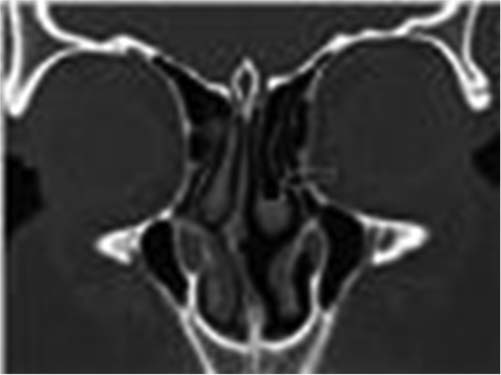
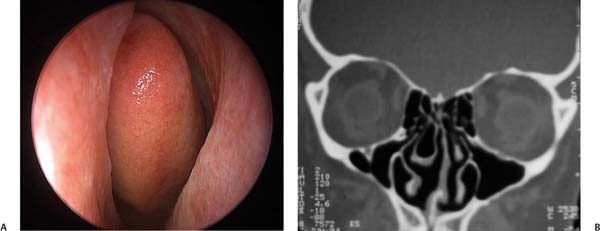
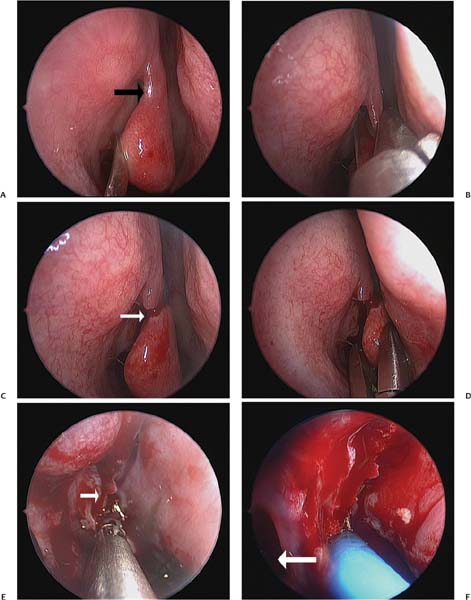
16 The View in Support of Middle Turbinate Resection As was stated in Chapter 15, the middle turbinate (MT) is an important landmark in endoscopic sinus surgery (ESS). Resection of the middle turbinate remains a source of considerable debate and controversy in the surgical management of sinonasal disease. Despite the volume of literature both supporting and disparaging the removal of the MT, there is only sparse objective evidence for either. The current rhinology literature remains inconclusive regarding the best management of the middle turbinate during sinus surgery. A great deal of controversy surrounding MT resection appears to be based on each surgeon’s personal philosophy regarding nasal physiology and anatomy. The debate obviously divides those who preserve and those who propose varying degrees of turbinate excision, from partial to neartotal removal. Historically, the practice of MT resection was condemned. Messerklinger felt that (with few exceptions) the MT should be preserved.1 Partial removal was only to be reserved in cases of concha bullosa or paradoxical MT, and resection in these instances was always conservative. Conversely, Wigand and colleagues recommended partial or total MT resection as a routine step in virtually all ESS.2 Both approaches to the middle turbinate yielded successful outcomes, thus supporting the use of either philosophy. Yet, even with the good results seen with either approach, surgeons who either routinely resect or those who routinely preserve the MT disavow the opposing method vehemently. Surgeons often cling to their respective positions on the issue quite passionately. Even in the face of such fervor, however, there are surprisingly very few studies that provide a hard scientific rationale in the approach to MT preservation or resection. In fact, virtually all of the literature that exists on the subject of MT resection is based on nonrandomized, retrospective data. In 2001, Clement and White3 reviewed over 500 articles describing turbinate surgery over a period of 35 years and not one randomized controlled study was identified. Their conclusion is essentially the overarching theme regarding MT resection: there really is no conclusive evidence supporting or discrediting the procedure. For every study that appears to favor one approach, there are others that endorse the opposing view; thus management is largely based on personal surgical belief or anecdotal experience. In the following section, we will review the relevant middle turbinate anatomy. The rational for its resection in sinus surgery will be discussed including some of the controversies and theoretical problems associated with removal of the middle turbinate, specifically addressing the validity or actual occurrence of complications of removal of the turbinate. The MT is embryologically derived from the ethmoid bone. Structurally, the MT can be divided into three segments.4 The anterior third attaches superiorly and vertically to the skull base at the horizontal plate of the ethmoid bone just lateral to the cribriform plate (Fig. 16.1). This attachment may be pneumatized in up to 12% of the population,5 thus forming an aerated vertical segment of the MT, which may be referred to as the interlamellar cell (Fig. 16.2). This aerated segment is subject to the same inflammatory and infectious processes as other sinonasal mucosa, thereby resulting in obstruction of drainage from the ethmoid infundibulum. The middle segment of the MT, the ground or basal lamella, inserts laterally, attaching it to the lamina papyracea. This attachment divides the ethmoid sinus into anterior and posterior compartments. The posterior segment of the MT is attached inferiorly and oriented horizontally, inserting onto the perpendicular process of the palatine bone anterior to the sphenopalatine foramen.4 The anterior-superior portion of the MT, an important surgical landmark, forms the medial boundary of the frontal recess. Therefore, lateralization of the MT can lead to structural narrowing of the frontal sinus outflow tract and frontal sinusitis.6 Also to be considered is the variability in the shape of the MT wherein there may be paradoxical curvature or pneumatization. Pneumatization of the head of the middle turbinate, or concha bullosa, is also a variation of special consideration in