The presence or absence of a malleus affects the hearing results in ossiculoplasty, particularly in the absence of a stapes superstructure. Numerous authors have emphasized the importance of the malleus in successful ossiculoplasty,1,2,3,4 and re-creation of the malleus has been used by several authors to enhance middle ear prosthesis stability.5,6,7
The presence of an anteriorly positioned malleus may also be a difficult situation for the otologist. In cases of an absent or a severely anterior malleus, the usual methods of ossiculoplasty presented in the literature have used reconstruction from the stapes head (or footplate) directly to the eardrum.8,9 However, placement directly under the medial surface of the eardrum increases the possibility of both perforation and extrusion.8,10 These ossicular reconstructions are frequently unstable because the lack of fixation by the malleus at the proximal end of the prosthesis can allow displacement at either the proximal or distal ends. Many authors believe that an acoustic benefit can be achieved by attaching the prosthesis to the manubrium of the malleus, as opposed to attaching it directly to the tympanic membrane, because of the catenary lever action of the malleus-tympanic membrane assembly.
Mounting evidence in the literature confirms the presence of the malleus as an important prognostic factor in ossiculoplasty, leading to better hearing results and lower rates of extrusion due to its role in preventing tympanic membrane lateralization.11 De Vos, Gersdorff, and Gérard reiterated the absence of the malleus as an adverse prognostic factor because its presence not only gives stability to the reconstruction, but also acts as catenary lever, thereby contributing to acoustic gain.12 However, it is not only the presence of the malleus, but also its position in relation to the stapes, that affects hearing outcomes. Vlaming and Feenstra demonstrated that the ideal reconstructive situation was when the malleus was positioned directly over the stapes. In practice, this anatomic configuration is very rarely seen but can be easily achieved with malleus relocation techniques.13 The theory is that all of the force of vibration through a strut prosthesis would be converted into an efficient piston-like motion at the footplate.
When the malleus is malpositioned, ossiculoplasty is often unstable and mechanically inefficient, particularly if the malleus is angulated more than 45 degrees from the axis of the stapes superstructure or footplate.14 Malleus relocation acts to reduce the angle to zero as the relocated malleus is positioned over the stapes head or footplate, allowing ideal placement of the prosthesis. In addition, this configuration allows an almost perpendicular direction of forces to the footplate, with optimal transfer of function and minimal dissipation of energy.
The Austin15 classification of ossicular defects as modified by Kartush8 provides a method for defining pre-reconstruction ossicular status. Presence of a malleus can be classified in Austin-Kartush Groups A (malleus and stapes intact and mobile) and B (malleus and stapes footplate present and mobile, stapes superstructure absent). An absent malleus can be classified in Austin-Kartush Groups C (malleus absent and stapes intact and mobile) and D (malleus and stapes superstructure absent, stapes footplate present and mobile). Our surgical technique of ossicular reconstruction will be presented for each of these four classifications.
30.2 Surgical Technique
30.2.1 Austin-Kartush Group A (Malleus and Stapes Intact and Mobile)
Reconstruction of the ossicular chain when the stapes and malleus are both present typically involves the use of a partial reconstruction prosthesis or incus autograft between the stapes head and the malleus handle or tympanic membrane, with or without supportive tissue to strengthen the tympanic membrane. Few authors advocate the use of a total reconstruction prosthesis from the footplate of a normal stapes to the malleus.1,2,8,15
Described here are two previously published original techniques: the malleus relocation technique11 and the Silastic banding technique.16 The malleus relocation technique allows for better placement of both partial (PORPs) and total ossicular replacement prostheses (TORPs). With the Silastic banding technique, a TORP is positioned from the stapes footplate to the relocated malleus despite the presence of a stapedial arch. The TORP is attached to the intact stapes superstructure with a band that allows for better prosthesis stability.
From 1991 to 2000, the author used a PORP positioned from the malleus to the stapes head in Austin-Kartush Group A cases. Since January 2000, the author has used a combined technique of malleus relocation and Silastic banding, and a TORP is inserted in all cases.
