Topical and Systemic Antiviral Agents
Steven A. Teich
Tony W. Cheung
Antiviral chemotherapy has lagged behind the development of antibiotics for bacterial infections. Because bacteria are relatively complex self-replicating organisms, they have many metabolic differences from mammalian cells that can be selectively attacked by drugs. Viruses, however, are much more primitive. As obligatory intracellular parasites, viruses replicate only by invading a cell and utilizing the host’s biochemical mechanisms to synthesize new viral proteins and genetic material. Until recently, it was difficult to find drugs that would inhibit viral functions without also damaging the host cell. Over the past 2 decades, however, the recognition of viral enzymes and proteins that can serve as molecular targets for drugs has revolutionized the treatment of viral infections. All currently available antiviral agents are virustatic and require an intact immune system to maintain the suppression of many viral infections.
Topical ophthalmic therapy for herpes simplex virus (HSV) infections has been available since 1962 (i.e., idoxuridine, vidarabine, and trifluridine), but it is only in the past 20 years, with the advent of acyclovir, that there is relatively safe and effective systemic treatment of herpetic infections (Table 1). Other systemically administered antiviral agents include ganciclovir, valacyclovir, famciclovir, valganciclovir, foscarnet, cidofovir and interferons. The development of these agents is especially timely for the ophthalmologist in view of the occurrence of new herpetic infections such as the acute retinal necrosis (ARN) syndrome. In addition, as a result of the acquired immunodeficiency syndrome (AIDS) caused by the human immunodeficiency virus (HIV), the ophthalmologist may be treating more severe and frequent infections caused by HSV and varicella zoster virus (VZV). A once rare retinal infection, cytomegalovirus (CMV) retinitis also occurs in these immunosuppressed patients.
TABLE 1. Topical Antiviral Agents for Ophthalmic Therapy | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
The ophthalmic uses of topical and systemic antiviral agents are discussed in this chapter. Antiretroviral agents and those agents that do not at this time have ophthalmic uses are not discussed.
IDOXURIDINE
Idoxuridine (5-iodo-2′-deoxyuridine; IDU) became the first clinically effective antiviral agent when it was shown to be useful for the topical treatment of HSV epithelial keratitis.1,2,3,4,5,6,7 It has been supplanted by the related, but more effective, thymidine analog trifluridine (Fig. 1).
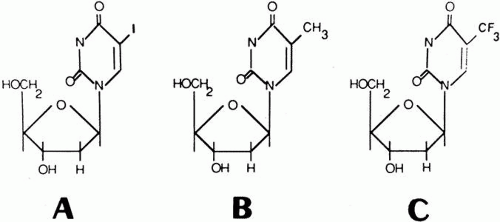 Fig. 1. Chemical structure of the thymidine analogs idoxuridine (A) and trifluridine (C) and of thymidine (B). |
MECHANISM OF ACTION, PHARMACOLOGY, AND TOXICITY
IDU is a pyrimidine analog that closely resembles thymidine. It is active against HSV and poxviruses. IDU depends for its antiviral activity on conversion to the triphosphate form, which mimics thymidine triphosphate and becomes incorporated into viral and mammalian DNA. The initial step is monophosphorylation by either cellular or virus-encoded thymidine kinase. The monophosphate is then converted to IDU triphosphate by cellular enzymes Incorporation of IDU triphosphate into viral DNA results in faulty transcription of viral proteins with inhibition of viral replication. This process is relatively selective in that thymidine kinase activity is higher in HSV-infected cells. This accounts for IDU’s usefulness as a topical agent in the treatment of HSV epithelial keratitis. Due to inhibition of uninfected cells,8 however, the therapeutic ratio is narrow and IDU is too toxic for systemic use.9
IDU is relatively insoluble, penetrates the stoma poorly, and is rapidly metabolized into an inactive form. At room temperature, early preparations of IDU lost in vitro antiviral activity owing partly to inhibition by its major degradation product.10,11 However, commercial preparations are reasonably stable at room temperature so that refrigeration is unnecessary.
Experimentally, IDU causes toxic changes in regenerating corneal epithelium that are not sufficient to result in a slower rate of epithelial wound closure. However, the toxicity does result in decreased stromal wound strength.12 IDU in clinical use is toxic or sensitizing in 5% to 8% of patients.13 Its use has been associated with chronic follicular conjunctivitis, conjunctival scarring, punctate keratopathy, pseudodendrites, corneal edema and opacities, indolent ulceration, punctal and canalicular stenosis, narrowing of meibomian gland orifices, and contact dermatitis of the lids.13,14,15,16 Topical IDU is teratogenic in rabbits.17 This may limit its use during pregnancy.
OPHTHALMIC USES
IDU was first demonstrated to be beneficial in the treatment of herpetic keratitis in rabbits and humans by Kaufman and co-workers in 1962.1,2 Subsequent double-blind studies confirmed the efficacy of IDU treatment in acute superficial epithelial keratitis due to HSV.3,4,5,6 Epithelial keratitis resolved in 55% to 80% of cases treated with IDU.2,3,4,5,6,18,19,20,21,22,23,24 IDU is most effective when used early in acute keratitis.2,3,4 However, IDU does not prevent future recurrence of disease.2,4,5 It is also ineffective in the treatment of HSV-related iritis or stromal disease.2,5,6 This is possibly related in part to the drug’s poor stromal penetration as well as to immunologic factors. A recent meta-analysis concluded that topical trifluridine, acyclovir, and vidarabine were significantly more effective than IDU for dendritic epithelial keratitis.%24a
IDU’s poor solubility adversely effects its potential antiviral activity.16 It is formulated as a 0.1% solution and a 0.5% ointment. The recommended regimen for HSV epithelial keratitis is 1 drop hourly during the day and every 2 hours at night. The frequency may be reduced in half once there is substantial healing.2 Alternatively, the ointment may be used every 4 hours during the day and once at bedtime. Treatment should be continued for at least 3 to 5 days after healing appears to be complete (to reduce the risk of disease reactivation2) up to a maximum of 14 to 21 days.
If a dendritic or ameboid ulcer fails to heal in 14 days, the possibilities of drug toxicity,13,14,15,16 other disease, or viral resistance to IDU must be considered.25 Resistance to IDU may result from a mutation in HSV leading to a loss of thymidine kinase or production of altered thymidine kinase.26
IDU has been replaced by trifluridine, which is more potent and less toxic, for the treatment of herpetic keratitis. It is no longer generally available.
TRIFLURIDINE
Trifluridine (5-trifluoromethyl-2′-deoxyuridine, trifluorothymidine), like IDU, is a thymidine analog, but it is a far more potent antiviral agent than IDU. Originally synthesized as an anticancer agent,27 it was too toxic for systemic use28 but was found to be effective topically for the treatment of HSV keratitis.29 Trifluridine is the drug of choice for the topical treatment of herpetic epithelial keratitis.
