CHAPTER 82 The Management of Head and Neck Melanoma and Advanced Cutaneous Malignancies
Although the overall trend in the United States demonstrates both a stabilization of cancer incidence and a decrease in cancer death rates, the incidence of cutaneous melanoma continues to rise dramatically on an annual basis.1,2 The diagnosis is growing in men faster than any other malignancy; for women, the increase in incidence is second only to that for lung cancer.3 Overall, cutaneous melanoma remains the sixth leading cause of cancer among men and the seventh cause among women. The current annual budget for melanoma treatment in the United States exceeds $740 million.4
Fortunately, the management of cutaneous melanoma is also one of fastest-evolving fields in cancer, with promising research taking place at both the molecular and clinical levels. Greater understanding of melanoma biology prompted major changes in the staging classification system set forth by the American Joint Committee on Cancer (AJCC).5 Given its association with sun exposure, melanoma is considered a preventable disease. Decreases in incidence and mortality ultimately hinge upon increases in education, prevention, and early diagnosis, as well as improved treatment for advanced disease.
Epidemiology
Despite a decline in overall cancer trends, the incidence of invasive cutaneous melanoma continues to rise dramatically, with an estimated 62,480 new cases anticipated in 2008.1 Over the past 50 years, the annual percentage change in invasive melanoma incidence has steadily increased by 4.3% each year. The lifetime risk for development of invasive melanoma has climbed at an epidemic rate, rising from 1 in 1500 individuals born in 1935 to 1 in 250 born in 1980.6 This trend is expected to continue at a startling rate, with a current estimation that 1 in 41 men and 1 in 61 women will have invasive carcinoma during their lifetimes.
Melanoma is the most lethal form of skin cancer, accounting for 8110 American deaths in 2007, 8420 deaths in 2008, and an expected 8650 deaths in 2009.1,2 These estimates average to approximately one American dying from melanoma every hour. Over the past 50 years, the annual percentage change in mortality rate has increased at a steady rate of 1.8% per year. Melanoma accounts for the second highest increase in mortality rate, especially for men older than 65 years. However, it should not be viewed as a cancer limited to the elderly because 1 in 4 patients are diagnosed before age 40, and it is the third most common cancer among women ages 20 to 39.4,6,7 Consequently, melanoma represents one of the leading cancer causes of lost potential life years, ranking second only to leukemia.
Approximately 25% of all cutaneous melanomas arise in the head and neck region,8 with more than 9000 cases diagnosed annually. The majority involve the cheek, scalp, and neck. A slight male preponderance is consistently reported,9–11 and the median age at diagnosis is 55 years.7 However, juvenile cases account for 1.66% of head and neck melanoma cases, and patients as young as 4 years are diagnosed with these lesions.12,13
Etiology and Risk Factors
Numerous environmental and genetic risk factors have been implicated in the development of cutaneous melanoma.14 They are summarized in Box 82-1.
Box 82-1 Risk Factors Associated with Cutaneous Melanoma
Adapted from Schmalbach CE, Johnson TM, Bradford CR. The management of head and neck melanoma. Curr Probl Surg. 2006;43:784.
Risk Factors
Sun exposure is considered the leading cause of melanoma.15,16 Patients who experienced peeling or blistering sunburns, even during childhood, are at particular risk.17 Associated factors include blond or red hair, green or blue eyes, and fair skin consistent with Fitzpatrick skin types I through III.18 Adults with more than 100 clinically normal-appearing nevi, children with more than 50 clinically normal-appearing nevi, and any patients with atypical or dysplastic nevi are also at risk.
A prior history of melanoma poses a greater risk; 5% to 10% of individuals diagnosed with melanoma experience a second primary melanoma.16 This increased risk remains lifelong, and the melanoma can occur anywhere on the skin. For this reason, long-term follow-up with a thorough total body examination is critical.
Genetics
A genetic component has been implicated in the pathogenesis of melanoma19; 10% to 15% of patients with melanoma report a positive family history.20 The most common chromosomal mutation associated with melanoma involves CDKN2A, which is also known as p16.21 However, the mutation accounts for only a small percentage (0.2%) of melanoma cases observed.22
B-K mole syndrome is a hereditary form of cutaneous melanoma in which members acquire large, irregular, and dysplastic nevi, often in sun-protected regions of the body, such as the scalp and trunk.23 A familial association of melanoma among individuals with atypical nevi has also been coined familial atypical multiple mole-melanoma (FAMMM) syndrome.24 Today, the term “atypical mole syndrome” is applied to familial cases of melanoma. The syndrome is inherited in an autosomally dominant fashion.25,26 The 10-year melanoma risk in this setting is reported to be 10.7%, compared with 0.62% in control patients.27,28 Fitzpatrick and Ortonne18 and Greene and associates29 approximated a 56% cumulative risk from age 20 to 59 years, which predicts that 100% of patients with atypical mole syndrome would have melanoma by age 76.