Malleus Relocation Technique
Entire separation of the malleus from the tympanic membrane is required (▶ Fig. 30.1; ▶ Fig. 30.2). Any remnant of the incus (even within the epitympanum) must be removed. The tensor tympani is sectioned as close as possible to its insertion into the malleus handle (▶ Fig. 30.3). Relocation of the malleus is performed using a strong 90-degree hook placed anterior to the neck of the malleus. Progressive posterior retraction of the malleus is applied until it comes to lie directly above the stapes capitulum or footplate (▶ Fig. 30.4). Subsequent anterior retraction of the malleus is avoided by overstretching the anterior malleal ligament, the position thereby being maintained by the superior ligament of the malleus, which is preserved (the malleus head is not removed). In the relocated position, the malleus should lie immediately over the stapes footplate (▶ Fig. 30.5). Precise measurement from the relocated malleus to the stapes capitulum or footplate can then be undertaken using a modified stapes-measuring rod (▶ Fig. 30.6).
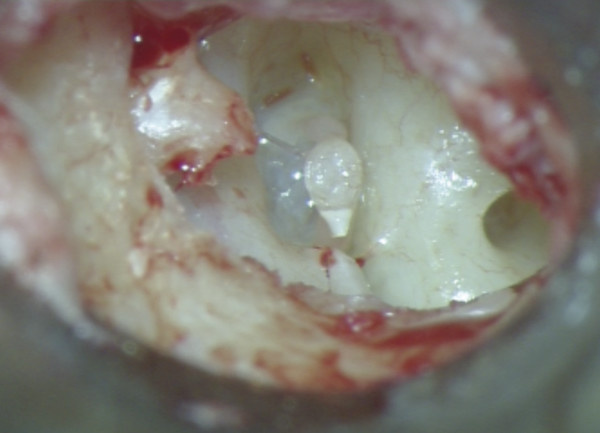
Fig. 30.1 Operative view of a right ear showing evidence of incus erosion, Austin-Kartush Group A. Both the stapes and malleus are mobile.
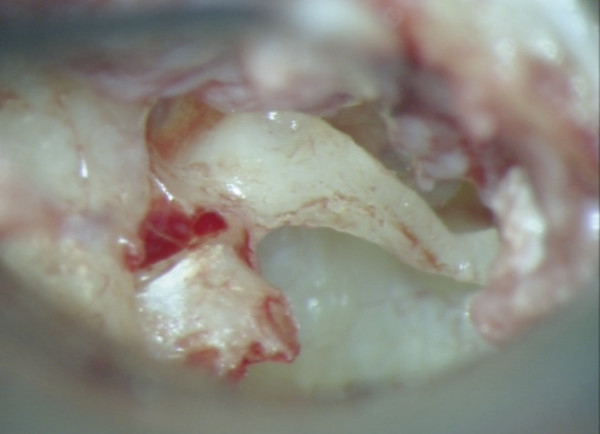
Fig. 30.2 The malleus is completely separated from the tympanic membrane.
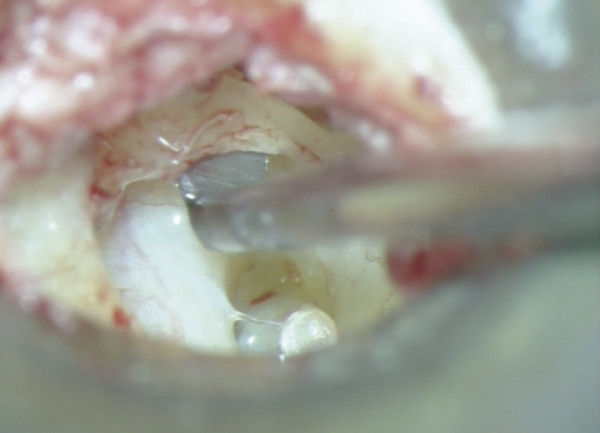
Fig. 30.3 The tensor tympani is sectioned as close as possible to its insertion into the malleus handle.

Fig. 30.4 Progressive posterior retraction of the malleus is applied until it comes to lie directly above the stapes capitulum or footplate.

Fig. 30.5 The relocated malleus should lie immediately over the stapes footplate.
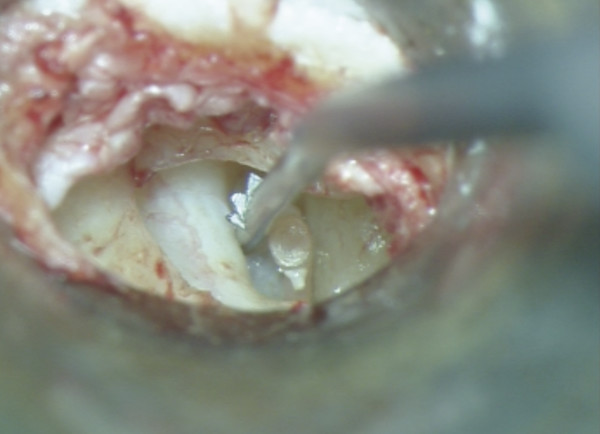
Fig. 30.6 Precise measurement from the relocated malleus to the stapes capitulum or footplate can be undertaken using a modified stapes-measuring rod.