MECHANISM OF ACTION, PHARMACOLOGY, AND TOXICITY
Trifluridine differs from IDU in that a trifluoromethyl group, instead of iodine, is present at the 5-carbon position of the thymidine base (see Fig. 1).28 As with IDU, its antiviral activity depends on triphosphorylation. It is first converted to an active form by way of monophosphorylation by both cellular and viral-encoded thymidine kinases. Because trifluridine monophosphate is a potent inhibitor of cellular thymidylate synthetase, less deoxythymidine monophosphate is formed for the drug to compete against for further phosphorylation. Cellular enzymes then convert trifluridine monophosphate to trifluridine triphosphate. This is incorporated into both viral and cellular DNA; however, viral DNA polymerase utilizes trifluridine triphosphate more efficiently than does host cell DNA polymerase. The incorporation of trifluridine triphosphate into viral DNA causes faulty transcription of messenger RNA and the production of abnormal viral proteins, leading to the inhibition of viral replication. Trifluirdine’s relatively selective antiviral activity is due mainly to the marked increase in thymidine kinase activity in virus-infected cells.28
Trifluridine is active in vitro and in vivo against HSV-1 and HSV-2%6a,29,30,31 and vaccinia32 and in vitro against CMV33 and some strains of adenovirus.34 It is more potent than IDU against HSV.20
Trifluridine is ten times more soluble than IDU30 and considerably more soluble than vidarabine,35 enabling it to be formulated as a 1% solution. Trifluridine can penetrate the rabbit cornea and reach the aqueous, especially if the epithelium is absent.36 In humans, topical trifluridine does not penetrate healthy corneas,35 but significant amounts of unmetabolized drug reach the aqueous through diseased corneas.37 This has not yet, however, translated into proven efficacy for the treatment of herpetic stromal keratitis or uveitis. Systemic absorption with topical use of trifluridine is negligible, and the drug is rapidly metabolized in plasma with a short half-life.38
Topical trifluridine is generally well tolerated. Like IDU, it causes toxic changes in regenerating corneal epithelium but does not retard the closure of epithelial defects. It appears to decrease the strength of stromal wounds to a lesser degree than does IDU.12 Although one might suppose that since trifluridine is relatively more selective than IDU in inhibiting cellular metabolism in viral-infected cells, it would have less chemical toxicity; however, this has not yet been conclusively demonstrated in clinical trials.16,18,19,20,21 Toxic actions in the eye are similar to those of IDU and include punctate keratopathy (especially after 2 weeks of use), filamentary keratopathy, epithelial and stromal edema, punctal narrowing, and contact blepharodermatitis.14,15,39 There is a possible association of chronic trifluridine usage with conjunctival cicatrization,39a anterior segment ischemia,40 and corneal epithelial dysplasia.%40a Intravitreal injections of up to 200 μg and vitrectomy solutions containing up to 60 μg/mL trifluridine were nontoxic to the rabbit retina, but higher concentrations caused retinal toxicity.41 Trifluridine is too toxic and mutagenic to be used systemically.28,38,42 Although trifluridine was teratogenic when injected directly into chick embryo yolk sacs,43 more importantly, topical application to the eyes of pregnant rabbits produced no teratogenic effects.17 It is, therefore, unlikely that topical trifluridine in the recommended dosages would, if used during pregnancy, cause fetal damage. Nevertheless a safe dose has not been established for the human embryo or fetus. This agent should be used cautiously during pregnancy and only if the potential benefits outweigh the potential risks. There is no cross-sensitivity of trifluridine with either IDU or vidarabine, thus allowing it to be used effectively in the treatment of herpetic keratitis in patients allergic to either of these two agents.19,20,21,44,45
OPHTHALMIC USES
Trifluridine is the drug of choice for the treatment of HSV epithelial keratitis. It is supplied as a 1% ophthalmic solution. The recommended dosage is 1 drop every 2 hours while awake (with a maximum of 9 drops daily) until healing is complete. This is followed by 1 drop every 4 hours for 7 days (minimum of 5 drops daily) to prevent reactivation of disease.39 Therapy should generally not be continued for more than 21 days. In most studies, trifluridine has successfully healed over 95% of herpetic superficial corneal epithelial ulcers within 2 weeks,16,18,19,20,21,39,45 despite the fact that in some studies trifluridine drops were used suboptimally (only five times daily).18,21,37 If there is no improvement after 7 days or if reepithelialization is not complete within 14 days, the use of other antiviral therapy as well as possible drug toxicity or another diagnosis should be considered. Trifluridine is the only topical antiviral agent that has been demonstrated in a controlled study to be superior to debridement in the treatment of herpes simplex dendritic keratitis.46
Randomized studies have demonstrated trifluridine to have a statistically significant better success rate than IDU in healing herpetic corneal epithelial disease, although the average healing time of about 6 days is similar for both drugs.18,19 Data from the manufacturer indicate that in comparison studies trifluridine heals 96% of dendritic and 88% of geographic ulcers compared with 84% and 41%, respectively, for IDU.38 Trifluridine is also superior to IDU in suppressing viral growth when concomitant corticosteroids are used.19,21
Trifluridine is at least as effective as topical vidarabine ointment in the treatment of herpetic dendritic keratitis. Comparative studies have not demonstrated a statistically significant difference in the success rate of these two highly effective agents.37,47,48 In the two randomized studies, however, trifluridine was administered either less frequently39 or in a different formulation47 than is currently recommended. Trifluridine was believed in one randomized study to be superior to vidarabine for the treatment of geographic ulcers.49
Trifluridine is generally effective against IDU and/or vidarabine-resistant HSV epithelial keratitis.19,20,21,44,45,50 True clinical resistance of HSV to trifluridine is rare.16,51 Treatment of HSV epithelial keratitis with trifluridine, as with all other antiviral agents, has no effect on the subsequent recurrence rate.52 Despite trifluridine’s apparent benefit in experimental herpetic stromal keratitis,53 there is no clinical evidence that it or any topical antiviral drug is effective in the treatment of HSV stromal keratitis or keratouveitis.16,39 However, trifluridine cover allows topical corticosteroid therapy (which has proved beneficial in stromal keratitis) by preventing epithelial disease from developing when the drugs are co-administered for 10 weeks.54
Trifluridine does not affect the course of adenoviral keratoconjunctivitis.55 It is recommended for the treatment of vaccinia keratitis,13,32,%55a although there has been no conclusive demonstration of its effectiveness. This condition is now rare because vaccinia virus vaccinations were halted, but it may reappear as this vaccine is reintroduced in response to bioterrorism.
VIDARABINE
Vidarabine (9-β-D-arabinosyladenine; adenine arabinoside; ara-A) was the second agent licensed for topical treatment of HSV epithelial keratitis. It was the first antiviral agent to be licensed for systemic use against life-threatening viral infections (i.e., HSV encephalitis), but it has been replaced for this use by acyclovir, which is more effective, less toxic, and more easily administered.