Xeroderma pigmentosa is a rare hereditary disorder also associated with melanoma; it is inherited in an autosomally recessive fashion.30 The fibroblasts in patients with this disease have a reduced or no ability to repair DNA that has been damaged by ultraviolet light.31 Consequently, multiple primary cutaneous malignancies, including melanoma, basal cell carcinoma, and squamous cell carcinoma, develop. Individuals are usually diagnosed with their first cancer prior to age 10. Unfortunately for patients with xeroderma pigmentosa, the relentless development of skin cancers—as well as other cancers—ultimately leads to death at an early age.
Congenital Nevi
Congenital melanocytic nevi (CMN) are present at birth or appear within the first 6 months of life32; an estimated 1% to 6% of children are born with CMN. The nevi are classified by size: small CMN measure less than1.5 mm in diameter and account for the majority of lesions; medium-sized CMN measure between 1.5 and 19.9 mm in diameter; and large CMN, which are also called giant congenital nevi, measure 20 mm or more. This large size can have significant cosmetic and psychosocial implications.28
Conversely, giant CMN carry an increased risk for melanoma, with an estimated 5% to 20% of patients with these lesions eventually experiencing cancer.33,34 Seventy percent of these individuals are diagnosed before age 10 years.35 Melanoma in the setting of giant CMN originates deep within the epidermis, thus potentially delaying the diagnosis and treatment.
Melanoma Classification
Several histologic subtypes of melanoma are recognized within the head and neck region. It is important to note that if data are corrected for other prognostic variables, such as tumor thickness and ulceration, melanoma subtype does not generally influence prognosis.36
Lentigo maligna (LM) represents intraepidermal or in situ melanoma. Histologically, it is often seen in the background of chronic sun damage. LM is the precursor to invasive lentigo malignant melanoma (LMM). The exact percentage of LMs that progress to invasive LMM remains unknown37; however, it is speculated that, if patients live long enough, all LMs will eventually progress to cancer. LM/LMM is most often found in the head and neck region. Traditionally, the subtype has been associated with older individuals, but the frequency in younger patients is increasing. The LM/LMM pattern warrants special comment, because this subtype is characterized by asymmetric, subclinical, and often extensive involvement of margins with atypical junctional melanocytic hyperplasia. Therefore, management with adequate wide margins can be challenging from both a functional and cosmetic standpoint. Additionally, amelanotic melanoma and invasive desmoplastic melanoma (see later) often arise within LM/LMM.
Desmoplastic-Neurotropic Melanoma
Desmoplastic melanoma (DM) describes a subtype composed of spindle cells, abundant collagen, and features resembling fibromas.38 Some lesions demonstrate a propensity for perineural and endoneural infiltration, which prompted further subclassification of a desmoplastic neurotropic melanoma (DNM) variant.39
DM/DNM subtypes are rare, accounting for approximately 1% of all cutaneous melanomas.40 However, up to 75% of the lesions manifest in the head and neck region, often in the setting of LM/LMM. The clinical presentation and biologic behavior of these tumors are distinct from those of other cutaneous melanomas. Although amelanotic cases account for only 4% to 5% of cutaneous melanomas, up to 73% of DM/DNMs are amelanotic.40,41 As demonstrated in Figure 82-1, the neoplasms often lack the typical ABCD criteria for melanoma (described later), and they can have a difficult histologic pattern that requires interpretation by an experienced pathologist. Overall, the atypical and challenging appearance of DM/DNM is thought to result in a delay in diagnosis. This fact provides one explanation for the reason that patients with DM/DNM present with thicker, more aggressive tumors.