Silastic Banding Technique
A Silastic band is fashioned by creating a 1.2-mm disc from a thin sheet of Silastic using a specially designed punch (Medtronic-Xomed, Inc., Jacksonville, Florida). The center of the disc is then fenestrated with an 0.8-mm diameter punch (▶ Fig. 30.7). The band should fit snugly around the stapes neck. The stapedius tendon is divided as closely as possible to the pyramid because an attempt will be made to place the band beneath the stapedius tendon to avoid lateral displacement of the band. The prosthesis shaft is cut to the appropriate length and is introduced through the band (▶ Fig. 30.8). The shaft is introduced between the stapes and the Fallopian canal, with the distal end being lowered onto the center of the footplate (▶ Fig. 30.9a). The head of the prosthesis is then introduced under the relocated malleus handle (▶ Fig. 30.9b). In its final position, the prosthesis head should rest directly under the malleus handle without undue tension, and the malleus neck should stay away from the superior wall of the external auditory canal.
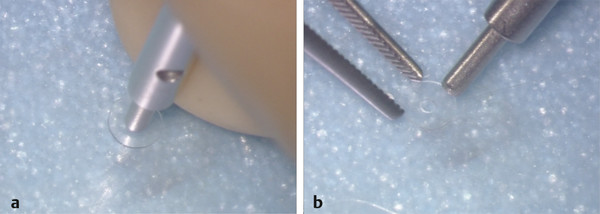
Fig. 30.7 (a) A Silastic band is fashioned by creating a 1.2-mm disc from a thin sheet of Silastic using a specially designed punch (Medtronic-Xomed, Inc., Jacksonville, Florida). (b) The center of the disc is then fenestrated with a 0.8-mm diameter punch.

Fig. 30.8 The prosthesis shaft is cut to the appropriate length and introduced through the band.
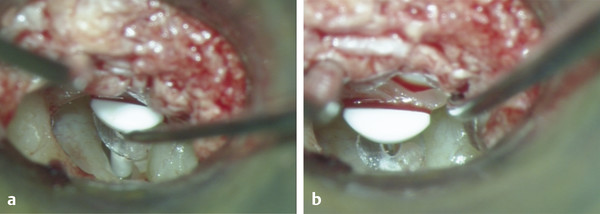
Fig. 30.9 (a) The shaft is introduced between the stapes and the Fallopian canal with the distal end being lowered onto the center of the footplate. (b) The prosthesis head is then introduced under the relocated malleus handle.
The band is then gently pulled and positioned around the stapes capitulum, beneath the stapes tendon, which had been cut. By snugging the band down over the sectioned tendon, the prosthesis becomes firmly apposed to the stapes, allowing precise placement on the stapes footplate with sufficient rigidity (▶ Fig. 30.10). This assembly facilitates an almost perpendicular position of the prosthesis from the footplate to the malleus handle and tympanic membrane. By keeping the distal end of the prosthesis in proper position using the Silastic band, the tendency of the prosthesis to tip or migrate is virtually eliminated. This combined technique of malleus relocation and Silastic banding results in an increasingly stable and more functional ossicular arrangement (▶ Fig. 30.11).
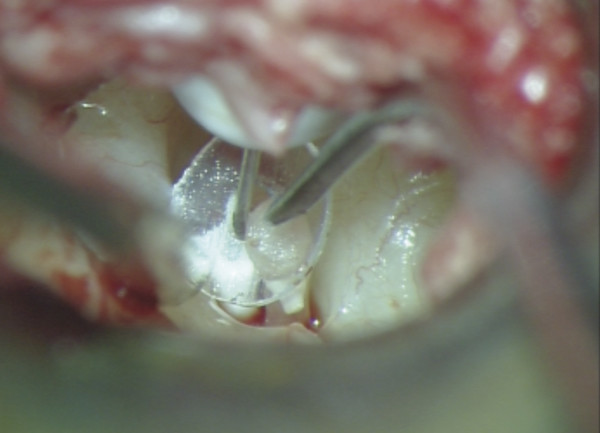
Fig. 30.10 The band is then gently pulled and positioned around the stapes capitulum.