MECHANISM OF ACTION, PHARMACOLOGY, AND TOXICITY
Originally synthesized as a potential anticancer agent, vidarabine is obtained from fermentation cultures of Streptomyces antibioticus.56 Vidarabine is a purine nucleoside analog that resembles deoxyadenosine but has an abnormal sugar (Fig. 2). It has in vitro activity against certain DNA viruses including herpesviruses, poxviruses, and probably hepatitis B virus.%6a,57,58,59,60 Cellular enzymes convert vidarabine to the triphosphate form, which acts as a competitive inhibitor of DNA polymerase. This effect is greater on herpes virus-induced than cellular DNA polymerase. The triphosphate derivative may also be incorporated into herpesvirus DNA, where it acts as a chain terminator. Unlike IDU, trifluridine, or acyclovir, vidarabine does not require viral thymidine kinase for its phosphorylation.60 Therefore, vidarabine might be expected to have high activity against thymidine kinase–deficient mutants of HSV.61,62,63 Because it does not selectively inhibit virally induced enzymes, however, there exists a potential for cellular toxicity especially at high doses.60 Vidarabine is relatively insoluble and for ocular use is formulated as a 3% ointment. Vidarabine is rapidly deaminated to hypoxanthine arabinoside (ara-Hx), which is more soluble but has much less antiviral activity.60,64 Topically administered vidarabine does not penetrate intact corneal epithelium, and even in diseased corneas only nontherapeutic amounts of ara-Hx can be found in the aqueous.36,65 About 50% of an intravenous dose appears in the urine in 24 hours, mainly as ara-Hx.66 The dosage must therefore be lowered in the presence of renal dysfunction. Because of vidarabine’s poor solubility, it must be administered as a continuous intravenous infusion in large fluid volumes over 12 hours. Vidarabine and its metabolites are widely distributed in body fluids and tissues, including the brain and cerebrospinal fluid.60 Minimally effective aqueous humour levels of vidarabine and ara-Hx were found after a few days of intravenous therapy at a dosage of 20 mg/kg/day in patients with HSV keratouveitis.67 The recommended intravenous dose is 10 to 15 mg/kg/day for up to 10 days for life-threatening HSV infections.
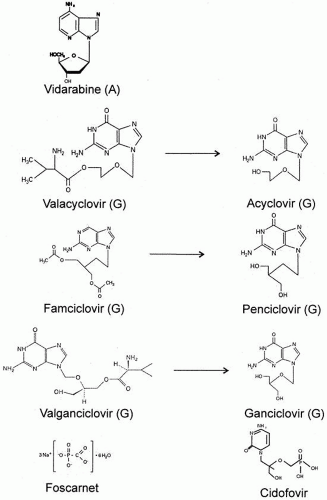 Fig. 2. Chemical structures of systemic antiviral agents. A, adenine analog; G. guanosine analog. |
Topically administered vidarabine does not retard the closure of corneal epithelial defects but weakens stromal wounds to the same degree as IDU. It is less toxic than IDU to regenerating corneal epithelium in animals.68 Clinically, the ocular toxicity of vidarabine ointment appears to be similar to that of IDU.22,23,24 Although some investigators believe that ocular toxicity is less frequent than with IDU, this remains to be proven.51 There is no cross-sensitization of vidarabine with either IDU or trifluridine.21,22,44
The major adverse reactions with systemic use are gastrointestinal (anorexia, nausea, vomiting, and diarrhea), which occur in 10% to 15% of patients. Central nervous system disturbances occur in 2% to 10% and can be severe.59,60,69,70 Ocular flutter has been reported in a patient with AIDS who was receiving vidarabine.71 Neurotoxicity is increased in the presence of renal dysfunction or when the drug is given in combination with either interferon%71a or the xanthine oxidase inhibitor allopurinol (owing to its inhibition of ara-Hx metabolism).72 Elevations in serum bilirubin and aspartate levels may occur, and hematologic toxicity occurs at higher dosages.59 Vidarabine, given parenterally, is teratogenic in animals and must be used with extreme caution in women of child-bearing age.73 Although there is minimal systemic absorption of the topical ocular preparation, this, too, should only be used in pregnancy if the potential benefits outweigh the potential risks.
SYSTEMIC USES
Vidarabine is beneficial in the treatment of HSV encephalitis74 and in VZV infections in immunosuppressed adults75,76,%76a However, acyclovir is equal or greater in efficacy and is less toxic.%76a,79
Vidarabine and acyclovir are equally effective for the management of neonatal HSV infections.80 Vidarabine is without proven benefit in the treatment of systemic CMV disease in neonates and renal transplant patients.81,82,83 Vidarabine’s role is that of a “back-up” drug for serious HSV and VZV infections should resistance to safer and more effective drugs occur.62
OPHTHALMIC USES
Vidarabine ophthalmic ointment is highly effective in the topical treatment of HSV epithelial keratitis. It is at least as effective as IDU ointment in randomized controlled studies. Although most of these studies have revealed a higher percentage of healed ulcers with vidarabine treatment (and one demonstrated a better visual acuity with vidarabine24), the differences have not been statistically significant.22,23,24,84 In randomized trials, vidarabine was about as effective as trifluridine against HSV dendritic keratitis39,47,48 but possibly less effective against geographic ulcers.49 Vidarabine is also effective in the treatment of IDU-unresponsive HSV epithelial keratitis.23,24 A meta-analysis concluded that vidarabine was superior to IDU and equivalent to topical acyclovir and trifluridine in relative efficacy for dendritic epithelial keratitis.%24a In common with other topical antiviral agents, it is not beneficial in the treatment of HSV stromal keratitis and/or iritis.39,49,84 The major use of topical vidarabine, therefore, appears to be for the treatment of HSV epithelial keratitis in patients intolerant of, or unresponsive to, trifluridine. It is recommended that the 3% ophthalmic ointment be applied five times daily at 3-hour intervals. Following re-epithelialization, treatment should be continued for 7 days at a reduced dosage, such as twice daily. Therapy should not be continued for more than 21 days. If there are no signs of improvement after 7 days, or complete healing by 21 days, alternative therapy or the possibilities of drug toxicity or other diagnoses should be considered.
Topical vidarabine is of no benefit in the treatment of adenovirus keratoconjunctivitis, but it may possibly have an effect on vaccinia keratitis.22,%55a
Intravenous vidarabine has a very limited role in the treatment of ocular HSV infections, both because of the effectiveness of topical agents in HSV corneal disease and because of the superiority and relative ease of administration of acyclovir when systemic treatment is required. Abel and associates67 believed that intravenous vidarabine gave slight improvement in HSV stromal keratouveitis, but there was no long-term follow-up. HSV retinitis in a renal allograft recipient transiently improved with the use of intravenous vidarabine in conjunction with a reduction of the patient’s immunosuppressive medications.85 In an uncontrolled trial of intravenous vidarabine for CMV retinitis in pharmacologically immunosuppressed patients, some improvement was suggested in four of seven cases. However, the beneficial effect was often transient, high doses (20 mg/kg) were required to suppress (but not eliminate) urinary viral excretion, and there were serious associated gastrointestinal, hematologic, and neurologic side effects.86 This therapy cannot, therefore, be recommended. A case of disseminated VZV with bilateral retinitis (suggestive of the acute retinal necrosis syndrome) in an immunocompromised patient was apparently successfully treated with a combination of intravenous vidarabine and acyclovir after therapy with each agent alone had failed.87 As in systemic disease, intravenous vidarabine for serious herpesvirus ocular disease has been replaced by safer and more effective agents.
