRANSCANAL ANTERIOR ATTICOTOMY
INDICATIONS
PREOPERATIVE EVALUATION
EXPOSURE
SURGICAL PROCEDURE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