DM/DNM is known to be locally aggressive and highly infiltrative, often leading to cranial nerve and skull base involvement. Local recurrence has been reported in up to 50% of cases.40 Explanations for this high rate include the association with neurotropism and the failure to recognize and adequately clear peripheral atypical junctional melanocytic hyperplasia margins. Although DM/DNM demonstrates greater tumor thickness at the time of diagnosis, the 12.5% rate of regional lymph node metastasis is lower than that for other melanoma subtypes.39
Mucosal Melanoma
Mucosal melanoma is recognized as a distinct subtype from its cutaneous counterpart. The most common site for mucosal melanoma is the head and neck, with 40% to 50% of cases arising in this location.42 However, less than 2% of all head and neck melanomas are mucosal in origin. Of the 84,836 melanoma cases registered in the National Cancer Database from 1985 to 1994, only 1074 (1.3%) were of the mucosal melanoma variant.43
Although small case numbers limit research to anecdotal reports, several common trends have been noted throughout the literature. The peak age for mucosal melanoma is during the sixth to seventh decade, which is approximately 10 to 15 years later than that for cutaneous melanoma.42,44–47 A slight male preponderance has also been reported.45,47,49 Ethnic differences have been observed; approximately 8.8% of mucosal melanoma cases afflict blacks and Hispanics, a considerable percentage given that less than 3% of all other melanoma variants are diagnosed among this group.48 The relative frequency is also exceedingly high in Japan, where mucosal melanoma accounts for 7.5% of all melanoma cases.50
Within the head and neck region, the most common site of origin is the nasal cavity, where the anterior nasal septum is most often involved, followed by the inferior and middle turbinates.46,49,51,52 The second most common site is the oral cavity, where a predilection for the hard palate and maxillary alveolar gingivae has been found. A review of five major mucosal melanoma series by Batsakis and colleagues51 found laryngeal primary tumors to account for less than 4% of all cases. Within the larynx, the supraglottis was the most common site of origin.
The presenting signs and symptoms of mucosal melanoma directly correlate with the anatomic site of origin. The majority of patients with nasal cavity primary tumors present with nasal obstruction and epistaxis.49,51,52 Proptosis, diplopia, pain, and facial deformity are less common and indicate advanced disease. When present, the most common sign of an oral cavity tumor is a mass lesion.52 However, oral cavity mucosal melanoma is often asymptomatic, going undiagnosed until a neck mass develops from metastasis.44,49
Many of the prognostic markers for cutaneous melanoma do not have correlates in mucosal sites.42 Consequently, the cutaneous melanoma staging system set forth by the AJCC (see later) may be less applicable to mucosal melanoma. Most patients with mucosal melanoma present with localized disease, and in only 18.7% is regional spread detected at the time of diagnosis. The high percentage of patients with stage I disease is deceiving, because local recurrence is the major reason for treatment failure.51 Fifty percent of patients have local recurrence, usually within 9 to 12 months of diagnosis, and the overall 5-year survival rate is a dismal 10% to 20%.45–4751 Rich submucosal vasculature and lymphatics are thought to account for the aggressive behavior of mucosal melanoma.51
Unknown Primary
Approximately 2% to 8% of cases of melanoma involve unknown primary sites.43,48,53 In two thirds of the cases, the patients present with regional metastasis in the absence of an identifiable primary lesion or history of melanoma; the remaining third of unknown primary cases involve distant metastasis to sites such as the subcutaneous tissues, lung, and brain.48,53–55 Several theories have been proposed to explain melanoma of unknown primary origin. The identification of melanocytes and nevus cells within the lymph node capsule and visceral organ epithelium lends credence to the belief that unknown primary cases result from melanoma arising de novo at regional and distant sites.43,56 Another clinical scenario is that the primary melanoma lesion undergoes complete spontaneous regression.56,57
The diagnosis of melanoma of unknown origin necessitates a search for the primary site with a total body skin and mucosal evaluation. A history of a previous skin biopsy or a skin lesion that spontaneously disappeared may be helpful. All pathology slides from previously excised lesions should be re-reviewed. The metastatic workup is identical to that for known primary cases (see later). After adjustment of data for tumor stage, melanomas of unknown primary origin share an overall prognosis equivalent to their counterparts with known primary sites.43,53–55
Diagnostic Workup
History
The majority of melanoma lesions are first detected by the patient or his/her significant other.58,59 Less than one fourth of lesions are diagnosed during routine office physical examination, and these latter lesions tend to be thinner.59 Overall, 80% of newly diagnosed melanomas are limited to localized, stage I/II disease.2
The earliest signs of melanoma are a change in color, size, or shape of a lesion, and pruritus is the earliest symptom. Later signs and symptoms, which are usually associated with a more advanced lesion, include bleeding, ulceration, and tenderness. Patients should be questioned about a personal and family history of melanoma. Information about previous skin biopsies, sun exposure, history of blistering sunburns, use of tanning booths, chronic sun exposure, and occupation should be obtained. Schwartz and colleagues59 investigated characteristics of 1515 patients with melanoma and found that 81% elicited a history of at least one sunburn.