ACYCLOVIR
Acyclovir (9-[2-hydroxyethoxymethyl] guanine) has proved to be an extremely safe and effective agent and is a drug of choice for most forms of HSZ and VZV infections. Its availability in topical, oral, and intravenous preparations allows its use in a wide range of clinical situations. However, its poor oral absorption has spurred the development of valacyclovir and famciclovir.
MECHANISM OF ACTION, PHARMACOLOGY, AND TOXICITY
An acyclic analog of guanosine (see Fig. 2), acyclovir is the prototype of a generation of specific antiviral drugs that are activated by a viral thymidine kinase to become potent inhibitors of viral DNA polymerase.88 The drug inhibits in vitro, in order of decreasing effect, HSV-1 and HSV-2, VZV, Epstein-Barr virus (EBV), human herpesvirus 6 (HHV-6), and CMV.89 (In vivo it does have some activity against CMV.90) Its in vitro activity is 160 times greater than that of vidarabine.91 Acyclovir’s antiviral spectrum is, however, limited to the herpesvirus group.
Acyclovir must be phosphorylated to the nucleotide form, acyclovir triphosphate to exert its antiviral activity. It is first selectively phosphorylated to acyclovir monophosphate by viral thymidine kinase produced only in infected cells. Cellular kinases then convert acyclovir monophosphate to the triphosphate form.92 Acyclovir triphosphate is found in HSV-infected cells at concentrations 40 to 100 times greater than in uninfected cells.93 That the drug is functional predominantly in infected cells explains its very low toxicity. Human CMV is relatively insensitive to acyclovir because it does not encode for viral thymidine kinase and is, therefore, inhibited only with a median inhibitory dose (ID50) similar to that of the host’s cells.89 Acyclovir triphosphate is both an irreversible inhibitor of, and a substrate for, viral DNA polymerase94 and has a greater affinity for viral DNA polymerase than for cellular DNA polymerase. In addition, the incorporation of acyclovir triphosphate into a growing DNA chain results in chain termination because it lacks a 3′ hydroxyl group and, therefore, no attachment point for the next link. Because EBV, which does not produce herpes-directed thymidine kinase, is sensitive in vitro to acyclovir, additional mechanisms of action may exist.95,96
Acyclovir can be administered topically (although not formulated for ophthalmic use in the United States), intravenously, and orally. The dosage is timed to achieve drug levels in the extracellular fluid that are greater than the ID50 for HSV types 1 and 2 (mean, 0.1 to 1.6 μM) and VZV (mean, 3 to 4 μM).88,89,97 Antiviral activity, however, is actually due to intracellular levels of acyclovir triphosphate. With intravenous dosing, the serum half-life is about 3 hours in adults with normal renal function. At a dosage of 5 mg/kg three times a day, serum concentrations are well above the ID50 for HSV-1 and HSV-2, but trough levels fall below the ID50 of many VZV isolates.98 However, a dosage of 10 mg/kg three times a day provides trough levels sufficient for most VZV infections.97,98 Acyclovir is 15% protein bound, and the volume of distribution is 70%, corresponding to total body water.99 The cerebrospinal fluid level is 50% that of plasma.100 Seventy percent of acyclovir is excreted unchanged in the urine through filtration and secretion99; therefore, the dosage must be adjusted in the presence of renal failure. Acyclovir is readily hemodialyzable.88,96
Absorption of orally administered acyclovir is slow and incomplete, with bioavailability of 15% to 30%. Peak plasma levels are reached in 1.5 to 2 hours.89 Steady-state levels after administration of 200 mg orally every 4 hours range from 1.4 μM to 4.0 μM (mean, 2.5 μM).101 Although these levels are inhibitory for HSV-1 and HSV-2, they are near or below the ID50 of VZV, which is one-tenth as sensitive as HSV-2 to acyclovir.97,98 However, 800 mg. orally five times a day yields peak and trough serum levels of 6.9 μM and 3.5 μM, respectively, which have a better clinical effect on VZV.88,102,103,104
Topical acyclovir 3% ophthalmic ointment has the best corneal penetration of any topical antiviral drug. It penetrates intact corneal epithelium to achieve aqueous levels well within the therapeutic range for HSV-1 and HSV-2.37
Clinically significant intraocular concentrations of acyclovir are also achieved following oral or intravenous administration. When 400 mg. is given orally five times a day, tear105,106 and aqueous107 acyclovir levels are produced in excess of the ID50 of HSV-1. The intravitreal acyclovir level 2 hours after an intravenous dose of 13 mg/kg was within the therapeutic range for HSV-1 and HSV-2, VZV, and EBV.108 Intravitreal concentrations of 8.8 to 11.0 μM may result from intravenous acyclovir dosages of 5 mg/kg three times a day.98 Subconjunctival injections of 25 mg result in clinically significant aqueous and vitreous levels109 but cause subconjunctival crystals.
Experimentally, topical acyclovir has no detrimental effect on regenerating corneal epithelium or on the healing of epithelial or stromal wounds. Nevertheless, a compilation of published clinical trials of topical acyclovir did not discover a statistically significant decrease in ocular adverse reactions compared with the other available antiviral drugs.110 One randomized trial found a significantly decreased frequency of superficial punctate keratopathy in acyclovir recipients compared with IDU recipients.111 Other, less common reported complications include burning or stinging, tearing, follicular conjunctivitis, palpebral allergy, and punctal stenosis.110 In patients with ARN who received acyclovir in the infusion fluid during vitrectomy at doses of 10 to 40 μg, there was no evidence of retinal toxicity, but one patient developed a posterior subcapsular cataract.112
Acyclovir is a remarkably safe drug when used systemically for periods as long as 5 years.%112a Toxic effects are predominantly associated with high doses (more than 5 mg/kg) of the intravenous formulation.113 The ρH of the intravenous formulation is 11, and concentrated solutions are caustic. Local irritation, phlebitis, and vesicular lesions may result from subcutaneous infiltration.114,115 Such reactions can be circumvented by infusing acyclovir at a concentration no greater than 6 mg/mL.116 Acyclovir’s major adverse effect is on renal function. This is due to crystallization and deposition of the drug in the kidneys of patients who are dehydrated or have preexisting renal insufficiency.117 Renal dysfunction can be avoided by infusing acyclovir slowly over 1 hour and administering 1 liter of fluid with each gram of the drug.116 Oral acyclovir has rarely been associated with renal dysfunction.118 Nausea, vomiting, and abdominal pain can occur and probably represent a direct toxic effect on the gastrointestinal tract.113 There is one report of diarrhea, presumably caused by the presence of lactose in oral acyclovir tablets, which responded to oral lactase administration.119 Rare reports of central nervous system toxicity or psychiatric disturbances have occurred, mainly in association with the use of other neurotoxic agents or in the presence of renal disease.118,120,121,122,123,124 Hypersensitivity reactions, typically transient maculopapular rashes near infusion sites, occur in less than 1% of patients.116 Acyclovir can be incorporated into DNA, which has raised some concern over its possible mutagenicity. There is no significant evidence that acyclovir is a carcinogen.125,126 At much higher than clinically relevant doses, acyclovir has been teratogenic in animals,127 but other animal studies indicate that it is not a significant teratogen.88,128 Although there is no clinical evidence indicating teratogenicity,129 acyclovir does cross the placenta130 and its safety in pregnant women or in neonates has not been established.131
SYSTEMIC USES
Acyclovir is safe and effective for most HSV and VZV infections. It is both less toxic and more efficacious than vidarabine in the treatment of HSV encephalitis.78,79 It can reduce mortality from 70% to nearly 20%. The usual dosage for HSV encephalitis is 10 mg/kg every 8 hours for at least 10 to 14 days.132 Acyclovir is comparable to vidarabine in the treatment of neonatal HSV infections80 but is easier to administer. A number of placebo-controlled, double-blind clinical trials have demonstrated the therapeutic efficacy of acyclovir in the treatment of primary genital HSV infections.133,134,135,136 Oral and intravenous treatment are superior to topical treatment.134 The usual oral dosage is 200 mg five times daily or 400 mg three times daily for 10 days.
