CHAPTER 47 The Pathogenesis of Rhinosinusitis
Definitions of Acute and Chronic Rhinosinusitis
In order to understand the pathogenesis and pathophysiology of rhinosinusitis one must realize that there are different forms of rhinosinusitis with dramatically different inciting mechanisms. Although sinusitis is commonly used for any inflammation or infection of sinuses, this term has largely been replaced by rhinosinusitis because the nose is almost always involved with the infection or inflammation at the same time as the sinuses.1 Many potential factors can result in the development of rhinosinusitis, so there has been some debate concerning the exact definitions.
More recently, rhinosinusitis has been defined as “a group of disorders characterized by inflammation of the mucosa of the paranasal sinuses.”2 In 1997 the Rhinosinusitis Task Force of the American Academy of Otolaryngology–Head and Neck Surgery3 developed a now well-accepted classification of rhinosinusitis, which was reported by Lanza and Kennedy.1 This classification relies on two major criteria that help to identify whether or not a patient has rhinosinusitis primarily on the basis of symptoms (Box 47-1) and then to classify rhinosinusitis types based primarily on temporal time frames from the onset of symptoms. The symptoms are divided into major and minor categories, with purulent nasal drainage, nasal congestion, facial pressure or pain, decreased smell, and posterior purulent drainage serving as the major symptoms.1
An inflammatory response is an expected sequela of an infectious process. Inflammation in the nose and sinuses from a variety of causes can result in sinus ostia obstruction and can predispose to the development of an infection. Many factors have been described as playing a role in the development of acute bacterial rhinosinusitis (ABRS).1,4,5 These include the following factors related to the host: genetic factors such as immotile cilia syndrome and cystic fibrosis; anatomic variants such as a concha bullosa, septal spur, and paradoxical turbinate; certain systemic diseases or medical treatments that predispose individuals to infections; neoplasms; and allergic or immune disorders. Rhinosinusitis may also develop in relationship to environmental factors, as follows: bacterial, viral, or fungal infections, or inflammation that occurs secondary to fungal or bacterial colonization2,6; trauma; primary or secondary tobacco smoke exposure7 and chronic or acute irritants or noxious chemicals; and iatrogenic factors, including surgery, medications, nasal packing, and nasogastric tube placement.8 There is growing evidence that individuals with allergies have a higher incidence of both acute and chronic rhinosinusitis, and an association of acute bacterial rhinosinusitis with asthma has also been suggested, although this may also relate to the presence of allergic rhinitis.9–11
Acute Rhinosinusitis
Acute rhinosinusitis is a very common disorder that at one time or another affects most people. From a temporal standpoint acute rhinosinusitis lasts for up to 4 weeks.1 The disorder is almost always due to an infectious process, principally from viruses and bacteria, with viruses accounting for the majority of the cases. There have been attempts at estimating the prevalence of acute rhinosinusitis. It is estimated that children have between six to eight upper respiratory (tract) infections (URIs) per year and that adults average two or three.12 If an assumption is made that 90% of patients with colds have sinusitis (bacterial or viral) and that each person has an average of four URIs per year, then it can be estimated that in the United States there are more than a billion cases of viral and bacterial rhinosinusitis annually (260 million people × 4 episodes = 1.040 billion cases).13
Acute bacterial rhinosinusitis has been defined as sudden in onset and with duration of less than 4 weeks.1 Because most cases of rhinosinusitis are caused by a self-limited viral infection and bacterial infections usually occur after a viral URI, ABRS has been diagnosed after at least 7 to 10 days of symptoms or in patients whose symptoms are worsening after 5 to 7 days.1,4,14 This distinction has been endorsed in most of the guideline development for the treatment of ABRS.4 The diagnosis may be more difficult in children, because they often have difficulty describing their symptoms.
