 ver the past four decades, the practice of dermatology has evolved from a subspecialty to a full-fledged specialty, and it is still evolving. Dermatosurgery is almost a superspecialty for most young dermatologists, who use cutting techniques and tools to gain ever better results.
ver the past four decades, the practice of dermatology has evolved from a subspecialty to a full-fledged specialty, and it is still evolving. Dermatosurgery is almost a superspecialty for most young dermatologists, who use cutting techniques and tools to gain ever better results.
Dermatosurgery is the branch of dermatology in which conditions refractory to medical treatment are dealt with and cosmetic improvement of the skin is thus brought about. Skin biopsies, excision of cysts and corns, ear lobe repairs, mole removal, and nail avulsion in cases of onychomycosis are all now being done by dermatosurgeons.
Common dermatosurgery procedures involve electrosurgery (which uses electrically generated heat), cryosurgery, or both (Tables 51.1 and 51.2). The Fugo blade can be of help in managing most of the conditions listed, as demonstrated by the following two case examples.
CASE STUDIES
Case 1: Tuberous Sclerosis
This 14-year-old patient had extensive nodule formation on the face. The diagnosis was tuberous sclerosis.
As a preliminary trial, the patient’s right cheek was partially treated after the injection of local anesthetic. Two weeks later, the patient and his parents thought that the treatment substantially improved his face. There was no scarring and no inflammation. It was then decided to treat the whole of the face under general anesthesia.
Table 51.1. Common Electrosurgery Techniques
| Electrofulguration | Small epidermal lesions such as verruga plana, milia, dermatitis papulosa nigra, and skin tags are removed by electrofulguration with a “fine epilation needle” electrode. In electrofulguration, superficial tissue is charred by sparks from the electrode, without actually touching the tissue. |
| Electrodesiccation | This involves touching the lesion with the electrode with a marginally higher current. Conditions such as seborrheic keratoses, verruca vulgaris, granuloma pyogenicum, cherry angiomas, and senile lentigines are removed by electrodesiccation followed by curettage. |
| Electro-epilation | This is a permanent hairremoval technique useful in hirsutism and cosmetic awareness for facial hair where the hair follicle is destroyed by various electrical techniques such as thermolysis, electrolysis or blend. |
| Benign | Warts |
| Molluscum contagiosum | |
| Cystic acne | |
| Acne scars | |
| Keloids | |
| Granuloma pyogenicum | |
| Prurigo nodularis and mucoid cysts | |
| Xanthelasma and xanthomas | |
| Seborrheic warts | |
| Epidermal nevi | |
| Mucosal lichen planus | |
| Premalignant | Leukoplakia |
| Bowen’s disease | |
| Actinic keratoses | |
| Malignant | Basal-cell carcinoma |
| Lentigo maligna | |
| Squamous-cell carcinoma <3 cm in size |
Surgical Technique
- Use a 600-µm Fugo blade at medium power and high energy setting.
- Depending on the size of the lesions treat them as follows. Touch small lesions and press vertically for a fraction of a second. This is enough to remove them.
- For larger lesions, press the activated tip and rub it in a circular motion from the center outward until the area became flat. Rub the largest lesions from the top and the sides until the skin is flat. During ablation, if a large lesion becomes dry, the plasma energy has lost its effect, so periodically wet the lesion with saline. In our case, it took over an hour to treat a few hundred lesions on the face (Fig. 51.1).
In our case, removing the lesions from all parts of the face was easy, but it was especially so on the nose and nasolabial folds, where there was firm tissue underneath.

Figure 51.1. A large lesion is ablated from the edge inward.
Postoperative Management
Seven days after surgery, our patient’s face was relatively clear. He was vastly better than before and was in high spirits (Figs. 51.2 and 51.3).

Figure 51.2. A part of the right cheek had already been treated with the Fugo blade as a trial. The rest of the face was treated in one sitting. Left: The patient 7 days after treatment. Right: Seven days after treatment left cheek.

Figure 51.3. Part of the face before and 7 days after Fugo blade ablation.
One month later, the condition had improved further. The uneven pigmentation over the face had lessened. However, hundreds of small lesions remained that merited further surgical attention. One large lesion on the right upper eyelid and several lesions on both cheeks had not shrunk and these, too, required additional treatment (Fig. 51.4).
Once again, under general anesthesia, the patient’s entire face was “touched up” as in the previous surgery. Figure 51.5 shows the patient 2 week after subsequent surgery. If the patient wishes greater skin smoothness, additional sessions can be scheduled. But the Fugo blade will not cause burning and scarring, as is common with current classic dermatologic surgical tools.
Case 2: Palmar Corn
The patient was a 65-year-old woman with a large corn on the palm of her hand. The corn was in a prominent position on the palm and caused pain when it was banged or bumped. Under the care of a dermatologist, she had received three intralesional injections of steroid over a 6-month period, but the corn did not resolve. The Fugo plasma blade was used to surgically remove the corn.