Oral acyclovir for 5 days is only modestly effective in treating genital or orolabial HSV recurrences in immunocompetent adults.137,138 However, chronic oral acyclovir reduces the frequency of recurring genital HSV infection.%138a Doses of 400 mg twice daily are convenient and well tolerated.%112a,139,140 Unfortunately, following completion of acyclovir therapy, patients may return to their previous pattern of recurrent infection. Topical acyclovir 5% cream%140a slightly decreases the duration of an episode of orolabial herpes. Oral acyclovir started within 3 days of onset of herpetic gingivostomatitis in young children significantly shortens the course of the disease.%140b
Systemic acyclovir in various regimens can successfully prevent and treat mucocutaneous HSV infections in immunosuppressed patients.141,142,143,144,145,146,147 However, recurrences commonly occur following the cessation of therapy.
Acyclovir is also of established benefit and preferable to vidarabine in the treatment of VZV infections in immunocompromised patients when given intravenously for 7 days at a dosage of 10 to 12 mg/kg every 8 hours.77,148,149,150,151,152
The indications for using acyclovir to treat VZV infections in immunocompetent adults and children with nonophthalmic disease are less obvious. Intravenous acyclovir benefits adults when administered within 72 to 96 hours of the onset of symptoms.150,152 Oral acyclovir, given as 400 mg five times a day, is clinically ineffective in VZV infections in immunocompetent patients.102,153 However, higher doses of up to 800 mg five times a day have had some benefit when initiated within 48 to 72 hours of exanthem and are of proven efficacy in treating herpes zoster ophthalmicus (HZO).153,154,155,156,157,158 A meta-analysis of 4 placebo-controlled trials of oral acyclovir 800 mg. 5 times daily for 7 or 10 days concluded that acyclovir accelerates pain resolution, especially in those aged 50 or older.%158a Treatment should be strongly considered for those over 50 years of age or with moderate to severe pain and definitely for ophthalmic zoster. Some consider therapy optional in young patients with uncomplicated disease.
Studies suggest that high-dose oral acyclovir, if given within 24 hours of exanthem, reduces the severity and duration (by 1 day) of primary varicella infections (chickenpox) in normal children,159,160 adolescents,%160a and adults.161 It is not known if this affects the subsequent risk of herpes zoster or if it is cost-effective to treat all patients to shorten slightly the duration of a generally self-limited disease. Treatment should be strongly considered in older patients, who tend to have more severe disease than young children.161 The American Academy of Pediatrics recommends the treatment of varicella with oral acyclovir (20 mg/kg to a maximum of 800 mg 4 times a day) in patients over 13 years of age, children receiving aerosolized corticosteroids, and children older than one year with chronic cutaneous or pulmonary conditions.%161a Treatment of infected household contacts might also be considered.%161b
Prophylactic high-dose intravenous or oral acyclovir may reduce the likelihood and severity of CMV infections in CMV-serononegative renal and CMV-seropositive bone marrow–transplant recipients.162,163 Trials of acyclovir in the treatment of established CMV infections, on the other hand, have shown no consistent benefit in immunosuppressed patients.164,165,166,167
In acute systemic EBV infections (e.g., infectious mononucleosis), acyclovir temporarily suppressed oropharyngeal EBV replication and excretion. The slight clinical benefit, however, does not justify the routine use of acyclovir for this condition.168,169 High-dose oral acyclovir can cause temporary regression of EBV-induced oral hairy leukoplakia in HIV-infected patients.170
Although there is some evidence that Bell’s palsy may result from inflammation of the facial nerve in the temporal bone caused by herpes simplex virus,171 a definitive benefit from oral acyclovir remains controversial. A randomized controlled study demonstrated a modest but statistically significant benefit from acyclovir 200 mg 5 times a day for 5 days plus oral prednisone, compared to prednisone alone.172 The acyclovir group was 1.22 times more likely to have a good recovery, but 17% of patients were lost to follow-up. A recent meta-analysis concluded that acyclovir combined with prednisone is safe and possibly effective in improving outcomes in Bell’s palsy.%172a
OPHTHALMIC USES
Herpes Simplex Virus Infection
Although not commercially available in the United States, topical acyclovir in a 3% ointment is superior to IDU111,173,174 and equivalent to vidarabine175,176,177,178 or trifluridine179,180 in the topical treatment of HSV epithelial keratitis.%24a Although able to penetrate the cornea, it does not prevent stromal disease from developing during the treatment of acute epithelial disease.175,177,178 Oral acyclovir, given as 400 mg five times a day, is equivalent to topical acyclovir105,106,181 in the treatment of HSV dendritic ulceration. Ninety percent of orally treated patients in one study had healing of dendritic ulcers in a median of 5 days.106 In another study, 200 mg five times a day healed epithelial keratitis within 5 to 21 days in 18 of 19 patients with concomitant stromal keratitis or uveitis.182 In most cases of HSV epithelial keratitis, a topical antiviral drug, such as trifluridine, would be preferable to the use of a systemic agent. Although not approved for this use, oral acyclovir may be considered in certain situations.16,183 An oral agent might be more effective in young children, the elderly, the disabled, or others in whom the use of an eye dropper is difficult or impossible, or as an alternative for patients suffering from topical antiviral ocular toxicity. In addition, it may be a useful adjunct to topical trifluridine for the treatment of HSV keratitis in eczema herpeticum.184 In small children, oral acyclovir may be especially useful as an adjunct to topical antivirals (which are diluted by children’s tears). A small, retrospective study of oral acyclovir in children demonstrated healing of epithelial keratitis in all patients (6 of whom also were receiving topical antivirals). It also prevented recurrent disease in those children receiving topical corticosteroids for immune stromal keratitis while they remained on full doses of oral acyclovir.%184a
Prophylactic oral acyclovir is of apparent utility following penetrating keratoplasty in herpetically infected patients for the prevention of HSV reactivation during postoperative corticosteroid therapy.183 Although acyclovir cannot eliminate ganglionic latency, it may reduce viral shedding in this high-risk situation185,186,187; in a rabbit model, it significantly lowered the incidence of keratitis.185 A statistically significant benefit of prophylactic oral acyclovir in decreasing the recurrence rate of herpetic keratitis after penetrating keratoplasty for herpes simplex keratitis was found in a small randomized trial18 (at doses of 800 or 1000 mg daily) and in a larger retrospective study (using 400 mg twice daily).189 Oral acyclovir seems safe and effective for this indication when used for a year or more.188,189,190 As in other situations, the prophylactic effect does not persist once acyclovir is discontinued. Although a large randomized placebo-controlled prospective trial would be needed to confirm these results, this is not likely to be done in view of the proven benefit of acyclovir in preventing herpetic ocular disease in other circumstances.