Streptococcus pneumoniae (20%-45%) and Haemophilus influenzae (22%-35%) are the predominant organisms in ABRS in adults, whereas S. pneumoniae (30%-43%), H. influenzae (20%-28%), and Moraxella catarrhalis (20%-28%) are the predominant organisms in ABRS in children.4,14 Although Staphylococcus aureus was previously thought to be a contaminant, a 2007 meta-analysis has confirmed that this organism should now be considered a real pathogen in ABRS, accounting for 8% to 10% of adult cases (Fig. 47-1).15 Because M. catarrhalis infection is largely a self-limited disease, and methicillin-resistant S. aureus (MRSA) is becoming a bigger health care issue, S. aureus may be more important to treat. S. aureus is also well recognized in both CRS and AECRS.14–16
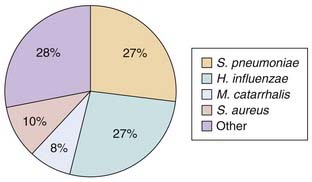
Figure 47-1. Pathogen distribution in acute bacterial rhinosinusitis (ABRS) as shown by a recent meta-analysis.
(From Payne SC, Benninger MS. Staphylococcus aureus is a major pathogen in acute bacterial rhinosinusitis: a meta-analysis. Clin Infect Dis. 2007;45:e121-e127.)
ABRS is a self-limited disease in many cases. Evaluation of placebo-controlled antibiotic trials has shown that there is a high self-resolution rate.4,13,14 Infections with M. catarrhalis are most likely to resolve without antibiotic treatment, those with H. influenzae less likely, and those with S. pneumoniae least likely to resolve without treatment. It may become important therefore to determine which patients have which organism. The most reliable way is to obtain a culture, with a maxillary sinus tap being the traditional method of obtaining sinusitis cultures. The invasiveness of this test and the advancement of endoscopically guided selective middle meatal culture collections have resulted in a shift to this latter method in clinical practice.16,17 An evidence-based review has shown that cultures of endoscopic middle meatal specimens are as sensitive and specific as those of maxillary sinus tap specimens.17 In clinical practice, however, cultures are rarely performed unless there has been a failure of treatment. The severity of the symptoms and radiographic findings may help identify different pathogens, in that patients infected with S. pneumoniae have been found to have more significant symptoms and worse radiographic findings than those infected with H. influenzae.18
With the widespread utilization of pneumococcal 7-valent conjugate vaccination, there has appeared to be a shift in the overall distribution of pathogens in ABRS. In a 2006 study assessing the pathogenesis of ABRS, the proportions of the recovery of pathogens from cultures of endoscopically obtained specimens in adults with acute maxillary sinusitis were compared for the periods 4 years prior to and 5 years after the introduction of the conjugate pneumococcal vaccine. Recovery rate for H. influenzae increased from 36% to 43%, making it the most common pathogen. At the same time, the rate for S. pneumoniae was found to decrease from 46% of isolates to 35%. There also were increases in the proportions of cases caused by M. catarrhalis and S. aureus.19 In a similar study, nasopharyngeal cultures were obtained in children with acute maxillary sinusitis before and after the widespread use of pneumococcal conjugate vaccination. S. pneumoniae decreased from accounting for 43% to 25% of isolates, whereas H. influenzae increased from 35% to 41%. The rate for M. catarrhalis remained stable, changing from 13% to 14%. The rate for Streptococcus pyogenes increased from 7% to 12%, and that for S. aureus from 4% to 8%.20
With the widespread use of pneumococcal vaccination a change also seems to have occurred in the serotypes of S. pneumoniae responsible for not only ABRS but also acute otitis media (AOM), with an increase in serotypes not found in the vaccine.21–23 There has been some speculation that this serotype replacement may reduce the long-term efficacy of the pneumococcal 7-valent conjugate vaccine.23 Multiple studies have shown a reduction in culture rates for both the nonsusceptible and highly resistant strains of S. pneumoniae in AOM and to a lesser extent in ABRS.24–28 Whitney and colleagues25 showed a drop of 35% in rate of strains not susceptible to penicillin.25 High-level resistance of S. pneumoniae to penicillin also appears to have dropped, from 15% to 5% in one report.27 There has been an associated increase in the β-lactamase–producing strains of H. influenzae.28 Although the data related to the shift in pathogens is less well supported in ABRS than in AOM, there have been clear and parallel shifts in the pathogens associated with ABRS and AOM. This finding is not unexpected because the pathogenic organisms are similar for ABRS and AOM and the shift in the microbiology of ABRS has been suggested to have occurred because of the involvement of the same pathogens in AOM and ABRS.29
