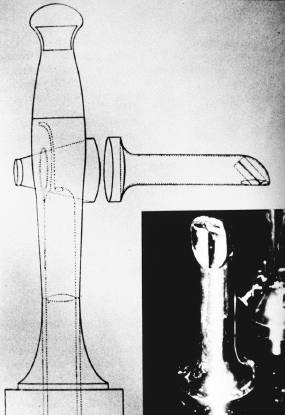
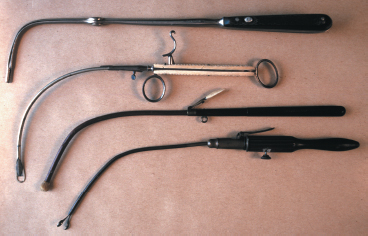
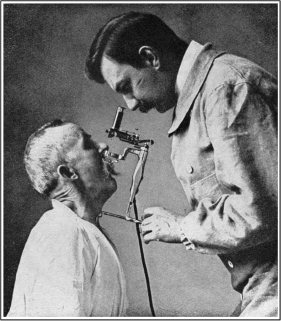
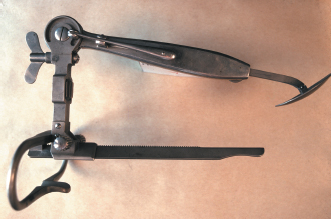
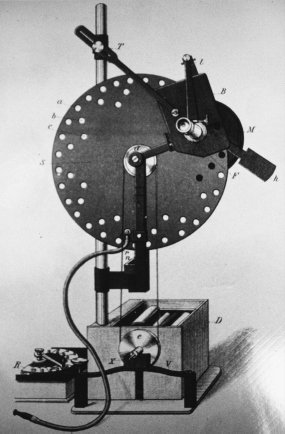
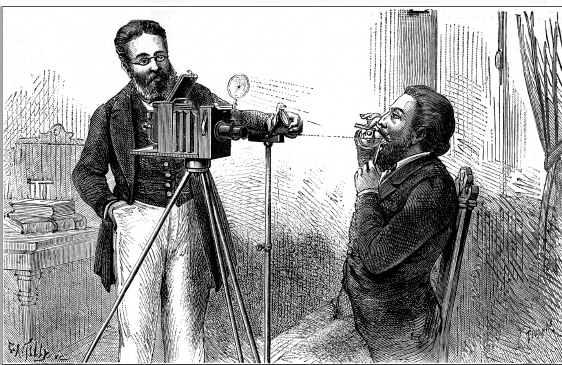
1 The origin and development of laryngeal imaging chronicles the initiation of the field of laryngology, and improved imaging continues to provide the foundation for a majority of the developments in our specialty today. Observing the larynx with high resolution and great precision allows for our understanding of normal/abnormal anatomy and function, which is the basis of designing treatment strategies. A primary focus of 19th century laryngology was mirror-guided management of laryngeal airway obstruction, primarily from infectious diseases of the upper aerodigestive tract.1 This continued into the early 20th century when Kirstein, Killian, and Jackson popularized direct laryngoscopic surgery, which was invaluable for treating cancer, stenosis, and a spectrum of benign phonatory lesions. Later in the 20th century, the key imaging advancements were stereoscopic magnified laryngoscopy in the operating room as well as office-based flexible laryngoscopy and stroboscopy. Today, researchers are exploring the value of highspeed imaging of vocal fold vibration. The origin and growth of laryngology is inextricably linked to the development of endoscopic laryngeal imaging and laryngoscopic surgery. Phillip Bozzini (1773–1809) was the first individual to suggest that image-controlled endoscopic surgery was possible and is therefore considered to be the father of minimally invasive surgery (Fig. 1.1)2 In 1807, at the age of 34, he described the Lichtleiter (“light conductor”), which was composed of a universal handle that incorporated a candle and a reflector as an extracorporeal light-source (Fig. 1.2). He attached a variety of cannulae to the handle to facilitate the examination of accessible orifices (i.e., throat, urethra, rectum). This concept was a revolutionary advancement in medical and surgical science, but his work continues to be largely unrecognized. The laryngeal cannula consisted of an additional mirror that allowed for visualization of the lower pharynx and larynx. Unfortunately, the medical community did not embrace Bozzini’s method, and he died in 1809 before the validity of his approach could be established. There were several other reports of mirror laryngoscopy in the first half of the 19th century; however, none were widely acknowledged or accepted.3–9 Most notable were the descriptions by Babington, Liston, and Avery.3,4,7 Babington first used the term glottoscope (1829) for his instrument, which consisted of a variety of mirrors as well as a retracting spatula to distract the tongue base. By retracting the tongue base out of the visual field, Babington’s glottoscope became the first device to employ internal distension of supraglottal tissues to enhance visualization of the glottis.10,11 Liston’s brief description of mirror laryngoscopy (1837) for the assessment of laryngeal edema was important because he introduced the concept of heating the mirror to avoid condensation on the reflecting surface.7 Avery (1844) designed a laryngeal cannula similar to Bozzini’s, however he employed an artificial light source separate from the device in the form of a headlight.3 This remarkable device employed a perforated concave mirror to reflect the illumination into the oropharynx to facilitate visualization of the larynx. Fig. 1.1 Phillip Bozzini (1773–1809). Manual Garcia (1805–1906), the renowned vocal pedagogist, reported auto-laryngoscopy to the Royal Society of London in 1855 (Fig. 1.3).12 This investigation was catalyzed by his desire to better understand singing phonation. In his paper entitled “Observations on the Human Voice,” Garcia made important contributions to the understanding of laryngeal sound production especially with regard to rhythmic pulsation of the expiratory airstream. Clerf believed that Garcia’s emphasis on observations and deductions regarding laryngeal physiology led to the subsequent widespread adoption of mirror laryngoscopy by physicians, which had not occurred as a result of prior 19th century descriptions of the technique.13 Fig. 1.2 Bozzini’s Lichtleiter (“light conductor”). Note the line drawing displaying a universal handle with a candle as a light source; the laryngeal speculum is seen in the inferior right in the inset photograph. There is little debate that laryngology was born from the imaging investigations of the acclaimed classical voice teacher. In addition to inspiring the genesis of this new field in medicine, Garcia maintained active engagement with laryngologists as the field developed from its infancy. This is evidenced in Mackenzie’s text, The Hygiene of the Vocal Organs.14 The tremendous esteem that laryngologists held for Garcia was vividly illustrated in Mackinlay’s description of the celebration for the maestro’s 100th birthday (1906).15 Laryngologists commissioned John Singer Sargent to paint Garcia for his centennial birthday. It appears that Garcia was too frail to remain stable for the entire process. Sargent is reported to have used a photograph as a model for the majority of the painting, whereas the head and hands were derived from the live sitting. Fig. 1.3 Manuel Garcia (1805–1906) at approximately 80 years old. In 1857, Turck explored, but then abandoned, the clinical application of mirror laryngoscopy.16 He could not obtain a reliable image because, like Garcia, he was depending on the sun for illumination, and unfortunately it was often overcast in Pesth in the