patients where this may cause nasal obstruction or obstruction of the ostiomeatal unit (Fig. 16.3). Fig. 16.1 The lateral nasal wall, showing the anatomy of the middle turbinate and surrounding structures. (From Levine HL, Clemente MP. Sinus Surgery: Endoscopic and Microscopic Approaches. New York: Thieme Medical Publishing; 2005:15. Reprinted with permission.) Fig. 16.2 Pneumatization of the vertical attachment of the middle turbinate or interlamellar cell. Fig. 16.3 (A,B) Concha bullosa. (A) Endoscopic view of a large right concha bullosa cell with partial occlusion of the nasal airway. (B) Computed tomography (CT) scan of right concha bullosa cell. The middle turbinate debate is largely centered on one crucial question: how much middle turbinate can one safely resect? The effect of MT resection on normal sinus and nasal physiology remains uncertain. The nasal turbinates are thought to function collectively to direct and assist in lamination of nasal airflow, humidify and warm inspired air, and provide a mechanical defense against particulate matter. As compared with the inferior turbinate, the MT is significantly smaller, contains less vascular and erectile tissue, accounts for a negligible portion of nasal airway resistance, and is believed to have less functional significance. Despite this evidence, as well as literature supporting the safety of middle turbinectomy, the procedure continues to provoke a considerable amount of controversy, particularly regarding lateralization of the turbinate remnant as a factor promoting postoperative frontal sinusitis. Other concerns include loss of a significant surgical landmark, development of atrophic rhinitis, postoperative hemorrhage and anosmia. The controversy surrounding MT resection appears to be based on personal philosophy regarding nasal physiology and anatomy. There are currently several indications for the removal of the MT in ESS that are more generally accepted. Some cited indications for middle turbinate resection include treatment of concha bullosa that participate in nasal obstruction and/or prevent access to the middle meatus in the “crowded nose,”6 removal of disease involving the turbinate,7 surgical access to the paranasal sinuses, and treatment of headache related to the middle turbinate syndrome where contact between an enlarged MT and either the septum or lateral nasal wall leads to stimulation of the sensory portion of the trigeminal nerve.8 The techniques for MT resection are also varied. Kennedy and Sinreich9 describe a technique where the turbinate is split in the middle and only the lateral portion is removed, leaving the medial portion intact to function physiologically. Wigand describes resecting the posterior third of the middle turbinate when performing any retrograde sphenoethmoidectomy.10 Morgenstein and Krieger describe a technique that involves cutting the superior attachment of the MT then snaring the anterior two-thirds.11 Freedman and Kern describe resection of the middle turbinate to within 0.5 cm of the skull base as an integral part of all headlight intranasal sphenoethmoidectomies.7 In the majority of patients, this maneuver addresses disease involving the turbinate (e.g., polyposis or osteitis); turbinate resection is advocated regardless of the amount of pathology involving the middle turbinate. The technique of MT resection employed by the senior author is depicted in Fig. 16.4, as a modification of the techniques described by Wigand (see Video 16.1). It is performed with the use of a zero-degree 4-mm telescope. Initially, the middle turbinate is fractured medially toward the septum using a Freer elevator to expose its vertical, superior attachment (Fig. 16.4A). This attachment is incised with a straight turbinate scissor at its most anterior portion (Figs. 16.4B,C). The body of the turbinate is then grasped with straight Wilde forceps and pulled inferiorly and posteriorly, leaving at least 0.5 cm of the superior attachment and basal lamella to preserve as landmarks (Figs. 16.4D,E). The most posterior attachment of the MT is then incised using through-biting forceps thereby completing the partial resection. The remainder of the posterior attachment is then suction cauterized to coagulate small branches of the sphenopalatine artery, as prophylaxis against intraoperative or postoperative hemorrhage (Fig. 16.4F). Fig. 16.4 (A–F) Technique of endoscopic right partial middle turbinectomy. (A) Middle