2 The presence of significant bleeding in the surgical field is a critical factor in the potential success or failure of endoscopic sinus surgery (ESS).1–4 When significant bleeding is present, recognition of anatomical landmarks becomes difficult.2–4 Bleeding obscures surgical planes and makes the identification of the drainage pathways of the sinuses difficult. Cell walls become difficult to distinguish from the lamina papyracea or skull base and the risk of causing complications increases.3,4 If the patient has significant inflammation of the sinuses, from chronic infection or the presence of pus/fungal debris, increased vascularity will often contribute to more bleeding.2,5 If the surgeon attempts to manipulate an instrument in the surgical field after the discernible anatomy is covered in blood, the risk of a complication increases. In addition, greater surgical trauma may occur, cells may be left behind and there is an increased likelihood of postoperative scarring and failure of the surgical procedure. It is therefore critical to optimize the surgical field and, in so doing, make the surgical dissection as easy as possible.2–4 Our department has a special interest in this aspect of ESS and has conducted several double blind randomized controlled studies in an attempt to establish which maneuvers to reduce bleeding are worthwhile. To date not all maneuvers have been scientifically evaluated but where there is evidence for a specific maneuver this will be presented. The first important issue to address is a grading system for bleeding in the surgical field. Boezaart and van der Merwe described and validated a grading system of five grades presented in Table 2.1.3 Although this grading system is valuable we have found that the majority of surgical fields are around grade 3 with some grade 2 and some grade 4.2 Only on rare occasions are grade 1 and 5 fields encountered. This tends to compress the grading system and makes differentiation of more subtle changes difficult. Grade 3 may need to be further divided to allow variation within grade 3 to be discerned.2 We have recently developed and validated an endoscopic sinus surgical field score which separates the middle grades and allows more accurate grading of the surgical field (Table 2.2). Local anesthetic has the advantage of not inducing generalized vasodilation. Increased circulating catecholamines may also improve the surgical field by continuing to act on the prearteriolar and precapillary sphincters. However, there are several limitations to local anesthetics. In our department local anesthetic is offered to patients having limited ESS confined to the middle meatus. We prefer general anesthesia for ESS that involves the frontal recess and/or posterior ethmoids and/or sphenoids. It is our current practice to use laryngeal masks rather than endotracheal intubation for all our patients undergoing sinus surgery. The rationale for this is that it allows the patient to be kept under a lighter general anesthetic with less vasodilation and less intraoperative bleeding. In addition, the patient does not cough and strain on the endotracheal tube as they recover from the anesthetic thus avoiding the venous congestion and subsequent hemorrhage often associated with such straining. One of the potential downsides of a laryngeal mask is the possibility of contamination of the upper airway by blood. This is prevented by the placement of a small throat pack above the laryngeal mask in the back of the throat to catch any blood from the nasal cavity. Another possible downside is the potential difficulty with ventilation of the patient during surgery. Our standard protocol is total intravenous anesthesia (TIVA) with a laryngeal mask in a nonparalyzed patient. The remifentanil infusion (part of TIVA) suppresses spontaneous ventilation and allows the patients to be ventilated through the laryngeal mask. The lack of paralysis provides additional safety against intraoperative awareness because the patient should move if the level of anesthesia becomes too light. Table 2.1 Boezaart and van der Merwe Grading System for Bleeding During Endoscopic Sinus Surgery
The Surgical Field in Endoscopic
Sinus Surgery
 Local versus General Anesthetic
Local versus General Anesthetic
 Patient anxiety and sudden patient movement during delicate surgery can be problematic.
Patient anxiety and sudden patient movement during delicate surgery can be problematic.
 Surgery takes between 1 and 2 hours. Some patients (especially older patients) have difficulty remaining still for this length of time.
Surgery takes between 1 and 2 hours. Some patients (especially older patients) have difficulty remaining still for this length of time.
 Appropriate anesthesia needs to be achieved in all the sinuses and the nasal cavity.
Appropriate anesthesia needs to be achieved in all the sinuses and the nasal cavity.
 If the procedure is bloody the patient may have difficulty dealing with the volume of blood trickling into the pharynx. If the patient is sedated aspiration can occur.
If the procedure is bloody the patient may have difficulty dealing with the volume of blood trickling into the pharynx. If the patient is sedated aspiration can occur.
 Water from the scope scrubber may add to the secretions in the pharynx that the patient needs to deal with.
Water from the scope scrubber may add to the secretions in the pharynx that the patient needs to deal with.
 Teaching of residents can be more difficult when the patient is awake.
Teaching of residents can be more difficult when the patient is awake.
 Standard Nasal Preparation for Endoscopic Sinus Surgery
Standard Nasal Preparation for Endoscopic Sinus Surgery
Laryngeal Mask versus Endotracheal Intubation
Grades | Surgical Field |
Grade 1 | Cadaveric conditions with minimal suction required |
Grade 2 | Minimal bleeding with infrequent suction required |
Grade 3 | Brisk bleeding with frequent suction required |
Grade 4 | Bleeding covers surgical field after removal of suction before surgical instrument can perform maneuver |
Grade 5 | Uncontrolled bleeding; bleeding out of nostril on removal of suction |
Source: Data from Boezaart AP, van der Merwe J, Coetzee A. Comparison of sodium nitroprusside- and esmolol-induced controlled hypotension for functional endoscopic sinus surgery. Can J Anaesth 1995;42:373–376.