autumn. Shortly thereafter, his colleague Czermak borrowed the same mirrors and commenced further investigations, which were highly successful (Fig. 1.4).17 Czermak reintroduced the artificial light source and the perforated concave mirror. A feud developed between Czermak and Turck over priority for the medical application of mirror laryngoscopy. The most important aspect of the dispute between Turck and Czermak was that the bitter quarrel fueled attention in the Western world toward the fledgling field of laryngology. Both pioneers immediately concentrated on educating physicians in the technique of laryngoscopy by convening clinics throughout Europe. This dissemination of knowledge led to the development of a watershed of instruments and contributions (Fig. 1.5). Fig. 1.4 Johann Nepomuk Czermak (1828–1873). Stoerk (1859) reported the first laryngoscopically controlled manipulation of the laryngeal tissues, which involved the topical application of silver nitrate to the larynx.18 Lewin (1860) was the first to report on the laryngoscopically guided management of laryngeal tumors.19 In his series of 50 neoplasms, he excised three and applied caustics to four others. Mackenzie introduced mirror laryngoscopy to Great Britain after attending Czermak’s clinic.20 He acquired acclaim as a surgical innovator and a prolific author.21,22 In 1886, Fraenkel published the first report of a transoral resection of a laryngeal cancer.23 In the United States, laryngoscopy and laryngology were initially slow to develop due to the concurrent outbreak of the U.S. Civil War. Near the end of the conflict, Louis Elsberg (1837–1885), who attended the Jefferson Medical College in 1860, published the first formal American book (1864) in laryngology and endolaryngeal treatment.24 Soon thereafter, he received the Gold Medal from the American Medical Association for his publication entitled Laryngoscopal Surgery Illustrated in the Treatment of Morbid Growths within the Larynx.25 Fig. 1.5 Various laryngeal instruments. Similar to virtually all laryngologists of the day, Elsberg was a physician and not a trained surgeon. Yet Jacob da Silva Solis-Cohen (1838–1927), at the conclusion of his Civil War service as a surgeon in the Union Navy and Army, was influenced to become a laryngologist by his boyhood friend and medical-school classmate—Elsberg. To the best that the authors can document, Solis-Cohen became the first formally trained surgeon to become a laryngologist, which was based on mastering mirror-guided imaging. This imaging skill allowed for surgical procedures, which fueled the progress of laryngology. Solis-Cohen’s professional development became a critical turning point in the history of laryngology, laryngeal surgery, and ultimately phonosurgery. He combined his newly acquired laryngoscopic skills with rigorous surgical training and wartime experience to the fledgling medical specialty of laryngology. Most likely, he is the first specialist head and neck surgeon in history and was probably the first individual to cure a laryngeal cancer, which was done by means of a laryngofissure and hemilaryngectomy.26,27 Solis-Cohen realized and taught that precise management of the upper aerodigestive tract disorders required both endoscopic and open surgical skills. This philosophy was vividly displayed in his magnum opus (1872), Diseases of the Throat: A Guide to the Diagnosis and Treatment, which was the benchmark for textbooks of its kind for decades.28 As a young man, Chevalier Jackson personally borrowed Solis-Cohen’s texts. It is likely that his compendium, Peroral Endoscopy and Laryngeal Surgery, is modeled after Solis-Cohen’s text.29 The isolated reports of mirror laryngoscopy in the early 19th century arose from the need to image the airway. Infectious diseases were a formidable problem that could cause membranous laryngeal airway obstruction.30,31 Horace Green (1802–1866) dedicated his career to this problem and spent time with Trousseau and Belloc in Europe. He became the first specialist for throat and respiratory diseases in the United States (Fig. 1.6). Green described blind transoral application of caustics to the larynx to treat infectious inflammatory disorders of the laryngeal membranes, as reliable laryngeal imaging was yet to be discovered.32–34 However, he was maligned by his contemporaries, who did not believe that his transoral interventions were possible.35–37 Later, Green resolved this skepticism by placing a whalebone probang transorally through the glottis of a patient who had a tracheotomy until the probang could be observed through the tracheotomy site. Fig. 1.6 Horace Green (1802–1866). In 1852, Green made his most seminal contribution to laryngology by describing the first direct laryngoscopy and visually controlled excision of a laryngeal neoplasm. He was managing a child with obstructive sleep apnea. He excised her tonsils, which did not resolve the problem. Subsequently, he inserted a bent tongue spatula (similar to a Macintosh laryngoscope) and was able to observe a ball-valving fibroepithelial polyp obstructing the glottal aperture. Using sunlight for illumination, he was able to successfully observe and resect the lesion due to the favorably cephalad position of the child’s larynx. He reported the case in detail in his landmark textbook, On the Surgical Treatment of Polypi of the Larynx, and Oedema of the Glottis.38 The book contained a drawing of what the artist could view during the procedure. Both Bozzini and Green were courageous figures in medical history, as their work was not accepted by their contemporaries, who could not replicate their techniques. They were both