turbinate being medially fractured to expose its vertical attachment (black arrow) superiorly. (B) Vertical attachment incised with straight turbinate scissors at its most anterior part. (C) After this incision of the anterior, superior attachment (white arrow). (D) The head of the turbinate is grasped and dissected inferiorly and posteriorly along the length of the turbinate back to the basal lamella. (E) Incision of the posterior turbinate attachment completes the partial resection. White arrow indicates remnants of the superior and basal lamella attachments being preserved as a landmark. (F) Suction cautery applied to the posterior attachment remnant to coagulate small branches of sphenopalatine artery. White arrow indicates maxillary sinus ostium. Historically, the practice of MT resection has been condemned, largely due to theoretical and actual observed complications following removal. The most prominent of these concerns and complications include alteration in nasal function including air humidification, filtration, and airflow;6 increased incidence of frontal sinusitis;6 ethmoid scarring;12 development of anosmia;13 postoperative epistaxis;14 loss of anatomic landmark for revision surgery;6 and the development of atrophic rhinitis.10 If the turbinates play a role in the lamination of nasal airflow, it is quite possible that their removal may contribute to postoperative changes in nasal airflow resistance. Is there evidence of such an effect? Recently, Brescia et al14 sought to define the effect of MT resection on nasal airflow. In this retrospective study, 23 patients with extensive sinonasal polyposis who had undergone partial resection of the middle turbinate ESS were compared with 25 polyp patients who had ESS with MT preservation. The outcomes examined included endoscopic scoring of polyposis and measurement of nasal airway resistance by computerized rhinomanometry performed at 3 months and 12 months after surgery. The findings of this study were improvement of endoscopic score and a statistically significant reduction of nasal airway resistance after both surgical techniques, with no statistically significant difference in the mean nasal airway resistance values before and after when comparing MT resection versus preservation. Previously, prospective evaluation of the effect of MT resection on nasal airflow was performed by Cook et al.15 They evaluated 31 consecutive patients who underwent ESS with partial middle turbinectomy performed as part of their surgery. They measured pre- and postoperative nasal airflow and nasal airway resistance using computerized rhinomanometry and found that all patients had significant improvement in nasal airflow (p < 0.001) and significant decrease in nasal resistance (p < 0.001) compared with preoperative measures. Obviously this study lacks a control group of patients who did not have turbinates removed; thus, the data should be considered with this in mind. It has been shown that olfactory neuroepithelium exists within the superior portions of the middle turbinate. In the late 1890s and early 1900s, both von Brunn16 and Read17 independently performed histologic evaluations in animals and humans and used their findings to develop schemata demonstrating the distribution of the olfactory neuroepithelium. According to these schemata, there is olfactory neuroepithelium localized to a small portion of the superior parts of the middle turbinate. However, this is a relatively small amount of olfactory tissue compared with the entire distribution of surface area available for olfaction, thus one could conclude that MT resection should not significantly affect olfaction. However, in combination with age-related decrease in olfactory neuroepithelium, there may be a perceptible difference in older patients after MT resection or as younger patients get older. Clinically, this has not been the case. Beidlingmanger13 reviewed the records of 110 patients undergoing 198 partial middle turbinate resections during endoscopic sinus surgery. The patients were evaluated for the complications of anosmia, bleeding, and crusting. Patients undergoing endoscopic sinus surgery with partial middle turbinate resections were evaluated by histopathologic and computed tomography (CT) analyses. In this review of 110 patients with 198 partial turbinate resections, there was only one patient who complained of anosmia. Also of note in this study, one patient required vessel ligation