Physical Examination
All patients presenting with a suspicious lesion warrant full evaluation of the skin and nodal basins by a physician who is well versed in cutaneous cancers. Thorough evaluation is imperative because up to 8% of newly diagnosed patients have multiple primary cutaneous melanomas.16,60–62
The differential diagnosis for cutaneous melanoma is broad and includes seborrheic keratosis, hemangioma, blue nevus, Spitz nevus, pyogenic granuloma, pigmented basal cell carcinoma, and cutaneous squamous cell carcinoma. The American Cancer Society has published the ABCD checklist to educate both patients and physicians about the early detection of melanoma.63 Under these guidelines, concerning signs for melanoma are as follows:
Although the ABCD checklist is helpful for the identification of melanoma, it does not detect every case.64,65 It is important to realize that a subset of cancers (e.g., amelanotic, desmoplastic, and nodular melanoma) lack the common features of the ABCD list. In one series, 88% patients with melanoma (615 of 696) recalled change in their pigmented lesions prior to melanoma diagnosis.66 Owing to the significance of change, a proposal has been set forth to add “Evolving changes” to the traditional ABCD warning signs.63 Clinicians are hopeful that the new, more comprehensive ABCDE criteria will lead to even further detection of melanoma at an earlier stage.66 Another useful screening tool is the “ugly duckling sign,”67 whereby any pigmented lesion that appears significantly and singularly different from other surrounding lesions should be viewed with a high index of suspicion, even if the lesion lacks the traditional ABCD criteria.
Biopsy
The pathology results from this biopsy then serve as the guide for the second step, which entails wide local excision (WLE) utilizing a 0.5- to 2-cm margin of normal surrounding skin, with or without sentinel lymph node [mapping and] biopsy (SLNB). The role of SLNB ultimately depends on the final microstaging of the primary lesion and is detailed later. Although obtaining wider margins at the time of the initial biopsy seems efficient and cost effective, it is highly discouraged because clinical accuracy is uncertain and removal of significant amounts of skin surrounding the lesion may compromise the ability to accurately stage regional lymph node basins by means of lymphoscintigraphy and SLNB techniques.68 Instead, biopsy with narrow margins in a two-step fashion is advocated.
Metastatic Workup
In an attempt to standardize staging workup for melanoma, a panel of the National Comprehensive Cancer Network (NCCN) has published guidelines.69 The metastatic workup performed at our institution, which accords with these guidelines, is summarized in Table 82-1.
Table 82-1 University of Michigan Guidelines for Workup for Cutaneous Melanoma
| Stage 0 (in situ) | History; physical examination |
| Stage I (<1 mm thickness) | History; physical examination |
| Stage I to II (1-4 mm thick) | History; physical examination |
| Chest radiograph optional | |
| Serum acetate dehydrogenase measurement optional | |
| Stage III (N0; >4 mm thick) | History; physical examination |
| Chest radiograph optional | |
| Serum lactate dehydrogenase measurement optional | |
| Stage III (N+; in transit) | History; physical examination |
| Chest radiograph | |
| Serum lactate dehydrogenase measurement | |
| Other imaging studies, if clinically indicated | |
| Stage IV (distant metastasis) | History; physical examination |
| Chest radiograph | |
| Serum lactate dehydrogenase measurement | |
| Other imaging studies, per clinical trial |
Adapted from Johnson TM, Bradford CR, Gruber SB, et al. Staging work-up, sentinel node biopsy and follow-up tests for melanoma: update of current concepts. Arch Dermatol. 2004;140:107.