branded as charlatans by the general medical establishment. Although Bozzini died shortly after his book was published, Green lived through the initial period of the origin of laryngology and he was vindicated. Louis Elsberg, the first president of the American Laryngological Association, dedicated that organization’s first meeting in 1879 to Green and referred to him as the father of American laryngology because of his brilliant skill and courageous contributions.37 No attempt to repeat Green’s 1850s work with direct laryngoscopy occurred until the end of the 19th century. Unaware of Green’s accomplishment, Kirstein reintroduced direct laryngoscopy (autoscopy) in 1895 (Fig. 1.7).39,40 Kirstein, who was in private practice, was visionary in his appreciation of the value of his technique, yet he was fully aware of the potential academic resistance both to a different approach for visualizing the larynx and to a new technology. He therefore called his procedure autoscopy and avoided calling it laryngoscopy. He wisely concluded in the preface of his text, “Of course, many a laryngologist is convinced that the laryngological technique needs no additions; others may think differently. Only the future can decide this question.” Kirstein’s success in precipitating a paradigm shift in endolaryngeal surgery was due to his careful and patient approach to change and to the fact that there was great academic interest in the field of laryngology. This allowed for enough open-minded inspection to embrace the advantages of direct endolaryngeal surgery, which has served us well in the 20th century. In 1895, Kirstein even predicted the enhanced value of autoscopy if it were to be married to improved imaging techniques, which could be provided by magnification and stroboscopy. Killian (1860–1921), who was an academic surgeon, was initially incredulous of Kirstein’s claims regarding direct laryngeal imaging. After viewing Kirstein’s demonstration, however, Killian became absorbed with the new technique. Not to be outdone, Killian perfected rigid bronchoscopy by 1897, thereby demonstrating direct examination of the airway distal to the larynx.41 Killian was destined to make other major contributions to direct laryngoscopy in the early 1900s. All substantive improvements in endoscopic surgery of the larynx during the 20th century have enhanced precision. Increased precision is inevitably linked to better exposure of the operative field and in turn improved visualization. The important innovations enhancing laryngeal exposure had been introduced by 1925. Jackson employed Kirstein’s head and neck position for direct laryngoscopy in the supine position (Fig. 1.8).42 Killian introduced the inverted V laryngoscope blade to conform to the anterior glottal commissure and designed the laryngeal suspension that facilitated bimanual surgery (Fig. 1.9).43–46 Internal distension in the anteroposterior dimension was reintroduced by Haslinger (initially by Babington) with his bivalve laryngoscope and in the mediolateral dimension by Jackson with his laryngostat.47,48 Although previously used by Czermak, external counterpressure was formally described by Brunings (Fig. 1.10).49 All laryngologists use one or more of these concepts; recently, however, Zeitels and Vaughan combined them together while using elevated vector suspension.10 Fig. 1.7 Alfred Kirstein (1863–1922). Most surgeons throughout the world employ torsion-fulcrum laryngoscope holders to maintain the laryngoscope in position for endolaryngeal surgery. They mistakenly refer to this as suspension laryngoscopy. This misconception appears to have evolved from an article in the early 1950s that referred to a gear-powered torsion-fulcrum holder as a suspension device.50 Remarkably, there were no references indexed in this report. Prior authors and scientific reports discussing these types of devices referred to them using terms such as “fulcrum-lift,” “self-retaining,” and “stabilizer.”51–54 Fig. 1.8 Chevalier Jackson (1865–1958). Fig. 1.9 Gustav Killian (1860–1921). The development of torsion laryngoscope holders arose from functional necessity, but their popularity today largely persists due to habit and custom rather than anatomic science and engineering principles. Because Killian’s disciples had difficulty using the suspension gallows on patients who are awake with marginal non-endotracheal anesthesia, they designed the precursors of current laryngoscope holders. Bruning’s laryngoscope system pushed off the larynx, whereas Seiffert’s instrument used the chest wall as a means of support (Figs. 1.10 and 1.11). Remarkably, chest-support torsion-holder systems were used exclusively for spatula laryngoscopes until the late 1940s, at which point they were retrofitted for use with tubular laryngoscopes.50–54 Fig. 1.10 Wilhelm Brunings (1876–1958). The introduction of general endotracheal anesthesia to direct laryngoscopic surgery in the 1960s should have catalyzed a rebirth in the use of true elevated vector suspension.55 Detailed discussions of the forces required for optimal exposure of the larynx advocate the use of a suspension-type device from which the patient is hanging. This information was well known to Strong and Vaughan when they fathered the Boston University Suspension Gallows (Pilling Co., Research Triangle Park, NC).56 Unfortunately, this suspension gallows did not gain wide acceptance and has remained primarily in use among the trainees of two generations of surgeons trained by Strong and Vaughan. Zeitels designed a substantially more robust suspension gallows and academically resurrected the value of true suspension laryngoscopy so that