 he proliferative fibrotic response of the tenon capsule leads to filtration failure. Keloid formation or “sclerification” of the subconjunctival connective tissue/tenon capsule can happen slowly over weeks or months, or it may take effect within days. The filtering bleb progressively shrinks and intra-ocular pressure increases. Forcing the fluid out of the eye with massage and pressure produces progressively less result and eventually fails. The tenon cyst has a characteristic clinical appearance: elevated localized bleb, prominent surface vessels, and patent internal opening on gonioscopy. Intervention with a needle or injection of fluorouracil or mitomycin C are ways to salvage the failing blebs. But the only recourse is to excise the tenon cyst.
he proliferative fibrotic response of the tenon capsule leads to filtration failure. Keloid formation or “sclerification” of the subconjunctival connective tissue/tenon capsule can happen slowly over weeks or months, or it may take effect within days. The filtering bleb progressively shrinks and intra-ocular pressure increases. Forcing the fluid out of the eye with massage and pressure produces progressively less result and eventually fails. The tenon cyst has a characteristic clinical appearance: elevated localized bleb, prominent surface vessels, and patent internal opening on gonioscopy. Intervention with a needle or injection of fluorouracil or mitomycin C are ways to salvage the failing blebs. But the only recourse is to excise the tenon cyst.
The cause of bleb encapsulation is not known. Male sex, topical corticosteroids, previous argon laser trabeculoplasty, and use of beta-blockers are some potential risk factors for the development of an encapsulated filtering bleb. Glaucoma valves also fail by encapsulation. The incidence of bleb encapsulation has been reported to be anywhere from 3 to 30% in trabeculectomy cases.
The conjunctiva over the cyst is generally, but not always, mobile. Its outer edge may adhere to the conjunctiva, requiring patience when cutting and reflecting the tissue. The cyst may be exposed by making a fornix-based or a limbal-based conjunctival flap. Sclerification and the edge of the tenon cyst extend much further than its apparent size.
Although optimal management of bleb encapsulation has not been defined, we have used the Fugo blade to address tenon cysts as discussed below.
Transconjunctival Restoration of Filtration
We use this approach when it appears that the cyst wall is thin and does not extend beyond the filtration area, the conjunctiva is mobile over it, and tissues appear normal—not inflamed or irritated.
Surgical Technique
- Check the motility of the conjunctiva over the cyst using a plain forceps. Make a mark using gentian violet on the conjunctiva near the proximal edge. When you pull the conjunctiva down, this spot marks the limit that should not be crossed in order to prevent buttonholing.
- Direct and gently press an inactivated 100-µm Fugo blade tip at the intended entry point. Press the foot paddle momentarily, which activates the tip and takes it through the cyst wall. Another indicator of successful breach of the cyst is the entry of cavitation bubbles into the anterior chamber. The outflowing aqueous raises the conjunctiva as a large bleb, and the anterior chamber becomes shallow.
- Use a diamond knife to make a side port incision through which to inject sodium hyaluronate to deepen the anterior chamber. Now the anterior chamber is not leaking, and a large conjunctival bleb now exists, with a hole that was made along with the transconjunctival track. At this stage it is easy to pass the ablation tip through the hole, enter under the conjunctiva, and make additional openings in the cyst.
- The conjunctival hole may or may not be sutured (Fig. 32.1).
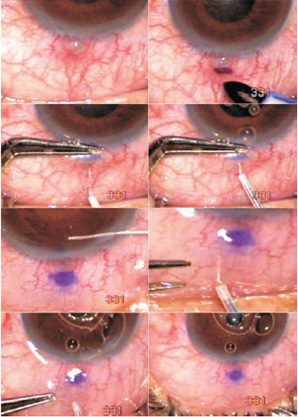
Figure 32.1. A small tenon cyst developed after microtrack filtration. A mark is made with gentian violet to prevent counterpuncture when the mobile conjunctiva is displaced downward and the cyst is opened transconjunctivally with a 100-µm Fugo blade tip. The conjunctiva is ballooned up with the outflowing aqueous. The anterior chamber is deepened with sodium hyaluronate through a 0.75-mm corneal pocket incision. One or more additional openings are made in the tenon cyst through the conjunctival opening.
Cyst Removal after Reflecting the Conjunctiva
This approach can be used to manage large cysts with thick walls. The conjunctival flap may be fornixbased or limbus-based. Dissection is not easy if the cyst is firmly adhered to the conjunctiva. In such cases, part or all of the conjunctiva over the cyst must be sacrificed. When the cyst is fully exposed, it is found to be much wider than it appeared before surgery.
Surgical Technique
- Use a 300- or 600-µm Fugo tip at medium power setting to ablate the cyst, starting from the periphery and progressing toward the center. When the cyst wall is breached, the aqueous flows outward and the eye becomes soft.
- Remove the last portion of the cyst wall, or it may be left as a partial cover for the filtration track.
- Suture the conjunctiva (Fig. 32.2).
In a fornix-based approach, greater risk of losing the conjunctiva over the cyst exists. In a limbus-based approach, dissection is done from underneath, and the anterior wall of the cyst may be left alone or merely thinned, but not breached, thereby preserving the conjunctiva over it. However, one clumsy move or an attempt to ablate a little more will create a buttonhole, which then necessitates suturing both at the limbus and toward the fornix.