Patients presenting with localized stage I disease simply require a thorough history and physical examination. Many physicians advocate a screening chest radiograph, because the lung is the most common site for distant metastasis.68 Although a chest radiograph is an inexpensive, noninvasive means of metastatic evaluation, the rate of detection of occult pulmonary metastasis on chest radiograph in an asymptomatic patient with stage I or II disease is exceedingly low (0.1%).70,71 The high false-positive rate, 15%, necessitates additional and costly evaluations. Evidence supporting the use of other screening modalities, such as computed tomography (CT),72,73 liver-spleen scans, magnetic resonance imaging, and bone scans for patients with limited stage I and II disease is also lacking.74,75 For this reason, the National Comprehensive Cancer Network panel unanimously agreed that a search for visceral metastases, with either a chest radiograph or blood analysis, is not warranted for a patient with in situ or thin, stage IA lesions. A baseline chest radiograph is considered optional for thicker stage IB and II lesions. Imaging studies (CT, magnetic resonance imaging, positron emission tomography) may be obtained in this setting if there are specific concerning signs or symptoms.69 Screening serum lactate dehydrogenase (LDH) measurement carries a 15% false-positive rate, does not correlate with sentinel lymph node (SLN) status, and has not been helpful in detecting occult disease in asymptomatic patients.76 For this reason, our institution recommends LDH measurement only when the history or physical examination reveals jaundice, abdominal pain, or other specific findings that raise concern about distant metastasis.77
Patients with clinically or radiographically suspicious lymph nodes, satellite lesions, or in-transit metastasis (defined as intralymphatic tumor dissemination between the primacy lesion and draining nodal basin) are considered to have stage III disease and are at higher risk for distant metastasis. Fine-needle aspiration is an accurate and cost-effective means of confirming metastatic melanoma within lymph nodes.78 Additional imaging studies should be ordered according to the patient’s history and physical findings. A list of symptoms that warrant a focused investigation of systemic metastasis is summarized in Box 82-2.79 Overall, the yield of screening CT in patients with stage III melanoma has been low77,80–82; however, many physicians obtain the studies to serve as a baseline for future comparison.
Box 82-2 Review of Systems for Melanoma and Metastasis
Adapted from Johnson TM, Chang A, Redman B, et al. Management of melanoma with a multidisciplinary melanoma clinic model. J Am Acad Dermatol. 2000;42:820.
Patients with known stage IV disseminated melanoma require a complete evaluation for systemic metastasis. LDH measurements and chest radiography or chest CT are recommended. CT of the abdomen and pelvis, magnetic resonance imaging of the head, and a positron emission tomography scan (whole body) should also be considered. In this setting, workup is often dictated by clinical trial protocols. Unfortunately, greater survival has not been demonstrated for patients who are asymptomatic when diagnosed with their distant, stage IV disease than for their symptomatic counterparts76; however, this thorough evaluation may lead to a better quality of life.
Prognostic Factors and Tumor Staging
As a result of a greater understanding of the biology of cutaneous melanoma, the AJCC introduced a revised staging system in 2001.5,83 The goal of modifying the classification system was twofold. The main objective was to develop categories based on the most important independent prognostic markers for melanoma. Doing so may make it easier to identify cohorts of patients who have similar survival rates, thereby leading to increased homogeneity in future clinical trials. To achieve this goal, reliable prognostic markers recognized throughout the literature were studied among a cohort of 17,600 patients with melanoma from 13 major cancer institutions.83 This investigation marks the largest analysis of its kind to date. The second goal was to provide physicians with a practical classification system that mirrors clinical practice.
Summary of Revisions
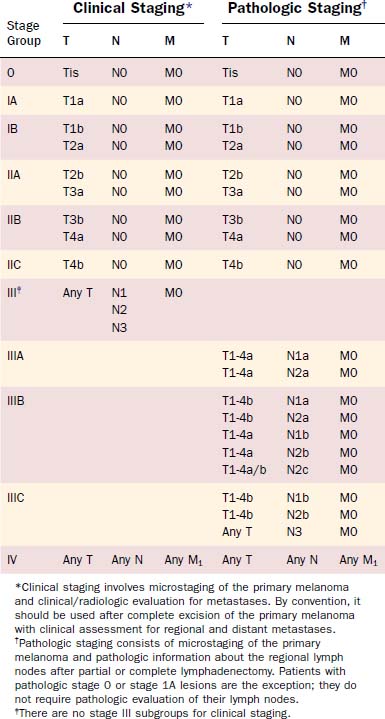
The current AJCC staging system for cutaneous melanoma remains founded upon the traditional tumor, node, metastasis (TNM) classification system (Tables 82-2 and 82-3). Stage I and stage II represent localized disease, stage III is regional disease, and stage IV is reserved for distant metastatic disease. The most important predictors for survival now serve as criteria for the definition of melanoma stage and are summarized in Box 82-3. Major revisions of the staging system are highlighted in Box 82-4.