now this philosophy is gaining more widespread adoption.57 Fig. 1.11 Seiffert’s direct laryngoscope. The justification for a return to a suspension gallows is that the most precise endolaryngeal procedure will be accomplished with the widest endoscopic surgical field, which requires the largest laryngoscope that can be placed between the lips and the larynx. Placement of the largest-lumen laryngoscope requires hanging the patient by the soft tissues adjacent to the lower jaw with accompanying general endotracheal anesthesia and muscular paralysis.10,11,58–60 It cannot be achieved by using the maxilla as a fulcrum and the laryngoscope as a lever. Around 1960, the surgical microscope was introduced to endoscopic laryngeal surgery by Scalco and colleagues, Jako, and Kleinsasser.61–64 Jako also designed the first set of microlaryngeal hand instruments.65 Kleinsasser designed hand instrumentation as well and became preeminent in educating surgeons throughout the world in microlaryngoscopic technique.66 At the same time, Priest introduced the concept of general endotracheal anesthesia to laryngoscopy.55 These innovations led to a new era of precision because of the stable magnified surgical field. In the early 1970s, Polanyi worked with Jako, Strong, and Vaughan and coupled the carbon dioxide laser to the surgical microscope.67–72 The laser provided precise hemostatic cutting as well as a delivery system that consisted of a joystick and a foot-pedal. This in turn allowed for precise bimanual surgery under high magnification, which was problematic for those who had difficulty controlling their nondominant hand in a magnified field.73 The aforementioned history reflects the inseparable linkage and interdependence of laryngeal imaging, performing vocal arts, laryngeal physiology, and laryngeal surgery. The laryngeal stroboscope, which was fundamental for understanding and teaching the physiology underlying laryngeal sound production, was introduced initially by Oertel in 1878.74 In this brief communication, Oertel outlined the concept; however, the device functioned poorly due to the lack of a consistent adjustable power source to regulate the rotating perforated disks (Fig. 1.12). His landmark article (1895) described the use of electricity for this purpose, which facilitated the feasibility of the laryngeal stroboscope.75 Furthermore, Oertel ingeniously fitted the stroboscope with a magnifying telescope. There were several incrementally improved rotating disk devices in the early 20th century. However, in the 1950s, laryngeal stroboscopy became substantially more feasible with acoustically synchronized light flashes illustrated by Timcke’s device.76,77 His coauthors, von Leden and Moore, demonstrated that the electronic laryngo-synchro-stroboscope was clinically more valuable compared with the predecessor devices of the prior 50 years.78,79 Hans von Leden’s career and voluminous scientific contributions serve as the foundation for modern phonosurgery, a term he developed (1963).80–83 His seminal contributions have retained their heuristic value through the past 4 decades, and he continues to contribute into the present. Over the past 2 decades, use of an acoustically synchronized laryngeal stroboscope in the management of routine voice disorders has become commonplace and has established the value of laryngeal stroboscopic imaging for any surgeon treating hoarseness and voice disorders. Fig. 1.12 Oertel’s laryngeal stroboscope. Initial illumination for direct laryngoscopy was sunlight.38 As a result of the introduction of electricity, Kirstein used a headlight with his initial autoscope spatula.84 Subsequently, he designed an electrified handle with a proximal incandescent bulb and a prism to direct the light distally. Later, Jackson introduced distal illumination by means of detachable electrified light-carriers.85 Holinger explained that little changed until “Broyles first demonstrated the advantage of fiberoptic light transmission in peroral endoscopes….” during his address as the guest of honor of the American Broncho-Esophagological Association in 1962.86,87 About the same time, the additional light provided by the surgical-microscope enhanced the self-contained illumination of the direct laryngoscopes. There has not been dramatic change since then. A magnified view of the larynx was first reported in 1895 by Oertel in his description of the mirror-guided stroboscope (Fig. 1.12).79 Brunings also used a magnified ocular and was the first to employ magnification to enhance direct laryngoscopy (Fig. 1.10).88 Haslinger designed a tubular laryngoscope with accompanying telescopic magnification. Kahler’s panelectroscope probably had magnification capabilities as well.89 In the early 1950s, Albrecht used a colposcope for magnified indirect vocal fold examination and for photodocumentation of keratosis.90 The first published report of the use of the surgical microscope during laryngoscopy was by Scalco, Shipman, and Tabb in 1960; they employed the Lynch spatula suspension laryngoscope for the task.61,91 The surgical microscope was a monumental innovation for enhancing the precision of endolaryngeal surgery because it provided high-power magnification with a three-dimensional stereoscopic field. Jako (in the United States) and Kleinsasser (in Europe) perfected surgical microlaryngoscopy.62–66 Jako introduced the first set of microlaryngeal hand instruments, and Kleinsasser introduced the 400-mm lens. The latter innovation increased the working distance between the microscope lens and the proximal lumen of the laryngoscope, which facilitated the placement of the long-shafted otologic