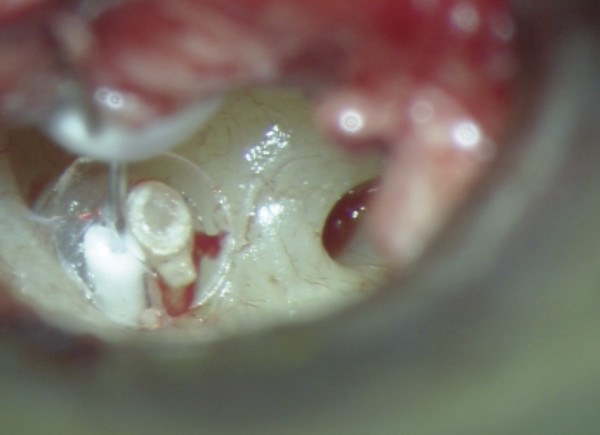
Fig. 30.11 Final view of surgical field, Austin-Kartush Group A. The prosthesis is in an almost perpendicular position from the footplate to the malleus handle and tympanic membrane and is kept in proper position by the band.
30.2.2 Austin-Kartush Group B (Malleus and Stapes Footplate Present and Mobile, Stapes Superstructure Absent)
In cases of absent stapes superstructure with a mobile malleus, a TORP is interposed to restore the transfer function of the middle ear. The malleus-to-footplate prosthesis connects the malleus to the footplate. The malleus is relocated using the malleus relocation technique described above (▶ Fig. 30.12; ▶ Fig. 30.13).
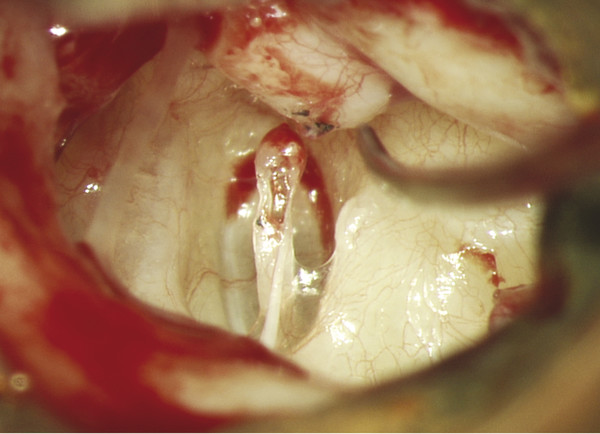
Fig. 30.12 Operative view of a left ear, Austin-Kartush Group B. Both the incus and stapes capitulum have been eroded. The eroded capitulum does not allow for the use of a PORP.
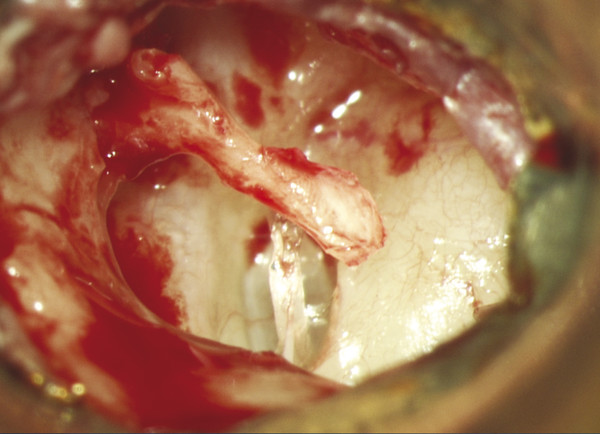
Fig. 30.13 The malleus is dissected free from the tympanic membrane and relocated in a position over the stapes footplate.
When the footplate appears to be very thin and fragile, it should be protected by an interposed vein graft. The technique of positionning the TORP is the same. The prosthesis is cut to the appropriate length as the shaft of the prosthesis must fit snugly onto the center of the footplate. The prosthesis head is then introduced under the relocated malleus handle (▶ Fig. 30.14). It is important to obtain a perpendicular position of the prosthesis from the footplate to the malleus handle.