There has been interest in oral acyclovir for the treatment of herpetic stromal disease and/or keratouveitis. Both active viral proliferation and immunogenic mechanisms appear to play important roles.191 Topical corticosteroids, which are required to suppress the latter, may trigger or exacerbate viral replication.192,%192a,193 In general, topical antivirals used alone have been disappointing in the treatment of stromal keratitis.16,191 Topical acyclovir with a topical corticosteroid may be of possible benefit.194,195 Sanitato and associates196 found the combination of topical and oral acyclovir without the use of topical corticosteroids to be ineffective in the treatment of 17 patients with disciform edema or necrotizing stromal keratitis.
HEDS Studies
In an effort to clarify these and other issues in therapy for herpetic stromal keratitis and iritis, including prevention of recurrent disease, the Herpetic Eye Disease Studies (HEDS) were initiated. These are a series of randomized, prospective, double-masked placebo-controlled multicenter clinical trials that have arrived at important conclusions concerning the use of oral acyclovir. HEDS determined that there is no clinical benefit to a 10-week course of adjunctive oral acyclovir for treating HSV stromal keratitis in patients receiving concomitant topical corticosteroids and trifluridine.197 Similarly, the addition of a 3-week course of oral acyclovir to topical trifluridine treatment of acute HSV epithelial keratitis did not prevent the subsequent development of stromal keratitis or iritis over the following year.198 For the treatment of HSV iridocyclitis, there was a strong suggestion of clinical benefit from a 10-week course of oral acyclovir 400 mg 5 times daily as an adjunct to topical corticosteroids and trifluridine (50% treatment failures with acyclovir vs. 68% with placebo).199 Because of low enrollmentt, this study was stopped prematurely, providing an insufficient number of patients to reach a statistically significant conclusion. There is, however, a clear-cut benefit from long-term suppressive oral acyclovir in preventing recurrent HSV epithelial keratitis and stromal keratitis.200,201 Seven hundred and three immunocompetent patients with prior episodes of ocular HSV disease (blepharitis, conjunctivitis, epithelial or stromal keratitis, or iritis) within the past year but no currently active disease, were randomized to oral acyclovir 400 mg twice daily or a placebo for 12 months. The cumulative recurrence rate of any ocular HSV was significantly reduced from 32% to 19% by acyclovir. The benefit was greatest in those with the most prior episodes. The benefit in preventing stromal keratitis (cumulative probability 14% with acyclovir vs. 28% with placebo), however, was solely in patients with a prior history of stromal keratitis (mainly because the risk is otherwise so low). An additional benefit was the reduction in the cumulative probability of nonocular (primarily orofacial) HSV disease from 19% to 36%. As expected, there was no lasting benefit once oral acyclovir was discontinued, but neither was there a rebound in the rate of HSV disease.
In summary, oral acyclovir 400 mg. five times daily can, in certain situations, be substituted for topical antiviral agents in the treatment of herpetic keratitis. It is of no benefit as short-term adjunctive therapy with topical agents for acute HSV epithelial or stromal disease, but is of likely benefit as adjunctive treatment of HSV iridocyclitis (in which case long-term suppressive therapy should also be considered). It is of proven benefit as long-term suppressive therapy for at least 1 year at a dosage of 400 mg twice daily. However, because HSV epithelial disease is normally responsive to topical therapy, one might consider reserving this for patients with a history of stromal disease, frequent recurrences, or immunosuppression. While there have not been studies in a randomized controlled trial for these indications, one would expect oral valacyclovir or famciclovir to be of at least comparable efficacy, with the advantage of less frequent administration.
Intravenous acyclovir has been used successfully to treat HSV retinitis in an otherwise healthy adult.202 Neither acyclovir nor ganciclovir was beneficial in a fatal case of ascending encephalomyelitis with retinitis and optic neuritis due to herpes B virus infection contracted from a monkey bite or scratch.203
Herpes Zoster Ophthalmicus
Herpes zoster ophthalmicus (HZO) accounts for 10% to 25% of cases of zoster dermatitis.%203a Topical acyclovir alone has given variable results in studies of immunocompetent patients with HZO.204,205,206,207,208 Although some series have suggested a possible benefit of topical acyclovir on epithelial keratitis,204,205,206 randomized controlled studies comparing topical acyclovir with topical corticosteroids have yielded conflicting results.205,207 Some authors suggest that topical corticosteroids may prolong the late inflammatory ocular complications.205 Acyclovir ointment has been of variable benefit in treatment of chronic herpes zoster keratitis in patients with AIDS unresponsive to systemic acyclovir.209,%209a
High doses of oral acyclovir (600 to 800 mg five times a day) have been found effective in reducing the ocular complications of keratitis and uveitis in HZO.154,156,157,210,211 This represents a major therapeutic advance in therapy for a disease for which only palliation was previously available.