instruments. Both surgeons designed wide-bore examining tubes to accommodate the optical characteristics of the surgical microscope. Kleinsasser designed his own hand instrumentation and established the foundations for cold-instrument microlaryngoscopic technique, which has recently enjoyed renewed enthusiasm as phonomicrosurgical procedures have increased in popularity. Today, most phonomicrosurgical procedures should be performed under high magnification to ensure maximal preservation of the vocal folds’ layered microstructure (laminae propria and epithelium). Although Nitze introduced the concept of a rigid telescope to view the bladder in 1879, Harold Hopkins initiated the modern era of rigid telescopic imaging in the late 1960s.92 Hopkins was approached by the urologist J.G. Gow asking if Hopkins could develop a better cystoscope, and he invented the rod-lens system to allow better light transmission from the bladder cavity. For the urologist, this provided a 50-fold improvement in the light level. A prototype cystoscope using rod-lenses and a camera was made at Imperial College in 1961. The British and American manufacturers were not interested, but after Hopkins lectured in Dusseldorf in 1963, Karl Storz combined this rod-lens with his cold light. The Storz cystoscope was produced in 1967, and similar rigid fiber endoscopes have since been used throughout the body. In turn, the Hopkins rod has been a key platform technology for laryngoscopic imaging. In 1951, Hopkins developed the idea of using a bundle of optical fibers for transporting an optical image and began experiments in 1952. By 1953, he and his research student N.S. Kapany had produced a coherent fiber bundle in which the fibers were of precisely the same order at the distal and proximal ends.93 Hirschowitz was later to collaborate with C. Wilbur Peters and Lawrence Curtiss to develop a permanent insulated glass coated optical fiber, making it possible to build the first fiberoptic gastroscope in 1957.94 The first commercial gastroscope based on the prototype was produced by American Cystoscope Makers Inc. (Southborough, MA) in 1960, leading on to flexible fiberoptic endoscopes to inspect, biopsy, and intervene throughout the gastrointestinal tract. In 1968, Sawashima and colleagues first reported flexible fiberoptic laryngoscopy.95 This was a profound innovation in laryngology as many patients tolerated flexible transnasal laryngoscopy substantially better than transpharyngeal laryngoscopy with a mirror or rigid telescope. Unfortunately, the optical resolution of flexible laryngoscopic technology is inferior to that of rigid telescopes. This observation is especially dramatic when comparing telescopic with flexible stroboscopic imaging. The recent development of distal-chip technology for flexible laryngoscopes has substantially narrowed this deficit in resolution. With the origin of laryngology (late 1850s), it became clear that the striking images of the larynx and its associated pathology required documentation. However, detailed color photography was not readily available until the late 20th century. This required advances in cameras and print media, illumination, as well as rigid and flexible endoscopes. Laryngoscopic image documentation served to define and describe pathology for identification of disorders, development of management strategies, follow patients’ progress, enhance communication between clinicians, and provide a foundation for education. For the first 25 years of laryngology, image documentation required detailed drawings, which were elegantly depicted in laryngological texts of that era and beyond.25,96,97 The seminal effort in laryngoscopic photography was made by Stein in collaboration with Czermak and perfected by French (Figs. 1.13 and 1.14).98,99 Although photographs of the larynx culminated from a series of elegant innovations, these images lacked optimal resolution, were cumbersome to obtain, and required exceptional equipment and skill. Apart from the obvious constraints of obtaining high-resolution photographic images of a small structure (larynx and vocal folds) in a dark chamber (pharynx), color was an invaluable missing component of the early laryngeal images. Contributions by Garel, Clerf, Holinger, Berci, Yanigasawa, and Benjamin provided the foundation for our current clinical paradigms of easily obtained photo-documentation in the office and the operating theater.100–107 Fig. 1.13 Stein’s laryngeal photography technique. Motion picture imaging of the upper respiratory tract has evolved substantially in the past 70 years. Farnsworth from Bell Laboratories was the first to use a high-speed motion picture camera to film the vocal folds in 1937.108 During this same time period, stroboscopy was being developed for assessing patterns of vocal fold vibration.109–111 The technology for capturing these moving images in a practical way had not yet developed. Brubaker and Holinger in the 1940s developed a motion camera for intraoperative use during bronchoscopy.112 Although this camera produced excellent images, the camera was not widely adopted due to the expense of the device. Von Leden and Moore advanced these research efforts and developed a method of capturing normal and pathologic vocal fold vibration.82,113 The results of this work raised more questions regarding the physiology of vocal fold mechanics. During this time period, cinematography remained a research tool and was impractical for use in clinical laryngology. For the most part, in the 1970s, motion picture filming of vocal fold mechanics remained in the research realm despite multiple investigators developing