Table 82-2 TNM Classification for Melanoma
| T Classification | Thickness (mm) | Ulceration Status |
|---|---|---|
| T1 | ≤ 1.0 mm | |
| T2 | 1.01-2.0 mm | |
| T3 | 2.01-4.0 mm | |
| T4 | > 4.0 mm |
| N Classification | No. of Metastatic Nodes | Nodal Metastatic Mass |
|---|---|---|
| N1 | 1 node | |
| N2 | 2-3 nodes | |
| N3 | 4 or more metastatic nodes, or matted nodes, or in-transit metastasis(es)/satellite(s) with metastatic node(s) |
| M Classification | Site | Serum Lactate Dehydrogenase Level |
|---|---|---|
| M1a | Distant skin, subcutaneous, or nodal metastases | Normal |
| M1b | Lung metastases | Normal |
| M1c |
* Micrometastases are diagnosed after sentinel or elective lymphadenectomy.
† Macrometastases are defined as clinically detectable nodal metastases confirmed by therapeutic lymphadenectomy or when nodal metastasis exhibits gross extracapsular extension.
Box 82-4 Revisions to the American Joint Committee on Cancer Staging System
From Schmalbach CE, Johnson TM, Bradford CR. The management of head and neck melanoma. Curr Probl Surg. 2006;43:797.
T Classification: Localized Disease
Multivariate analysis of 13,581 patients with localized disease identified tumor thickness and ulceration as the most important predictors of outcome. Overall, tumor thickness was the most powerful prognostic indicator for this subgroup. The 1997 staging system had employed the empirically based Breslow depth of 0.75 mm to differentiate T1 from T2 lesions.84 The revised staging system now uses even-integer cut-points of 1.0, 2.0, and 4.0 mm to delineate T stage. These new cut-points represent the best statistical fit in the correlation of tumor thickness and survival.
In the previous staging system, histologic level of invasion, as represented by the Clark scale (Fig. 82-2), was also used in the definition of T classification. However, the analysis by Balch and associates83 found the histologic level of invasion to be prognostic only for thin T1 lesions. For tumors 1 mm or thinner without ulceration, invasion to Clark level II or III is considered T1a, whereas invasion into the reticular dermis (level IV or V) is considered T1b. With the exception of T1 lesions, Clark level of invasion is no longer used in staging melanoma.
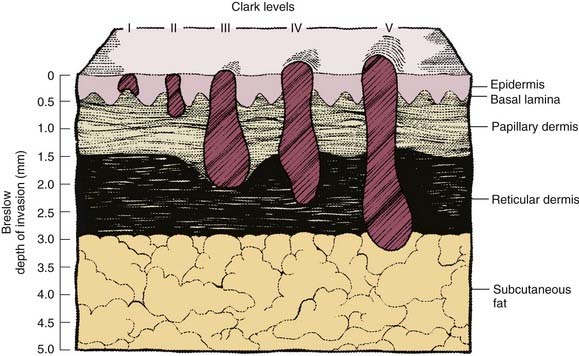
Figure 82-2. Schematic representation of cutaneous melanoma invasion according to Clark level and Breslow microstaging.
Tumor ulceration was the second most important prognostic indicator for patients with localized disease. Ulceration is not a visible crater on gross examination but, rather, a histologic diagnosis in which intact epidermis overlying the melanoma is absent. Survival rates were found to be significantly lower for all patients with ulcerated lesions than for their counterparts without ulceration. In fact, the survival of patients with ulcerated tumors mirrored that of patients with nonulcerated tumors in the next highest T categories; for this reason, ulceration warrants classification of a tumor to a higher stage. The prognostic significance of ulceration85 and the correlation between ulceration and mitotic rate have been reported.86,87 Although mitotic rate was not evaluated during the revision of the AJCC staging system, it may become an important prognostic marker in the future.
Nodal Classification: Regional Disease
Similar multivariate analysis was performed in more than 1000 patients with melanoma diagnosed with lymph node metastasis. The following three prognostic factors met statistical significance, at P < .0001: (1) number of metastatic lymph nodes, (2) tumor burden as represented by microscopic versus macroscopic disease, and (3) primary tumor ulceration. The gross diameter of metastatic nodes was previously used in N classification but is no longer incorporated into the staging system owing to a lack of compelling evidence supporting its predictive value.72,88
Overall, the most important predictive marker for patients with nodal metastasis was the number of positive lymph nodes.83 The greatest difference in 5-year survival rates was used to subclassify the N category. Patients with one metastatic node are now categorized as having N1 disease, patients with two or three metastatic nodes as having N2, and patients with four or more nodes as having N3.
The second most important prognostic indicator for patients with regional metastasis was tumor burden. Patients identified as having microscopic nodal disease, through either SLNB or elective lymphadenectomy, were found to have a significantly better survival than individuals diagnosed with macroscopic disease on the basis of clinical or radiographic examination.83
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