The mechanism by which the viral inflammation of a viral URI can lead to ABRS has been suggested in a number of reports.5,30 As previously mentioned, acute rhinosinusitis typically develops in conjunction with an acute viral URI. The propensity for development of a viral URI may occur more commonly in predisposed individuals. The viral infection can result in swelling of the mucosa of the nose or sinuses, and the resultant swelling can produce occlusion or obstruction of the sinus ostia. A reduction in oxygen tension occurs that in turn can reduce mucociliary transport and transudation of fluid into the sinuses.5 The inflammation also results in changes in the mucus, which becomes more viscous, and often in alterations in cilia beat frequency. These changes in the nasal-sinus environment lead to reduced clearance, stasis of mucus, and bacterial colonization. If the sinuses remain obstructed or the mucociliary transport system does not return to normal, a bacterial infection can ensue. The ability of the body to respond to the viral challenge and reduce the inflammation may, in part, determine whether a secondary bacterial infection occurs.
The role of allergies in the development of rhinosinusitis has been strongly suggested but not proven.9–11 Antigen-antibody reactions result in the release of histamine and other mediators of inflammation. These mediators cause changes in vascular permeability, destabilization of lysosomal membranes, and other reactions that produce inflammation, mucosal swelling, and ostia obstruction.5 Although infectious agents can be primary causes of sinus inflammation, they may also represent a secondary infection. The type and magnitude of the reaction may be related to the host response and how it relates to the disease process and progression.
Recurrent acute rhinosinusitis is defined as 4 or more episodes of acute rhinosinusitis per year, with each lasting longer than 7 to 10 days, and an absence of intervening signs or symptoms that would suggest an ongoing or chronic rhinosinusitis.1 Although recurrent viral respiratory tract infections are common, in general it is rare for people to develop true recurrent episodes of ABRS to meet the preceding criteria for recurrent ABRS. When they do, it is expected that the bacteriology and pathophysiology would be similar to those of individual episodes of ABRS.
Invasive Fungal Rhinosinusitis
In a very small subset of patients with acute rhinosinusitis the inciting pathogen is neither viral nor bacterial. They have acute invasive fungal rhinosinusitis (IFRS). This disorder is almost always confined to patients with altered host defenses. A review of 43 patients with IFRS has shown that 65% were immunosuppressed because of a hematologic malignancy or its treatment. Twenty-three percent had diabetes, 7% were taking long-term steroid therapy, and 2% had acquired immunodeficiency syndrome.31 Any disorder that results in immune suppression or an immunodeficiency can lead to the development of IFRS in some individuals.
Historically the most common organism reported in IFRS has been Mucormycosis, but in the past decade, Aspergillus has become more common.31 Alternaria species and Pseudallescheria boydii have also been identified in IFRS. Aspergillus is particularly common in diabetic persons with IFRS. On examination, however, it is very difficult to distinguish between the two organisms on the basis of clinical presentation or physical examination. IFRS is suspected when the immunocompromised patient demonstrates a fever and localization of symptoms suggesting a complication of sinusitis, such as orbital swelling, change in vision, or significant facial pain. Patients may present with anesthesia of the face, mucosa, or palate and may have nasal bleeding. Nasal endoscopy may show necrosis of the nasal mucosa, or there may even be a blackish color, suggesting Mucormycosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