more effective techniques.114–116 Fig. 1.14 Stein’s laryngeal photographic device. The routine clinical use of color motion picture capturing devices became a reality in the 1980s and 1990s. Yanagisawa and others explored the practical use of videography and photography for laryngeal imaging.117,118 The development of new video cameras, tape-based video systems, and low-cost color printers allowed the established widespread employment of motion pictures in the clinical setting during the past 3 decades. Yanagisawa championed the use of this readily available equipment for several reasons including (1) peer and trainee education, (2) patient education, and (3) treatment evaluation. In the past decade, the development of digital imaging and storage has made it feasible, economical, and practical for the practicing laryngologist to use motion-picture video. These motion pictures are an invaluable education and training instrument and are often incorporated into clinical research. Today, color ultrahigh-speed imaging of vocal fold vibration has become the new research frontier. Despite these substantial advances in motion-picture laryngeal imaging, new ethical issues have arisen. How much information should be captured and at what resolution, as digital storage may have constraints? Are there different considerations for recording office visits compared with recording surgical procedures? Is the information officially a component of the medical record, and do surgeons want to explain/review details of surgery with patients? Laryngeal surgeons and speech-language pathologists must address these issues carefully, wisely, and responsibly while maintaining the highest level of care for their patients. 1. Zeitels SM. Preface. In: Atlas of Phonomicrosurgery and Other Endolaryngeal Procedures for Benign and Malignant Disease. San Diego: Singular; 2001:xi–xii 2. Bozzini P. Der Lichtleiter oder Beschreibung einer einfachen Vorichtung, und ihrer Anwendung zur erleucht ung inherer Hohlen, und Zwischenraume des lebenden animalischen Korpers. Weimar; 1807 3. Avery J. 1844 [Cited in Mackenzie M. The Use of the Laryngoscope in Diseases of the Throat. Philadelphia: Lindsay and Blakiston, 1865:25] 4. Babington BG. Description of the glottiscope. London Medical Gazette 1829;3:555 5. Baumes. Compte Rendu des Travaux de la Societe de Medecine de Lyons 1836–1838;19:18 6. Cagniard de Latour C. [Cited by Fournie: Physiologie de la Voix.] Journal L’Institut 1825;350 7. Liston R. Practical Surgery. London: J. & A. Churchill; 1837:350 8. Selligue AF. 1832 [Cited in Mackenzie M. The Use of the Laryngoscope in Diseases of the Throat. Philadelphia: Lindsay and Blakiston; 1865:17] 9. Senn of Geneva. 1829 [Cited in Mackenzie M. The Use of the Laryngoscope in Diseases of the Throat. Philadelphia: Lindsay and Blakiston; 1865:11] 10. Zeitels SM, Vaughan CW. “External counterpressure” and “internal distention” for optimal laryngoscopic exposure of the anterior glottal commissure. Ann Otol Rhinol Laryngol 1994;103:669–675 11. Zeitels SM. A universal modular glottiscope system: the evolution of a century of design and technique for direct laryngoscopy. Ann Otol Rhinol Laryngol 1999;108(Suppl 179):1–24 12. Garcia M. Observations on the human voice. Proc R Soc Lond 1855;7:397–410 13. Clerf LH. Manuel Garcia’s contribution to laryngology. Bull N Y Acad Med 1956;32:603–611 14. Mackenzie M. The Hygiene of the Vocal Organs, 8th ed. New York: Edgar S. Werner; 1899 15. Mackinlay MS. Garcia the Centenarian and His Times: Being a Memoir of Manuel Garcia’s Life and Labours for the Advancement of Music and Science. New York: D. Appleton and Company; 1908 16. Turc L. On the laryngeal mirror and its mode of employment, with engravings on wood. Zeitschrift der Gesellschaft der Aerzte zu Wien. 1858;26: 401–409 17. Czermak JN. Ueber den Kehlkopfspiegel. Wien Med Wochenschr 1858;8:196–198 18. Stoerk C. On the layrngoscope. Zeitschrift Der Gesellschaft Der Aerzte Ze Wein 1859;46:721–727 19. Lewin G. Allgemeine Medizinische Central-Zeitung 1861;30:654 20. Mackenzie M. The Use of the Laryngoscope in Diseases of the Throat with an Appendix on Rhinoscopy. London: J. & A. Churchill; 1865 21. Mackenzie M. Growths in the Larynx. London, UK: J.& A. Churchill; 1871 22. Mackenzie M. Diseases of the Pharynx, Larynx, and Trachea. New York: William Wood & Co.; 1880 23. Fraenkel B. First healing of a laryngeal cancer taken out through the natural passages. Langenbecks Arch Klin Chir Ver Dtsch Z Chir 1886;12:283–286 24. Elsberg L. Laryngoscopal Medication or the Local Treatment of the Diseases of The Throat, Larynx, and Neighboring Organs, Under Sight. New York: William Wood & Co.; 1864 25. Elsberg L. Laryngoscopal Surgery Illustrated in the Treatment of Morbid Growths within the Larynx. Philadelphia: Collins; 1866 26. Zeitels SM. Jacob Da Silva Solis-Cohen: America’s first head and neck surgeon. Head Neck 1997;19: 342–346 27. Solis-Cohen J. Clinical history of surgical affections of the larynx. Med Rec. 1869;4:244–247 28. Solis-Cohen J. Diseases of the Throat: A Guide to the Diagnosis and Treatment. New York: William Wood; 1872 29. Jackson C. Peroral Endoscopy and Laryngeal Surgery. St. Louis: Laryngoscope Co.; 1915 30. Ehrmann CH. Histoire des Polyps du Larynx. Straasbourg; 1850 31. Trousseau A, Belloc H. Phthisie Laryngie. Paris: Chez and Bailliere; 1837 32. Green H. A Treatise on Diseases of the Air Passages. New York: Wiley and Putnam; 1846 33. Green H. Observations on the Pathology of Croup. New York: John Wiley; 1849 34. Green H. On the subject of the priority in the medication of the larynx and trachea. American Medical Monthly 1854;1:241–257 35. Dr. Horace Green and his method. Harper’s Weekly 1859;5:88–90 36. Donaldson F. The laryngology of Trousseau and Horace Green. Trans Am Laryngol Assoc 1890;12: 10–18 37. Elsberg L. President’s address: laryngology in America. Trans Am Laryngol Assoc 1879;1:30–90 38. Green H. Morbid Growths within the Larynx. In: On the Surgical Treatment of Polypi of the Larynx, and Oedema of the Glottis. New York: G.P. Putnam; 1852 39. Kirstein A. Autoskopie des Larynx und der Trachea (Laryngoscopia directa, Euthyskopie, Besichtigung ohne Spiegel). Archiv fur Laryngologie und Rhinologie 1895;3:156–164 40. Kirstein A. Autoscopy of the Larynx and Trachea (Direct Examination Without Mirror). 