Cobo and co-workers156,157 performed a placebo-controlled clinical trial of 71 immunocompetent patients with acute HZO presenting within 1 week of onset of skin lesions and who did not receive oral or topical corticosteroids. They demonstrated that oral acyclovir, at a dose of 600 mg five times a day for 10 days, ameliorated the cutaneous signs and symptoms and decreased the ocular complications. The effect on cutaneous disease, including acute pain, occurred predominantly in patients treated in the first 72 hours, but the incidence and severity of inflammatory ocular complications were reduced even when treatment was begun later independent of initial severity of disease. Compared with placebo, oral acyclovir significantly reduced the incidence of pseudodentritiform keratopathy (from 31% to 14%), stromal keratitis (56% to 25%), and anterior uveitis (56% to 19%). There was no effect on episcleritis or on the development of corneal hypesthesia or neurotrophic ulceration. It was postulated that although the 600-mg dose was beneficial, it may have been near the threshold for effect.155 The persistence of virus-productive disease was evidenced by the development in some patients of new dermatomal lesions and skin microdissemination as well as the recovery of virus from skin lesions as late as 14 days.157 An 800-mg dose might have been even more beneficial, since it gives peak and trough serum levels above the ID50 of VZV and has been effective and well tolerated.103,104,153,158 Other investigators210,211 in randomized studies found that the 800-mg dose given five times daily without corticosteroids for 7 to 14 days reduced chronic ocular complications. One randomized study determined that this dosage given for 7 days was just as effective as 14 days of treatment211; another randomized study of non-ophthalmic zoster found no additional benefit of 21 days over 7 days of therapy.212 Although clinical trials have demonstrated the effectiveness of treatment within 72 hours of rash onset,213 patients may still benefit from later treatment if new vesicles are appearing.157,%161b There has been only a single retrospective study that concluded that acyclovir did not reduce ocular complications.214 The preponderance of evidence, however, indicates that high-dose oral acyclovir does reduce the frequency of ocular complications.157,%158b,210,211,215,216,%216a Furthermore, as noted previously, a meta-analysis of placebo-controlled trials of oral acyclovir 800 mg 5 times daily,%158a which included one trial of patients with HZO,210 confirmed that it shortens the duration of acute pain. A recent chart review of patients with HZO in Olmsted County provides further support for early routine systemic viral therapy. While not randomized or controlled, this study indicated that antiviral therapy may reduce the likelihood of neurotrophic keratitis.%216a The addition of oral corticosteroids to acyclovir remains controversial. It has not been rigorously studied in HZO. In non-ophthalmic zoster, there appears to be a modest effect on reducing acute (but not chronic) pain.212,217 One study found that the combination improved short-term quality of life measures in patients over 50, compared to placebo.217
It has not yet been adequately demonstrated that acyclovir lessens the development of post-herpetic neuralgia., This complication is most common in those older than the age of 50 and especially those aged more than 80.218 Neither 600 mg five times daily for 10 days nor 800 mg five times daily for 7 days had an effect on the incidence, severity, or duration of post-herpetic neuralgia.157,158 In two other placebo-controlled trials (one of HZO), 800 mg given five times daily for 10 days decreased post-herpetic neuralgia at 1 to 3 months but not at 4 to 6 months.153,210 A recent literature review found marginal evidence that antivirals prevent post-herpetic neuralgia.219 Although systemic corticosteroids have been advocated to prevent post-herpetic neuralgia,214 placebo-controlled trials failed to demonstrate a long-term benefit from adding oral corticosteroids to acyclovir.212,217,220
In summary, oral acyclovir therapy is indicated for all immunocompetent patients with HZO at a dosage of 800 mg five times a day for 7 to 10 days.210,211,216 The newer drugs valacyclovir and famciclovir are at least as effective, with the advantage of simpler dosing.221,222,223 Whether this treatment prevents chronic, life-disruptive post-herpetic neuralgia and whether the addition of oral corticosteroids provides additional benefit cannot be answered definitively at this time. Corticosteroids may be considered in patients older than 60 years of age who have no risk for corticosteroid toxicity.%158b
Herpes zoster infections may be more frequent and severe in immunosuppressed patients with an increased brisk of cutaneous and visceral dissemination of encephalomyelitis.224 Intravenous, high-dose acyclovir therapy77,148,149,150,152 is beneficial in these patients. In patients with AIDS or HIV seropositivity, HZO may be the first indication of underlying immunosuppression.225,226,%226a To prevent central nervous system complications, intravenous acyclovir may be considered in high-risk patients with HZO before obtaining the results of HIV testing.227 There is some evidence that immediate high-dose oral acyclovir administered before the development of these complications may be of benefit.228 There is not, however, sufficient information to recommend this approach.224,228 One must be cautious in using oral acyclovir to treat patients with AIDS because of possible malabsorption.229 Retinitis in association with or following herpes zoster may occur in patients with AIDS.230,231,232,233 It can resemble ARN, but the response to intravenous acyclovir treatment is variable. Long-term oral-maintenance acyclovir may be appropriate following intravenous acyclovir therapy of herpes zoster in AIDS patients.%233a
Acute Retinal Necrosis Syndrome
In view of the evidence implicating VZV and HSV as etiologic agents of ARN, acyclovir is a logical therapy.234,235 Pepose and Biron236 determined the ED50 of VZV recovered from the vitreous of a patient with ARN (5.3 μM). Such serum and vitreous levels are achievable with the current intravenous dosage of acyclovir for ARN108,237 but are difficult to maintain with oral therapy.103
Acyclovir given intravenously allows more rapid resolution of the retinitis234,237,238,239 and has become the mainstay of therapy. Because of the relatively uncommon occurrence of this syndrome, a randomized placebo-controlled trial has not been performed. In the first large reported series of treated patients, Blumenkranz and associates237 used intravenous acyclovir (1500 mg/m2/day in three divided doses) for 7 to 21 days, with an average of about 10 days. The average dose was 945 mg every 8 hours. Regression began in about 4 days and was complete on the average in about 1 month. Three of 13 eyes retained 20/30 or better vision and eight could see 20/400 or better. Also, no eye had visual loss due to progressive retinitis or optic neuropathy after 2 days of therapy. In unilateral cases, acyclovir reduced the risk of fellow eye involvement.237,238,239,240,241 Despite acyclovir therapy, the progression of vitritis is common, possibly owing to immunologic processes. Unfortunately, acyclovir does not reduce the incidence of retinal detachment.237 However, some investigators have proposed that the use of acyclovir in the “mild type” of ARN may lessen the risk of retinal detachment.239,240,241,242
The current recommended treatment of ARN is with intravenous acyclovir, 1500 mg/m2/day in three divided doses for 7 to 10 days. It is suggested that oral acyclovir (800 mg five times daily) be continued for 6 to 14 weeks after intravenous treatment, as this is the period of greatest risk of bilateral involvement.234,241 It is reasonable to substitute oral valacyclovir or famciclovir for oral acyclovir at the conclusion of intravenous therapy.243,244,245 In unresponsive cases, the addition of intravitreal injections of ganciclovir and/or foscarnet have been of reported benefit.246 Aspirin and prednisone may be useful adjuncts,234,237,247 but prednisone should not be used until after the initiation of acyclovir therapy.234 Successful acyclovir therapy of ARN without the use of systemic corticosteroids was accomplished in an immunocompetent patient.238 Early prophylactic vitrectomy with intravitreal infusion of acyclovir in doses of 10 to 40 μg, in addition to intravenous acyclovir, has given variable results.112,237,248 Although selected patients might benefit, this therapy cannot be recommended routinely.237
Intravenous acyclovir as monotherapy is ineffective in the progressive outer retinal necrosis (PORN) syndrome caused by VZV in profoundly immunosuppressed AIDS patients. The visual prognosis is guarded with any attempted treatment.232,233,249 There is some evidence that early combination antiviral therapy may improve the outcome, with the combination of ganciclovir and foscarnet seemingly better than acyclovir-containing regimens.250,251
Epstein-Barr Virus Infection
Both acute and chronic EBV infections have been loosely associated with ocular inflammatory disease.252 Experimentally, intraocular levels of acyclovir are therapeutic for EBV infection after subconjunctival, but not topical, administration.109 There are only a few case reports of acyclovir use for presumed ophthalmic EBV infection. Corneal lesions and conjunctivitis resolved in one case of infectious mononucleosis treated with topical acyclovir.253 However, stromal keratitis associated with EBV infection has responded to topical corticosteroids without the use of acyclovir.254,255 One patient had no recurrences of presumed EBV keratitis during or after 6 months of oral acyclovir treatment,256 but this may represent the natural course of the disease. Wong and associates257 reported three cases of bilateral uveitis in patients with chronic EBV disease. Two patients had an improvement in systemic symptoms with the use of intravenous acyclovir; one of these had lessened intraocular inflammation with the addition of topical acyclovir plus topical and systemic corticosteroids. Another patient with chronic EBV infection with interstitial pneumonitis and papilledema was treated with intravenous and oral acyclovir.258 Although the systemic symptoms improved, there was no mention of the response of the optic disc edema. These reports suggest a possible beneficial effect of acyclovir, but further studies are required to determine the role of this drug in treating the ocular manifestations of EBV infection.