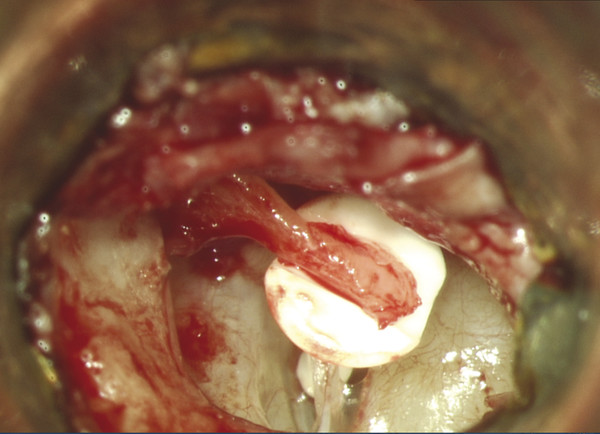
Fig. 30.14 Final view of surgical field, Austin-Kartush Group B. The prosthesis is cut to the appropriate length. The shaft of the prosthesis must fit snugly onto the center of the footplate. The prosthesis head is then introduced under the relocated malleus handle.
30.2.3 Austin-Kartush Group C (Malleus Absent, Stapes Intact and Mobile)
Reconstruction of the ossicular chain when the stapes is present and the malleus is absent typically involves a PORP between the stapes head and tympanic membrane or graft surface.8,9 However, these ossicular reconstructions are frequently unstable because the lack of fixation by the malleus at the proximal end of the prosthesis can allow displacement at either the proximal or distal ends. The Silastic banding technique is used by the author in all Austin-Kartush Group C cases, and a TORP is positioned from the stapes footplate to the tympanic membrane, despite the presence of a stapedial arch. The TORP is attached to the intact stapes superstructure. As previously described, the band allows for better prosthesis stability, thus eliminating tipping or migration. This configuration prevents prosthesis displacement and avoids contact with the promontory or the posterior canal wall. The Silastic banding technique also prevents undesirable contact with a dehiscent or overlying facial nerve. In many ears with an intact stapes superstructure, there is enough room between the horizontal segment of the facial nerve and the stapes superstructure to place the shaft of a TORP. We prefer this location because it provides a reliable vertical alignment of the prosthesis with the overlying tympanic membrane. However, if a dehiscent facial nerve is too close to the stapes superstructure, the shaft of the prosthesis is positioned on the other side, between the stapes and the promontory.
In general, determining the exact length of a prosthesis can prove to be difficult when the malleus is absent. This new technique achieves an almost perpendicular position of the prosthesis to the footplate and the tympanic membrane, allowing the use of an elongated stapes measuring rod (Xomed-Medtronic) for precise measurement within 0.5 mm, even in cases of lateralized tympanic membranes. The tympanomeatal flap is replaced in its anatomic position to verify the position of the head of the prosthesis beneath the under-surface of the tympanic membrane.
It is also possible to use a newly designed malleus replacement prosthesis (MRP) in Austin-Kartush Group C cases, which is combined with a TORP. This will be described in the Austin-Kartush Group D cases.
30.2.4 Austin-Kartush Group D (Malleus and Stapes Superstructure Absent, Stapes Footplate Present and Mobile)
In cases where the malleus and stapes are both missing, the author uses a newly designed titanium MRP, which was created in 2009 in collaboration with Heinz Kurz, Inc. (Dusslingen, Germany), to replace a missing malleus as an attempt to reduce the risk of prosthesis dislocation (▶ Fig. 30.15). Prior to the introduction of the MRP, the TORP head was universally placed in direct contact with the tympanic membrane (tympanic membrane-to-footplate assembly). The MRP is designed to be affixed to the bony ear canal to provide superior stabilization of a total or partial prosthesis coupled to it. A TORP is positioned from the MRP to the stapes footplate (MRP-to-footplate assembly) in all Austin-Kartush group cases (▶ Fig. 30.16).
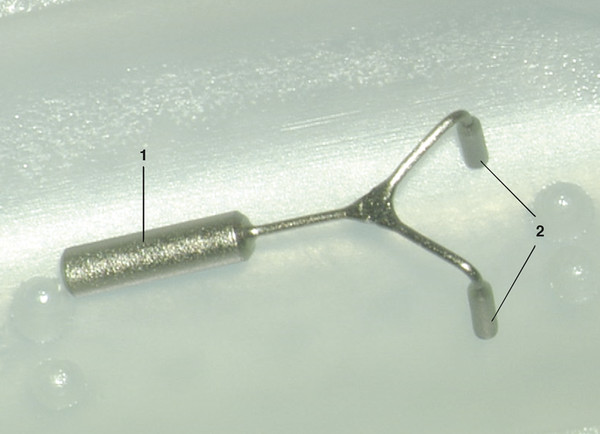
Fig. 30.15 Malleus Replacement Prosthesis (MRP). 1=0.8-mm diameter handle; 2=0.3-mm diameter posts that will be inserted in the external auditory canal.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