Figure 51.4. The patient 1 month after Fugo blade ablation. The number and size of the lesions are greatly reduced.
Lignocaine was injected under and around the lesion. The front of the lesion was sliced with a 100-µm Fugo blade tip and the deeper layers and the walls were removed with a 600-µm Fugo blade tip. The 600-µm tip removed the tissue more slowly and simultaneously stopped any bleeding. Finally, the base and sides were cleaned up a 300-µm tip. The dissection was clean, and no clinically visible damage to healthy tissues occurred. The raw edges were brought together with superficial 80-µm steel sutures (Fig. 51.6). Recovery was uneventful and the sutures fell off after 12 days (Fig. 51.7). One month after surgery the skin at the surgical site appeared normal (Fig. 51.8).
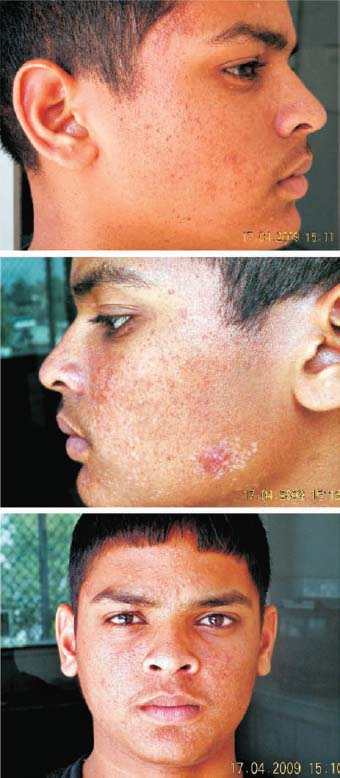
Figure 51.5. Fourteen days after the second extensive touch-up, the patient’s face has improved further. No inflammation, scar formation, or dyspigmentation are present.
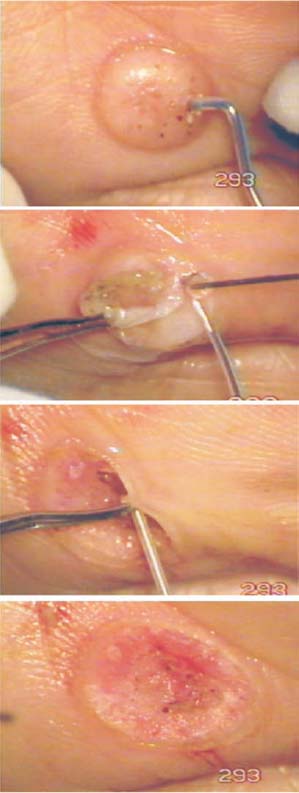
Figure 51.6. A first attempt to remove the corn was made with a 600-µm Fugo blade tip, to see how it would react to ablative energy from a thick tip, but the result was unsatisfactory. The lesion was then sliced with a 100-µm Fugo blade tip. The side walls were cleared with 600-and 300-µm tips.

Figure 51.7. Twelve days after surgery, the operated area still appears rough.
Summary
If a difficult condition like tuberous sclerosis can be successfully treated with a simple ablative tool like the Fugo blade, then it is likely that many common and rare skin conditions can be treated with no risk of inflammation or scarring.
The two cases described above were a challenge to the current armamentarium of dermatosurgeons. The Fugo blade, however, easily corrected these conditions. It appears that dermatosurgery will undergo a revolution with the use of the Fugo blade.

Figure 51.8. One month after surgery, the skin appears near normal.
Suggested Reading
Darke DB, Morgan RF, Cooper PH. Shave excision and dermabrasion for facial angiofibroma in tuberous sclerosis. Ann Plast Surg. 1992;28:377–380.
Dvir E, Hirshowitz B. The use of cryosurgery in treating the fibrous papules of tuberous sclerosis. Ann Plast Surg. 1980;4:158–160.
El-Musa KA, Shehadi RS, Shehadi S. Extensive facial adenoma sebaceum: successful treatment with mechanical dermabrasion: case report. Br J Plast Surg. 2005;58: 1143–1147.
Fischer K, Blain B, Zhang F, et al. Treatment of facial angiofibromas of tuberous sclerosis by shave excision and dermabrasion in a dark-skinned patient. Ann Plast Surg. 2001;46:332–335.
Hori K, Soejima K, Nozaki M, et al. Treatment of facial angiofibroma of tuberous sclerosis using cultured epithelial autografts. Ann Plast Surg. 2006;57:415–417.
Janniger CK, Glodberg DJ. Angiofibromas in tuberous sclerosis: comparison of treatment by carbon dioxide and argon laser. J Dermatol Surg Oncol. 1990;16:317–320.
Pantelis A, Bootz F, Kühnel T. Laser skin resurfacing and fibrin sealing as successful treatment for facial angiofibromas in tuberous sclerosis. HNO. 2007;55:1009–1011.
Pasyk KA, Argenta LC. Argon laser surgery of skin lesions in tuberous sclerosis. Ann Plast Surg. 1988;20:426–433.
Swaroop MR, Nischal KC, Rajesh Gowda CM, et al. Radiofrequency ablation of adenoma sebaceum. J Cutan Aesthet Surg. 2008;1:89–91.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