for bleeding, and no patients had excessive crusting. This 0.9% incidence of anosmia is comparable to the 0.8% incidence in Wigand’s series of 220 patients who underwent ESS with turbinate preservation. Similarly, in two other large series of over 1000 patients each, Lawson18 and Freedman and Kern7 found no increased risk of anosmia or atrophic rhinitis in patients who underwent MT resections. Similarly, Toffel, who reported a large series of patients over 16 years who underwent partial middle turbinectomy, emphasizes the importance of preserving the superior rim of turbinate in which olfactory epithelium may reside to minimize the possibility of postoperative olfactory disturbance.19 Postoperative scarring can be a source of great disappointment after ESS. The incidence of scarring for all undergoing ESS ranges from 4 to 27% in the literature,12 which may lead to recurrent symptoms and the need for further surgery. Reports of MT resection leading to lateral scarring of the MT to the nasal wall have been described. Scarring of frontal sinus outflow secondary to middle turbinate resection is also an outcome that has been discussed in the literature. This scarring is thought to be related to the healing process after middle turbinectomy.6 The proposed mechanism is that a middle turbinate cut near its anterior superior attachment becomes destabilized, and the lateral aspect of the MT remnant adheres to the surgical field. Granulation tissue in the ethmoid cavity gives way to scar and gradual traction on the turbinate remnant drawing it across the area of the frontal recess. The ensuing inadequate drainage and ventilation of the frontal sinus leads to sinusitis. There is data both supporting and disproving that MT resection can cause frontal sinusitis in this manner. In 1995, Swanson et al6 performed a retrospective review to determine if MT resection affected postoperative frontal sinus disease. They identified 110 consecutive patients with chronic or recurrent acute sinusitis, 69 of whom had previous middle turbinectomy and 41 patients with intact MTs after prior sinus surgery. In 42 patients, CT scans were scored and defined as having mild to moderate or severe disease. Frontal sinusitis seen on CT scan was present in 30 of 40 (75%) patients who had MT resection versus 9 of 20 (45%) patients who did not, and this difference was statistically significant (p < 0.05). They also considered the degree of MT resection in this study by using CT scans to determine the height of MT resection in the frontal recess area and found no statistical difference between patients with high and low resection. The authors discussed several potential weaknesses of their study, including its retrospective nature, the lack of information on preoperative sinus disease, and the lack of standardization of operative indications or technique. Scar formation and maxillary antrostomy patency were not addressed in this study. Conversely, in 1998, Fortune and Duncavage20 retrospectively reviewed 155 consecutive patients undergoing partial MT resection for either sinusitis or nasal obstruction. Their findings revealed a 10% rate of frontal sinusitis after partial middle turbinectomy and found that the development of sinusitis in these patients was largely associated with preoperative comorbidities such as asthma, nasal polyps, and severe disease on CT or diseased middle turbinates. In some instances, preservation of the MT can be a contributing factor to failure after ESS. Some propose that the MT may play a role in the pathogenesis of inflammatory nasosinusal disease secreting vasoactive sensory neuropeptides.21 More likely, however the preserved MT may often be destabilized by its pathology or by inherent anatomic abnormalities like paradoxical curvature. In such instances, lateral scarring of the turbinate can lead to further obstruction of maxillary sinus drainage despite our most earnest surgical attempts to improve it. There is evidence to support a potentially higher rate of postoperative synechiae with MT preservation versus resection.22 Examples of such scarring can be seen in Fig. 16.5. Additionally, visualization of the sphenoethmoidal region is aided by its absence allowing for the detection of scarring in this area, which may be easily addressed with office-based manipulation thus avoiding the need for revision surgery. It is our practice to facilitate postoperative management by regular examinations of