1897 41. Killian G. Ueber direkte Bronchoskopie. Munch Med Wochenschr 1898;45:844–847 42. Jackson C. Position of the patient for peroral endoscopy. In: Jackson C, ed. Peroral Endoscopy and Laryngeal Surgery. St. Louis: Laryngoscope Co.; 1915:77–88 43. Killian G. Die Schwebelaryngoskopie. Archiv fur Laryngologie und Rhinologie 1912;26:277–317 44. Killian G. Suspension laryngoscopy and its practical use. J Laryngol Otol 1914;24:337–360 45. Killian G. Suspension laryngoscopy. In: Jackson C, ed. Peroral Endoscopy and Laryngeal Surgery. St. Louis: Laryngoscope Co.; 1915:133–154 46. Killian G. Die Schwebelaryngoskopie und ihre praktische Verwertung. Wien, Austria: Urban & Schwarzenberg; 1920 47. Israel S. The Directoscope of Haslinger in diagnosis and surgery of the larynx. Laryngoscope 1923; 33:945–948 48. Jackson C, Tucker G, Clerf LH. Laryngostasis and the laryngostat. Arch Otolaryngol Head Neck Surg 1925;1:167–169 49. Brunings W. Direct laryngoscopy: autoscopy by counter-pressure. In: Brunings W, ed. Direct Laryn goscopy, Bronchoscopy, and Esophagoscopy. London: Bailliere, Tindall, & Cox; 1912:110–115 50. Lewy RB. Suspension fixation gear power laryngoscopy (with motion pictures). Laryngoscope 1954;64:693–695 51. King NE. Direct laryngoscopy aided by a new laryngoscope “stabilizer.” Arch Otolaryngol Head Neck Surg 1951;53:89–92 52. Roberts SE, Forman FS. Direct laryngoscopy, a simplified technique; an aid to the early detection of laryngeal cancer. Ann Otol Rhinol Laryngol 1948; 57:245–256 53. Roberts SE. A self retaining dual distal lighted laryngoscope with screw driven fulcrum lift. Laryngoscope 1952;62:215–221 54. Sommers KE. Direct laryngoscopy and description of a self-retaining attachment for the laryngoscope. Arch Otolaryngol Head Neck Surg 1952;55:484–488 55. Priest RE, Wesolowski S. Direct laryngoscopy under general anesthesia. Trans Am Acad Ophthalmol Otolaryngol 1960;64:639–648 56. Grundfast KM, Vaughn CW, Strong MS, de Vos P. Suspension microlaryngoscopy in the Boyce position with a new suspension gallows. Ann Otol Rhinol Laryngol 1978;87(4 Pt 1):560–566 57. Zeitels SM, Burns JA, Dailey SH. Suspension laryngoscopy revisited. Ann Otol Rhinol Laryngol 2004; 113:16–22 58. Hochman II, Zeitels SM, Heaton JT. An analysis of the forces and position required for direct laryngoscopic exposure of the anterior vocal folds. Ann Otol Rhinol Laryngol 1998;108:715–724 59. Hochman II, Zeitels SM. Exposure and visualization of the glottis for phonomicrosurgery. Oper Tech Otolaryngol Head Neck Surg 1998;9:192–195 60. Zeitels SM. Premalignant epithelium and microinvasive cancer of the vocal fold: the evolution of phonomicrosurgical management. Laryngoscope 1995;105(3 Pt 2, Suppl 67):1–51 61. Scalco AN, Shipman WF, Tabb HG. Microscopic suspension laryngoscopy. Ann Otol Rhinol Laryngol 1960;69:1134–1138 62. Jako GJ. Microscopic laryngoscopy. Presented at: New England Otolaryngological Society; 1964 63. Jako GJ, Kleinsasser O. Endolaryngeal micro-diagnosis and microsurgery. Presented at: Annual Meeting of the American Medical Association; 1966 64. Kleinsasser O. Mikrochirurgie im Kehlkopf. Arch Ohren Nasen Kehlkopfheilkd 1964;183:428–433 65. Jako GJ. Correspondence documents between Geza Jako and the Stuemar Instrument Company. 1962 66. Kleinsasser O. Microlaryngoscopy and Endolaryngeal Microsurgery. Philadelphia: W.B. Saunders; 1968 67. Polanyi T, Bredermeier HC, Davis TW Jr. CO2 laser for surgical research. Med Biol Eng Comput 1970;8: 548–558 68. Jako GJ. Laser surgery of the vocal cords. An experimental study with carbon dioxide lasers on dogs. Laryngoscope 1972;82:2204–2216 69. Strong MS, Jako GJ. Laser surgery in the larynx. Early clinical experience with continuous CO2 laser. Ann Otol Rhinol Laryngol 1972;81:791–798 70. Strong MS. Laser excision of carcinoma of the larynx. Laryngoscope 1975;85:1286–1289 71. Vaughan CW. Transoral laryngeal surgery using the CO2 laser: laboratory experiments and clinical experience. Laryngoscope 1978;88(9 Pt 1):1399–1420 72. Vaughan CW, Strong MS, Shapshay SM. Treatment of T1 and in situ glottic carcinoma: the transoral approach. Otolaryngol Clin North Am 1980;13:509–513 73. Zeitels SM. Laser versus cold instruments for microlaryngoscopic surgery. Laryngoscope 1996;106(5 Pt 1):545–552 74. Oertel M. Ueber eine neues laryngostroboskopische. Untersuchungsmethode des Kehlkopfes. Centralblatt Medizinischen Wiss 1878;16:81–82 75. Oertel M. Das laryngo-stroboskop und die Laryngo-Stroboskpische Untersuchung. Archiv fur Laryngologie und Rhinologie 1895;3:1–16 76. Timcke R. [Synchronous stroboscopy of the vocal cords in man and analogous sources of sound and the duration of opening.] J Laryngol Rhinol Otol (Stuttg) 1956;35:331–335 77. Timcke R. [Laryngostroboscopy with a new synchronizing stroboscope.] Arch Ohren Nasen Kehlkopfheilkd 1956;169:539–543 78. von Leden H, Moore P, Timcke R. Laryngeal vibrations: measurements of the glottic wave: part III. The pathological larynx. Arch