Figure 32.2. A case of transciliary filtration. The cyst is apparently small but turns out to be much bigger when it is exposed. All of the cyst wall is ablated using a 600-µm Fugo blade tip, leaving a small loose leaking cap (as seen by the flow of trypan blue) over the filtering track. The conjunctiva is pulled down and sutured to the limbus.
Subconjunctival Approach for Subtotal Tenon Cyst Ablation
The subtotal destruction of the tenon cyst wall and its base is relatively less traumatic than the open approach. No hemorrhaging occurs, and ablation debris is washed away with copious irrigation under the conjunctiva. We have tried to use a vitrector to ablate tenon capsule; two ports were made in the conjunctiva, one for irrigation and the other for the vitrectomy/tenonectomy tip. But only very thinwalled cysts could be managed partially, and a high risk of bleeding and conjunctival buttonholing existed.
A special Fugo blade tip is used for the subconjunctival approach. The tip has a 300-µm filament surrounded by a thick sleeve of nonstick material, so that the tip is naked for about 0.125 mm on the front and about 0.25 mm on the underside. When the tip is moved in the process of ablation, it will not threaten overlying conjunctiva.
Surgical Technique
- Make a conjunctival hole with a plasma blade with a 100-µm tip, near the limbus about 3 mm from the edge of the cyst (Fig. 32.3).
- Balloon the conjunctiva around the cyst with saline, followed by visco-elastic material. Injecting the visco-elastic material stretches the conjunctival hole.
- Insert the tenon ablation tip under the conjunctiva until it reaches the edge of the cyst.
- Use medium power and medium energy for ablation. First, ablate the nearest wall, releasing the blocked aqueous and further raising the conjunctival bleb. Make a stab incision in the anterior chamber and inject visco-elastic material to halt further aqueous flow under the conjunctiva. Reintroduce the ablation tip and move it from the limbal side upward to open up the tenon cyst as much as possible. In this process, the side walls and the scleral side of the cyst are destroyed, while the anterior wall and the conjunctiva over it are saved from ablation. If necessary, inject more visco-elastic material under the conjunctiva, so that the ablation tip poses no threat of counterpuncture.
- Depending on the situation, you may approach the tenon cyst from one or two additional conjunctival openings: one from the opposite side and one from above. You may inject the area of the cyst with 0.04% mitomycin for 4 to 5 minutes and then rinse it copiously with saline. Its entry into the anterior chamber is blocked by the sodium hyaluronate inside the chamber.
- Close the conjunctival holes with sutures, or you may leave them alone to close naturally (Fig. 32.4).
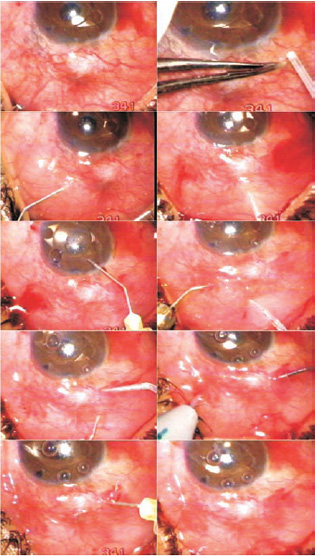
Figure 32.3. Three conjunctival holes are made with a 100-µm Fugo blade tip, and the conjunctiva is raised with saline and sodium hyaluronate. The cyst is first breached with an ablation tip introduced through the upper opening. The anterior chamber is filled with sodium hyaluronate, injected through a stab incision. The ablation process is carried out through all the three conjunctiva, while the conjunctiva is kept raised by continued irrigation under it. The process is considered complete when a cannula introduced from the side can be moved freely up and down. Mitomycin 0.04% was irrigated under the cyst and rinsed by irrigation after 4 minutes.
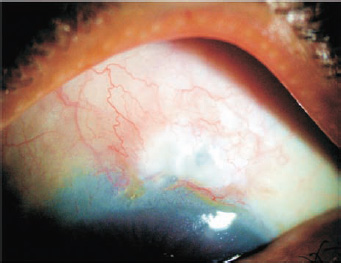
Figure 32.4. The same patient as in Figure 32.3, 2 months after surgery.
Tenon Cyst over the Glaucoma Valve
A frequent cause of glaucoma valve failure is the formation of a thick tenon cyst over it, but these cysts are easy to manage. Make a bold 100-µm tip incision over the valve, going through the conjunctiva and the cyst wall. The cyst wall usually does not adhere to the conjunctiva or to the valve. Excise a strip of the cyst wall, including the part over the edge of the valve, with the same Fugo blade tip, exposing the valve; the restrained aqueous flows out from under the edge of the valve. Nothing more needs to be done. Suture the conjunctiva (Fig. 32.5).

Figure 32.5. A failed glaucoma valve due to tenon cyst. Incision in the conjunctiva is followed by excision of a strip of the tenon cyst that also exposes the edge of the valve. The conjunctiva is closed with sutures.
Summary
The Fugo blade is a useful tool to manage all cases of tenon cysts. The size and thickness of the cyst wall are immaterial. Either an open or a closed approach can be used. Bloodless, nondissective destruction/ablation of the tenon cyst through tiny holes in the conjunctiva guarantees quick recovery. Injection of antimitotic agents or application of pressure to the eyeball to squeeze out the aqueous fluid is not needed.
Suggested Reading
Gutiérrez-Díaz E, Montero-Rodríguez M, Julve San Martín A, et al. [Incidence of encapsulated bleb after filtering surgery.] [Article in Spanish.] Arch Soc Esp Oftalmol. 2001; 76:279–284.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


