Purpose
To describe the clinical course and ancillary findings of 3 patients with choroidal melanoma who inadvertently received multiple intravitreal injections of bevacizumab for a presumed diagnosis of choroidal neovascular membrane.
Design
Observational case series.
Methods
Three patients with choroidal melanomas who received a series of monthly intravitreal injections of bevacizumab for presumed choroidal neovascularization were evaluated. Clinical, ultrasonographic, and angiographic findings are presented. Histopathologic features are correlated with clinical features in 2 patients who underwent enucleation.
Results
Lack of benefit in halting tumor progression was observed in all 3 cases. In 2 cases treated with enucleation, there was evidence of bevacizumab-induced gliotic/fibrotic retinal changes.
Conclusions
We present 3 cases of choroidal melanomas that showed progression while patients received multiple intravitreal injections of bevacizumab. The use of the drug led to the formation of a gliotic/fibrotic membrane that resulted in masking of the underlying tumor and consequently delayed the correct diagnosis.
The diagnostic accuracy of uveal melanoma is high in the majority of eyes with clear media, based on ophthalmoscopic findings and ultrasonographic and angiographic features. However, atypical cases may be confused with other simulating lesions including hemorrhagic processes, choroidal metastases, and retinal pigment epithelium tumors. In such cases diagnostic biopsy is commonly performed.
We describe the clinical course and ancillary findings of 3 patients who received several intravitreal injections of bevacizumab at monthly intervals for a presumed choroidal neovascular membrane, who were later diagnosed with a choroidal melanoma. Lack of benefit in avoiding tumor progression was observed in all 3 cases. Moreover, use of bevacizumab resulted in masking of the underlying tumor and consequently delayed the correct diagnosis. In 2 cases enucleation was performed, providing evidence of bevacizumab-induced retinal changes.
Case Report
Case 1
A 55-year-old white woman presented to the Cole Eye Institute in November of 2009 for further investigation of a peripapillary lesion of the right eye. In December of 2007, she was evaluated at another institution because of complaints of decreased vision. At that time, her best-corrected visual acuity was 20/40 in the right eye and 20/20 in the left eye. Findings were limited to the right eye, where optical coherence tomography (OCT) disclosed the presence of subretinal fluid in the peripapillary region. She was treated with 5 intravitreal injections of bevacizumab (1.25 mg/0.05 mL), at monthly intervals, for a presumed idiopathic peripapillary choroidal neovascular membrane, with initial reduction of the subretinal fluid. She was lost to follow-up until January of 2009. Her condition worsened during this interval and her visual acuity dropped to 20/200 in the right eye. Intravitreal bevacizumab therapy was reinstated, but there was lack of improvement. A full battery of tests to check for underlying infectious, autoimmune, and connective tissue disorders was unremarkable.
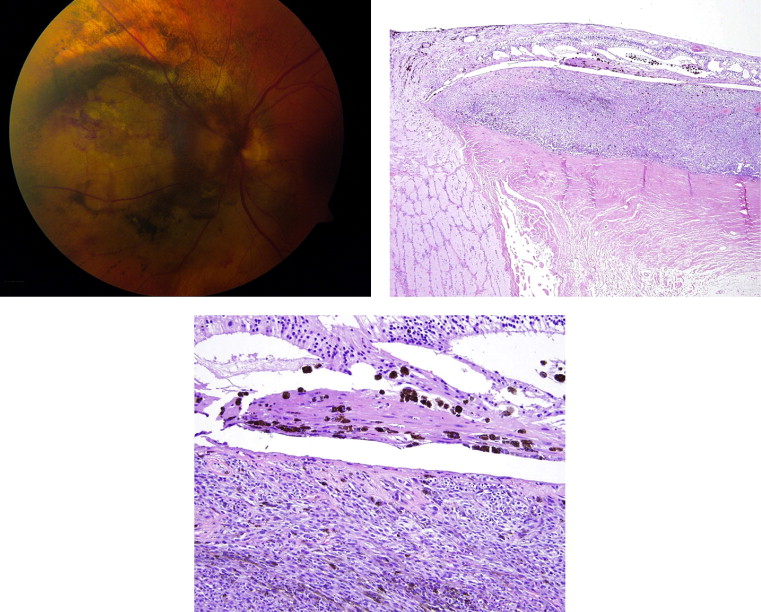
Upon presentation, visual acuity was count fingers at 6 feet in the right eye and 20/20 in the left eye. An afferent pupillary defect was present in the right eye. Anterior segment examination was normal in both eyes, without evidence of heterochromia or melanocytosis. Dilated fundus examination was unremarkable in the left eye. Examination of the right eye demonstrated a pale yellow peripapillary choroidal mass ( Figure 1 , Top left). There was evidence of optic disc swelling with intraretinal hemorrhages. Ultrasonography revealed a dome-shaped, slightly irregular, choroidal mass, 11 × 10.5 mm in basal dimension and 4.1 mm in height, with a suggestion of extraocular extension ( Figure 1 , Top right). Although the lesion had low reflectivity, intrinsic vascularity was absent. Indocyanine green (ICG) angiography demonstrated a large hypofluorescent choroidal lesion surrounding the optic disc, without intrinsic vessels ( Figure 1 , Middle left). The hypofluorescence extended late into the study, which did not support the diagnosis of choroidal melanoma. A presumptive diagnosis of choroidal metastasis was made. Computed tomography (CT) scan of the chest, abdomen, and pelvis and a mammogram did not identify a primary site.