Otolaryngol Head Neck Surg 1960;71:16–35 79. von Leden H. The electronic synchron-stroboscope: its value for the practicing laryngologist. Ann Otol Rhinol Laryngol 1961;70:881–893 80. von Leden H. Plastic surgery of the larynx. Revista Panamerica de Otorrinolaringologia y Broncoesofagologia 1963;1:7–11 81. von Leden H. Surgery for the improvement of vocal function. Revista Panamerica de Otorrinolaringologia y Broncoesofagologia 1969;3:137–143 82. Isshiki N, von Leden H. Hoarseness: aerodynamic studies. Arch Otolaryngol Head Neck Surg 1964; 80:206–213 83. Hirano M, Koike Y, Von Leden H. Maximum phonation time and air usage during phonation. Clinical study. Folia Phoniatr (Basel) 1968;20:185–201 84. Kirstein A. Preface. In: Autoscopy of the Larynx and Trachea (Direct Examination Without Mirror). Philadelphia: F.A. Davis Co.; 1897:vii 85. Jackson C. Instruments. In: Tracheo-Bronchoscopy, Esophagoscopy and Gastroscopy. St. Louis: Laryngoscope Co.; 1907:15–34 86. Holinger PH. Presentation of instruments. Fiber-optic laryngoscopes, bronchoscopes and esophagoscopes. Ann Otol Rhinol Laryngol 1965;74:1164–1167 87. Broyles EN. Address of the guest of honor. Presented at: Annual Meeting of the American Bronchoesophagological Association; 1962 88. Brunings W. Direct Laryngoscopy, Bronchoscopy, and Esophagoscopy. London: Bailliere, Tindall, & Cox; 1912 89. Jackson C. Instruments. In: Jackson C, ed. Peroral Endoscopy and Laryngeal Surgery. St. Louis: Laryngoscope Co.; 1915:11–51 90. Albrecht R. Uber den Wert koloskopischer Untersuchungsmethoden bei Leukoplakien und Carcinomen des Mundes und Kehlkopes. Arch Ohren Nasen Kehlkopfheilkd 1954;165:459–463 91. Lynch RC. Suspension laryngoscopy and its accomplishments. Ann Otol Rhinol Laryngol 1915;24: 429–446 92. Nitze M. Eine neue Beleucht Untersuchungsmethode fur die Harnohre, Harnblase und Rektum. Wien Med Wochenschr 1879;24:649 93. Hopkins HH, Kapany NS. A flexible fiberscope using static scanning. Nature 1954;173:39 94. Hirschowitz BI, Curtiss LE, Peters CW, Pollard HM. Demonstration of a new gastroscope, the fiberscope. Gastroenterology 1958;35:50–53; discussion 51–53 95. Sawashima M, Hirose H. New laryngoscopic technique by use of fiber optics. J Acoust Soc Am 1968; 43:168–169 96. Jackson C, Jackson CL. Cancer of the Larynx. Philadelphia: W.B. Saunders; 1939 97. Turck L. Atlas zur Klinik der Kehlkopfkrankheiten. Wein, Austria: Wilhelm Braumuller; 1866 98. Stein T. Photographing the larynx. Sci Am 1885;21: 179–180 99. French T. Photographing the larynx. Arch Laryngol 1882;3:221–222 100. Garel J. Nouvel appariel perfectionee pour la photographie stereoscopique du larynx sur le vivant. Rev Laryngol Otol Rhinol 1919;40:249–253 101. Clerf LH. Photography of the larynx. Ann Otol Rhinol Laryngol 1925;34:101–107 102. Holinger PH. Endoscopic photography in otolaryngology and bronchoesophagology. Proc Inst Med Chic 1948;17:138 103. Berci G, Caldwell FH. A device to facilitate photography during indirect laryngoscopy. Med Biol Illus 1963;13:169–176 104. Yanagisawa E, Eibling DE, Suzuki M. A simple method of laryngeal photography through the operating microscope. “Macrolens technique.” Ann Otol Rhinol Laryngol 1980;89(6 Pt 1):547–550 105. Yanagisawa E, Yanagisawa R. Laryngeal photography. Otolaryngol Clin North Am 1991;24:999–1022 106. Benjamin B. Technique of laryngeal photography. Ann Otol Rhinol Laryngol 1984;109(Suppl):1–11 107. Benjamin B. Eighteenth Daniel C. Baker, Jr, Memorial Lecture. Art and science of laryngeal photography. Ann Otol Rhinol Laryngol 1993;102(4 Pt 1):271–282 108. Farnsworth D. High-speed motion pictures of the human vocal cords. Bell Laboratories Record 1940;18:203–208 109. Kallen LA. Laryngostrobscopy in the practice of otolaryngology. Arch Otolaryngol Head Neck Surg 1932;16:791–807 110. Perlman HB. Laryngeal stroboscopy. Ann Otol Rhinol Laryngol 1945;54:159–165 111. Powell LS. The laryngostroboscope. Arch Otolaryngol Head Neck Surg 1934;19:708–710 112. Brubaker JD, Holinger PA. An endoscopic motion picture camera for otolaryngology and broncho-esophagology. J Biol Photogr Assoc 1947;15:171–192 113. Von Leden H. Laryngeal physiology. Cinematographic observations. J Laryngol Otol 1960;74:705–712 114. Gould WJ, Jako GJ, Tanabe M. Advances in high speed motion picture photography of the larynx. Trans Am Acad Ophthalmol Otolaryngol 1974;78: ORL276-ORL278 115. Koike Y. High speed photography of the larynx and film data processing. Can J Otolaryngol 1975;4: 800–806 116. Yoshida Y, Hirano M, Nakajima T. A video-tape recording system for laryngo-stroboscopy. J Jpn Bronchoesophagol Soc 1979;30:1–5 117. Yanagisawa E. Videolaryngoscopy using a low cost home video system color camera. J Biol Photogr Assoc 1984;52:9–14 118. Yanagisawa K, Shi JM, Yanagisawa E. Color photography of video images of otolaryngological structures using a 35 mm SLR camera. Laryngoscope 1987; 97(8 Pt 1):992–993
The History of Laryngeal Imaging
 The Origin of Mirror Laryngoscopy and the Field of Laryngology
The Origin of Mirror Laryngoscopy and the Field of Laryngology

 The Origin of and Development of Direct Laryngoscopy and Endolaryngeal Surgery
The Origin of and Development of Direct Laryngoscopy and Endolaryngeal Surgery
 Laryngeal Stroboscopy
Laryngeal Stroboscopy
 Illumination
Illumination
 Magnified Laryngoscopy
Magnified Laryngoscopy
 Rigid Telescopic Laryngoscopy
Rigid Telescopic Laryngoscopy
 Flexible Laryngoscopy
Flexible Laryngoscopy
 Photography of the Larynx
Photography of the Larynx
 Laryngeal Cinematography and High-Speed Imaging
Laryngeal Cinematography and High-Speed Imaging
References
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