Cytomegalovirus Infection
There are no well-documented cases of successful treatment of CMV retinitis with acyclovir. Although regression of CMV retinitis in patients with AIDS has been reported with the use of acyclovir and zidovudine,259 this was believed to represent improved immunologic function caused by the anti-HIV effect of zidovudine in improving CD4 lymphocyte counts. High-dose intravenous acyclovir plus oral zidovudine was of dubious benefit in minimally delaying the recurrence of CMV retinitis in patients with AIDS that was previously treated with ganciclovir.260
RESISTANCE
There are at least three mechanisms of resistance to acyclovir. The most common mutation is loss of synthesis of viral thymidine kinase so that acyclovir is not phosphorylated to its active form.89 A second type of mutation induces thymidine kinase with altered substrate specificity that phosphorylates thymidine but not acyclovir. Finally, a mutation of the viral DNA polymerase gene induces altered DNA polymerase that is not sensitive to inhibition by acyclovir triphosphate.
Acyclovir-resistant HSV and VZV mutants are uncommon in immunocompetent patients.229,261 Isolates of HSV-1 in the United Kingdom obtained from 40 primary ocular infections in immunocompetent patients showed reduced sensitivity in 7.5% and acyclovir-resistance in 2.5%. Sensitivity to IDU and vidarabine was retained.262 A second British study, however, found no resistance of HSV-1 viruses, although one HSV-2 isolate was resistant in vitro to all antiviral agents tested.263 Resistance to acyclovir is becoming more common in immunodeficient patients.229,264 This is especially so in patients with AIDS receiving chronic therapy with acyclovir.61,229,265,266,267 Although many thymidine kinase-deficient HSV mutants appear less neurovirulent and less efficient in establishing ganglionic latency,268 they may cause progressive and severe mucocutaneous disease in immunocompromised patients, especially those with AIDS.61,62,264,267 Some of these patients have been successfully treated with foscarnet or cidofovir which do not rely on phosphorylation by thymidine kinase.61,269,270,271 Continuous intravenous infusion of high-dose acyclovir has also been used successfully in some patients.272,273
Acyclovir-resistant VZV has caused hyperkeratotic skin lesions in HIV-infected patients after long-term oral acyclovir suppressive therapy.229 The viral isolates had deficient or altered thymidine kinase function. Subtherapeutic doses or inadequate courses of acyclovir may have been factors in the development of acyclovir resistance in these cases. Foscarnet may be effective in treating acyclovir-resistant VZV.274
VALACYCLOVIR
Valacyclovir, the L-valyl ester of acyclovir, is a prodrug that is rapidly and nearly completely converted to acyclovir after oral administration. Its excellent bioavailability results in serum acyclovir levels comparable to intravenous acyclovir but requiring less frequent dosing than oral acyclovir. Therefore, it has much the same antiviral indications and safety as oral acyclovir with the advantage of simpler dosing.
MECHANISM OF ACTION, PHARMACOLOGY, AND TOXICITY
Following oral administration and absorption, valacyclovir is nearly completely hydrolyzed to the active moiety acyclovir and L-valine (an essential amino acid) via first-pass intestinal and hepatic metabolism. Its antiviral activity, pharmacodynamic properties, and toxicity are, therefore, essentially those of acyclovir.275,276,277 Valacyclovir, unlike acyclovir, is a substrate for a sterospecific transporter and is wellabsorbed through the gut wall.278 This results in a bioavailability of acyclovir from oral valacyclovir three- to five-fold higher than that of oral acyclovir, ranging from 54% to 70%.222,277,278,279,280,281 Peak acyclovir concentrations averaging 5.65 μg/mL are achieved 1.75 hours after a single oral dose of 1000 mg of valacyclovir.278 Systemic acyclovir exposure (serum area under the curve, or AUC) values after oral valacyclovir 1000 mg three times daily and 2000 mg four times daily are similar to those after intravenous acyclovir 5 mg/kg and 10 mg/kg three times daily, respectively.277,278,282 Food does not affect valacyclovir administration.277 The mean plasma elimination half-life of acyclovir after oral valacyclovir administration is 2.62 to 3.13 hours, consistent with that of intravenous acyclovir.277,278,281 Less than 1% of administered valacyclovir is recovered in the urine, being excreted mainly as acyclovir.278,281 As with acyclovir, dosage modification is required with renal but not with hepatic impairment.277
Valacyclovir is administered only orally. It is well tolerated, with a toxicity profile similar to that of acyclovir. In comparative studies with oral acyclovir in immunocompetent patients, adverse events have been mild and infrequent; the most common events reported with either drug were nausea, headache, and diarrhea.221,222,277,280 In patients treated with valacyclovir or acyclovir for HZO, the most frequent adverse events were vomiting (5% and 3%, respectively) and facial edema (2% and 5%, respectively).221 High doses of valacyclovir have been associated with hallucinations, confusion, gastrointestinal complaints, and nephrotoxicity (especially in severely ill HIV-infected patients).277,281,283,284,285 As with acyclovir, neurotoxicity is more likely in the presence of renal failure, reinforcing the need for dosage adjustment with renal dysfunction.286 An important caveat is that long-term (>90 days) high-dose (2 g four times daily) valacyclovir in patients with advanced AIDS was associated with the occurrence of thrombotic microangiopathy (thrombotic thrombocytopenic purpura/hemolytic uremic syndrome).285 Although this finding has not been reported in subsequent studies of patients (including HIV-infected patients) receiving lower doses (up to 1000 mg/day) for long-term-HSV suppression,287 this regimen should be avoided for extended periods in severely ill HIV-infected patients. Aseptic meningitis occurred after a single 1000-mg dose in an elderly patient.288
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