A fine-needle aspiration biopsy of the choroidal lesion was performed, which was positive for malignant cells, suspicious for malignant melanoma. Cytokeratin AE1/3 immunostain and S100 immunostain were inadequate because of insufficient cellularity. A second fine-needle aspiration biopsy was then performed. The cellular features were consistent with melanoma. Immunostaining was positive for HMB-45 and negative for cytokeratin AE1/3, further supporting the diagnosis of choroidal melanoma. After discussing treatment options with the patient, decision was made to proceed with enucleation.
The pathology of the surgical specimen revealed a slightly pigmented peripapillary choroidal malignant melanoma ( Figure 1 , Middle right). Eighty percent of the cells were spindle B type and 20% epithelioid. The tumor was positive for melan A and negative for cytokeratins CK7 and AE1/3, consistent with melanoma and ruling out a metastatic carcinoma ( Figure 1 , Bottom left). There was tumoral involvement of the optic nerve to the lamina cribrosa, and the tumor invaded deeply into the sclera adjacent to the optic nerve. Overlying the tumor was a large GFAP-positive gliotic plaque measuring 1.1 mm in thickness ( Figure 1 , Bottom right). Prominent vessels were present within the plaque and there was focal calcification. An attempt to determine the presence of vascular endothelial growth factor (VEGF) and VEGF receptor by immunoperoxidase method gave noncontributory results. There was no iris neovascularization. By fluorescence in situ hybridization analysis, the tumor was found to be monosomic for chromosome 3 with gain of chromosome 6p. 8q24 amplification was not observed.
Case 2
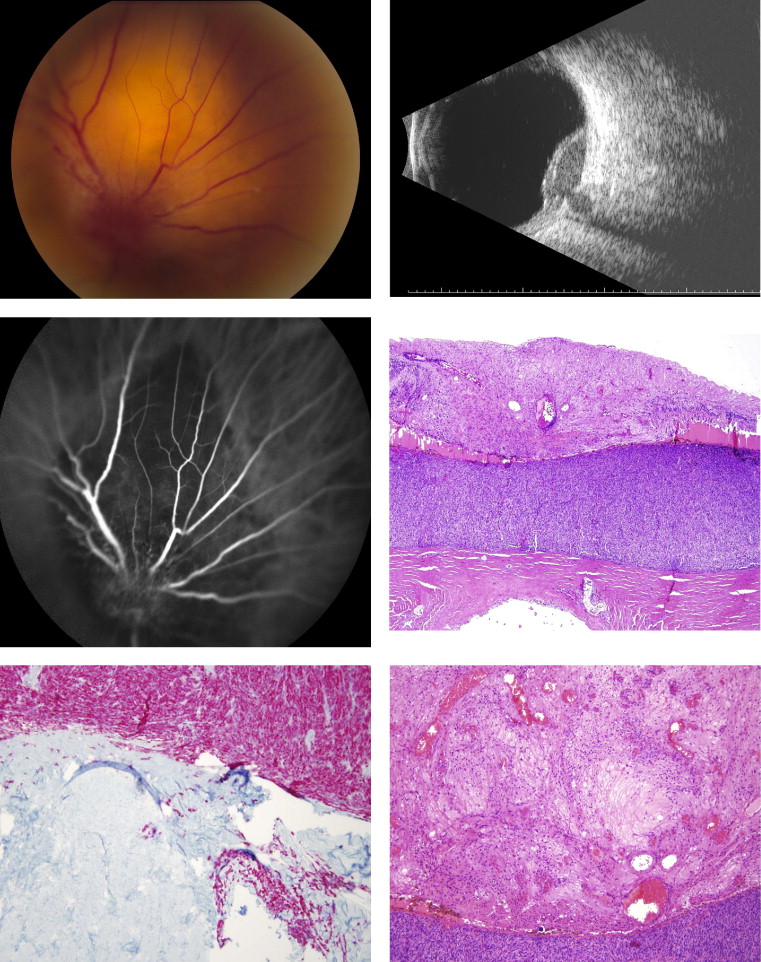
A 60-year-old white woman was referred to the Cole Eye Institute for evaluation of a choroidal lesion nasal to the disc in the left eye. The patient had initially presented to another institution in October of 2008 with complaints of decreased vision. Her visual acuity was 20/25 in the right eye and 20/80 in the left eye. Examination of the right eye was normal. A large area of subretinal hemorrhage that partially obscured the disc was observed in the left eye, and extended nasally, superiorly, and inferiorly. A B-scan showed an elevated homogeneous pseudotumoral lesion around the optic nerve. OCT demonstrated an area of sub-retinal pigment epithelium fluid inferonasal to the optic disc. ICG angiography was not performed because of iodine allergy. She was presumed to have a juxtapapillary choroidal neovascularization nasal to the disc and was treated with a series of 4 intravitreal injections of bevacizumab (1.25 mg/0.05 mL), at 4-week intervals, with initial resolution of the subretinal fluid. In January of 2009, recurrent subretinal fluid was noted on OCT, with persistent residual dark mass nasal to the disc.
Visual acuity was 20/25 in both eyes upon presentation to our service in February of 2009. Anterior segment examination of both eyes and dilated fundus evaluation of the right eye were unremarkable. A juxtapapillary flat pigmented mass in the nasal quadrant was identified in the left eye ( Figure 2 , Top left). The basal dimension of the mass was 12.0 × 11.0 mm with a height of 2.0 mm. Extension of the pigment obscured the nasal half of the disc and overlying retinal vessels. Deeper choroidal mass encircling the optic disc was also noted. There was evidence of regressed subretinal fluid along the superior margin and intraretinal pigment migration inferiorly. Abnormal intrinsic vessels within the lesion could not be identified.