Table 2.2 The Wormald Grading System for Bleeding During Endoscopic Sinus Surgery*
Grade | Surgical Field |
0 | No bleeding |
1 | 1–2 points of ooze (no blood in the sphenoid) |
2 | 3–4 points of ooze (no blood in the sphenoid) |
3 | 5–6 points of ooze (slight blood accumulation in the sphenoid) |
4 | 7–8 points of ooze (moderate blood accumulation of sphenoid; fills after 90 seconds) |
5 | 9–10 points of ooze (sphenoid fills after 60 seconds) |
6 | > 10 points of ooze, obscuring surface (sphenoid fills between 40 and 60 seconds) |
7 | Mild bleeding/oozing from entire surgical surface with slow accumulation of blood in postnasal space (sphenoid fills by 40 seconds) |
8 | Moderate bleeding from entire surgical surface with moderate accumulation of blood in postnasal space (sphenoid fills by 30 seconds) |
9 | Moderately severe bleeding with rapid accumulation of blood in postnasal space (sphenoid fills by 20 seconds) |
10 | Severe bleeding with nasal cavity filling rapidly (sphenoid fills in < 10 seconds) |
*Used when all sinuses have been opened.
Positioning the Patient
The positioning of the patient is described in Chapter 1. It is important to have the patient 30 to 40 degrees head up so that the venous return from the head and neck is facilitated. This puts the patient’s head above the chest, which lowers the arterial pressure and prevents venous congestion, and thereby improves the surgical field.6
Topical Vasoconstriction
In a study recently published we showed that any packing material placed in the nasal cavity tends to cause damage to the nasal mucosa.7 The more abrasive the packing, the worse the trauma.6 Taking this into consideration, the least abrasive packing material is used, namely the neurosurgical Cottonoid patties (Codman, Raynham, MA). The anesthetist is consulted to ensure there is no contraindication to the use of cocaine. If there is a concern then 1% oxymetazoline is used in place of cocaine. In an adult patient a mixture of 2 mL of 10% cocaine, 1 mL of 1:1000 adrenaline, and 4 mL of saline is divided into two equal portions, with one portion used to soak six neuropatties. These six neuropatties are placed in the nose once the patient is anesthetized. The other half of the cocaine mixture and remaining four neuropatties are kept sterile on the instrument trolley for later use during surgery if required. Three neuropatties are placed on each side directly after intubation using a Freer elevator to manipulate them gently into place. The first neuropattie is placed in the sphenoethmoidal recess, the second under the middle turbinate, with the third being placed over the axilla of the middle turbinate (Fig. 2.1). If there is a concha bullosa or significantly lateralized middle turbinate, the neuropattie is placed along the inferior margin of the middle turbinate. No force is used to place the neuropatties in the middle meatus.

Fig. 2.1 Placement of the neuropatties in the left nasal cavity prior to surgery. A pattie is in the sphenoethmoidal recess (1), another is in the middle meatus (2), and another is in the region of the axillary flap (3).
Local Infiltration
A 2% solution of lidocaine (“lignocaine” in the UK and Australia) with either 1:80 000 or 1:100 000 adrenaline is administered with a dental syringe and needle. The injections are given after the patient has been draped and the camera and endoscope are available. Under endoscopic guidance the area above the middle turbinate is infiltrated. This is followed by infiltration into the anterior end of the middle turbinate. Note that the area anterior to the uncinate is not infiltrated as bleeding from an injection site can obscure the uncinate during its removal. In some patients, where there is expected increased likelihood of bleeding, a third injection is given into the back end of the middle turbinate in the region of the sphenopalatine artery. A spinal needle is used as the dental needle is usually not long enough to reach this area. Figure 2.2 illustrates the routine infiltration points used.
Preoperative Antibiotics and Steroids
Inflammation increases the vascularity of tissues and, when surgery is conducted on highly inflamed tissues, increased bleeding results. Patients with acute sinusitis, who have an infective complication requiring surgery, will often have a very bloody surgical field. It therefore stands to reason that using antibiotics in patients with a significant infection preoperatively should improve the surgical field. However, most of our patients undergoing ESS have had extended medical therapy which normally includes numerous courses of antibiotics and often systemic steroids, and therefore rarely have an acute infection present. The value of using antibiotics preoperatively in this elective patient group is unknown as there are no well-designed studies addressing this issue. The important questions that remain unanswered are the type of antibiotic, the length of time it should be used before surgery, and the patient group most likely to benefit from preoperative use. Currently I do not routinely place patients on antibiotics preoperatively.
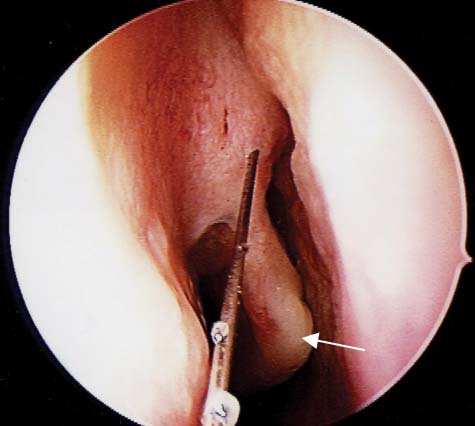
Fig. 2.2 Injection sites in the right nasal cavity for local anesthetic prior to endoscopic sinus surgery. The needle is in the region of the axillary flap and the white arrow indicates the injection site on the anterior end of the middle turbinate.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