the sinus openings for early indications of scar formation. With the access afforded by partial MT resection, both visualization and manipulation of these openings are possible in the office using topical anesthesia. Fig. 16.5 (A,B) Postoperatively, unresected middle turbinates have scarred laterally to cause maxillary outflow obstruction. In both cases, previous ethmoidectomy and maxillary antrostomies were performed. The role of middle turbinate resection in endoscopic sinus surgery, despite the myriad of studies and articles on the subject, remains uncertain. The degree to which MT resection may have deleterious effects on nasal airflow, postoperative scarring and future surgery, with the loss of surgical landmarks is emphasized in some studies and refuted in others. The one prevailing theme of these studies is that none meets the standard of prospective randomized controlled evidence from which one may extrapolate a conclusion about which approach is best. Thus, all we are left with are the studies of those in whose hands both methods seem to work quite well. There are some points that must be kept in mind when approaching the turbinates, regardless of which side of the fence one favors. Complete removal of the middle turbinate including its most superior attachment is neither recommended nor necessary in the absence of malignancy or other invasive disease. The most superior attachment, if left in place may serve as a landmark and may contain olfactory neuroepithelium whose preservation would prevent theoretical diminution in olfaction, either immediately or long-term. Care should be taken to address the possibility for hemorrhage from the posterior turbinate attachment. In the hands of those familiar with their respective techniques, both yield successful outcomes. • Despite the volume of literature both supporting and disparaging the removal of the MT, there still is sparse objective evidence for either. The current rhinology literature remains unclear regarding the best management of the middle turbinate during sinus surgery. • The effect of middle turbinate resection on normal sinus and nasal physiology remains uncertain. Although the role of the inferior turbinates in nasal airflow has been demonstrated, the middle turbinate, which contains less vascular and erectile tissue, accounts for a negligible portion of nasal airway resistance, and is believed to have less functional significance. • There are currently several indications for the removal of the middle turbinates in endoscopic sinus surgery that are generally accepted. These include concha bullosa that participate in nasal obstruction and/or prevent access to the middle meatus, removal of disease involving the turbinate, and treatment of headache related to the middle turbinate syndrome where contact between an enlarged MT and either the septum or lateral nasal wall leads to stimulation of the sensory portion of the trigeminal nerve. • Techniques for MT resection are varied and include removal of only the lateral portion, resection of the posterior third, and resection along the length of the turbinate to within 0.5 cm of the skull base. • Proposed problems associated with MT resection include alteration in nasal function, increased incidence of frontal sinusitis secondary to scarring, development of anosmia, bleeding, loss of an anatomic landmark for revision surgery, and the development of atrophic rhinitis. • Complete removal of the middle turbinate including its most superior attachment is neither recommended nor necessary in the absence of malignancy or other invasive disease. The most superior attachment, if left in place, may serve as a landmark and may contain olfactory neuroepithelium whose preservation would prevent theoretical diminution in olfaction, either immediately or long-term.
 Anatomy of the Middle Turbinate
Anatomy of the Middle Turbinate
 The Resection versus Preservation Debate
The Resection versus Preservation Debate
 Middle Turbinate Resection Techniques
Middle Turbinate Resection Techniques
 Concerns about Middle Turbinate Resection
Concerns about Middle Turbinate Resection
Alteration in Nasal Function
Anosmia
Scarring and Frontal Sinusitis
 Why Not Preservation?
Why Not Preservation?

 Conclusion
Conclusion
The View in Support of Middle Turbinate Resection

Pearls
< div class='tao-gold-member'>Only gold members can continue reading. Log In or Register to continue

Full access? Get Clinical Tree


